
Abstract
Purpose:
Total hip arthroplasty (THA) after failed osteosynthesis for proximal femoral fractures is associated with higher revision rates, particularly for dislocation. The purpose of this study was to report our results with THA after failed osteosynthesis within a treatment period of 10 years.
Methods:
A retrospective cohort study including 80 consecutive patients was conducted. After a minimum follow-up of 1 year, we evaluated revision for any cause including dislocation, outcome, and mortality.
Results:
We performed 48 THAs with standard components only and 32 THAs with revision implants. Routinely, a 36-mm femoral head was used, and trochanteric fixation was performed in one-third of the cases. Total revision rate for any cause was 21%, which included six infections, six periprosthetic fractures, and five hematomas. One hip dislocation was also treated. Treatment with uncemented revision stem revealed significantly higher number of revisions—compared to standard cemented or uncemented stem. The mortality rate after 1 year was 9%, and the mean Parker score at follow-up was 6.6 (range: 0−9).
Conclusions:
THA was associated with an increased surgical revision rate, but hip dislocation was documented only once. In most cases, a standard implant with a large 36-mm femoral head size was sufficient. Uncemented revision stem revealed significantly higher number of revisions—compared to standard cemented or uncemented stem. One-year mortality was lower than expected.
Introduction
Surgical treatment of proximal femoral fractures predominantly occurs in geriatric and therefore common in multimorbid patients. 1,2 A variety of hardware, particularly the dynamic hip screw and intramedullary devices such as the proximal femoral nail (DePuy Synthes, Umkirch, Germany) or Gamma nail (Stryker, Freiburg/Stetten, Germany), are available for treatment. 1 –4 Research have reported conflicting results, with no device demonstrating clear benefit. 3 –8 Moreover, treatment of proximal femoral fracture is associated with high complication rates (up to 35%) due to multifactorial and often patient-related factors as well as fracture etiology. 3,9,10 Osteosynthesis failure is considered a major complication, which necessitates changing or replacing the device to prevent further complications. In the latter one, total hip arthroplasty (THA) or hemiarthroplasty is necessary as a “salvage” procedure to maintain hip joint mobility and stability. 11,12 For that reason, the surgeon must not only remove the failed fixation first but also adapt the acetabular and femoral components of the endoprosthesis because of the more pathological situs, for example, an unstable trochanteric fragment or acetabular defect zone. 13 Therefore, THA after failed osteosynthesis has also been reported with both higher complication and dislocation rates. 10,14,15 However, few clinical studies have investigated this topic and they have been characterized by small samples 15 ; preselection of consecutive patients, for example, exclusion of dementia 12 ; and higher loss to follow-up because of morbidity or mortality. 12,14 –17
The primary end point of this retrospective mono-center study was to determine the (1) incidence of failed osteosynthesis, (2) rate of surgical revision after THA, and (3) postoperative mortality rate after THA. The secondary aim was to identify variables influencing surgical revision and mortality.
Patients and methods
We conducted this retrospective mono-center cohort study using an internal clinic database for all surgically treated proximal femoral fractures (fracture line up to 5 cm distal to the minor trochanteric). Institutional review board approval was obtained, and all patients or relatives contacted via telephone provided informed consent for data review and collection.
The following exclusion criteria were applied: fractures with multiple segments, histologically confirmed pathological femoral fractures (with the exception of fractures due to osteoporosis), and patient age <18 years. We identified a total of 54 consecutive patients treated between January 1, 2006 and December 31, 2015 who met the following criteria: (a) failed osteosynthesis, (b) undergoing THA, and (c) within one-stage procedure. Patients with failed osteosynthesis due to infection were excluded. We further included 26 patients referred to the clinic for the treatment of existing failed osteosynthesis by using the same inclusion criteria. First, demographic variables (Table 1) and information on postoperative surgical revision for any cause including closed reduction for dislocation were evaluated. At least 1-year postoperatively, telephone interviews with surviving patients were conducted to assess any further complications, current mobility status using the Parker score, 18 and subjective satisfaction with THA by using a dichotomous scale—satisfied or unsatisfied. Missing data for deceased or demented patients were collected from relatives or general practitioners.
Baseline data for the 80 study patients in relation to revision surgery for any cause and 1-year mortality.a

BMI: body mass index; DHS: dynamic hip screw; PFN: proximal femoral nail; THA: total hip arthroplasty.
aThe only one statistical significant variable was THA with revision stem compared to standard stem with regard to postoperative surgical revision.
Definitions
Cutout by screw or blade involved medio-central or generally cephalad perforation of the device from the femoral head. 19 Postoperative infection was defined as a fistula connected to the implant and/or a minimum of two positive intraoperative tissue samples. 20 We primarily treated acute infection with debridement, irrigation, head and liner exchange, and antibiotics (based on antibiogram) for 4−6 weeks. Failed infection control was treated by resection arthroplasty. A dislocation was defined as complete femoral head disconnection from the cup, regardless of direction. Dementia was defined as impaired cognition in patients receiving disability/legal assistance.
Surgical procedure
All cases were exclusively treated by consultant surgeons in an operating room with laminar air flow. The surgery was performed in the supine position until 2011 and in the lateral position thereafter. A posterior approach was never used. Normal skin conditions were recorded in all cases; notably, no fistulas were observed. Infections at the time of THA were excluded in all cases using laboratory and bacteriological tests, based on deep tissue samples routinely collected during THA. Immediately before skin incision, all patients received antibiotic by a single-dose intravenous cefazolin 1.5 g.
The following surgical steps were taken. Initially, the fascia was cut longitudinally and followed by complete hardware removal. The hip joint was prepared by a Watson-Jones’ or Bauer et al.’s approach, according to the surgeon’s preference. 21,22 Selection of acetabular cup or femoral stem components was also based on the surgeon’s discretion and experience, along with bone quality and patient age. Generally, uncemented standard components were used for younger patients (< 70 years), and cemented standard components including hybrid technique were applied in elderly patients (Table 2). The cemented femoral components were implanted with a so-called “third-generation” technique (plug femur, pulsed lavage, and cement preparation in vacuum with retrograde insertion). Moreover, nonmodular, uncemented, and tapered stems were also applied (Table 2). In cases involving an additional unstable trochanteric fragment, fixation was performed using one or two wires or a hook plate at the surgeon’s discretion. The positions of the components were intraoperatively controlled by an X-ray image converter. According to our standard protocol, all patients received an intra-articular drain and subcutaneous suction for 48 h. Patients received physiotherapy on crutches with full weight-bearing for cemented components and partial weight-bearing (6 weeks; 40 lb) for uncemented or revision stem.
Components used for the total study cohort of 80 patients.a

aAll used implants were produced by Zimmer® (Warsaw, Indiana, USA).
Statistical analysis
Statistical analyses were performed using SPSS software (SPSS Inc., Chicago, Illinois, USA) for Windows, Version 24.0. Continuous variables were presented as mean or median values. Categorical and/or nominal data were specified as absolute and relative frequencies. Survival analysis was performed using the Kaplan–Meier analysis. 23 Categorical data were analyzed using the χ2 test and Fisher’s exact test. All statistical tests were two sided, with p values < 0.05 considered statistically significant.
Results
Basic data analysis
Based on the defined criteria, 1314 consecutive osteosynthesis procedures in patients with proximal femoral fractures were performed in our clinic over a 10-year period. During the same period, 63 osteosynthesis failures were reported, for an incidence of 4.8% in our evaluated population. THA was performed in 54 of these patients, and 26 additional patients with failed osteosynthesis were referred to our clinic from external facilities (see flow chart; Figure 1). Thus, 80 consecutive patients were considered for further study analyses.

Flow chart of patient enrollment. DHS: dynamic hip screw; PFN: proximal femoral nail; THA: total hip arthroplasty.
Descriptive data
Mean age at the time of osteosynthesis was 74.1 years (range: 22−95). Demographic variables are summarized in Table 1. The most common reason for failed osteosynthesis was cutout (50 of 80; 68%), followed by nonunion (n = 9), fracture/dislocation (n = 7), head necrosis (n = 7), post-traumatic arthritis (n = 3), and others (n = 4). The median interval between osteosynthesis and THA was 75 days (range: 2−914).
The components used for THA are presented in Table 2. Excluding five cases with a dual mobility bearing, all patients received a large 36-mm femoral head. Forty-eight patients underwent THA with standard components only (Figure 2), whereas 32 patients received one (cup or stem) or two (cup and stem) revision components (Table 2). Twenty-nine patients received a nonmodular, uncemented revision stem (Table 2; Figure 3). Additional trochanteric fixation with wires or hook plate for unstable trochanteric major was performed in 27 (34%) of 80 patients. Median operation time, estimated blood loss, and length of stay in the hospital ward (excluding admission and discharge days) were 125 min (range: 60−285), 900 ml (range: 300−3500), and 13 days, respectively.
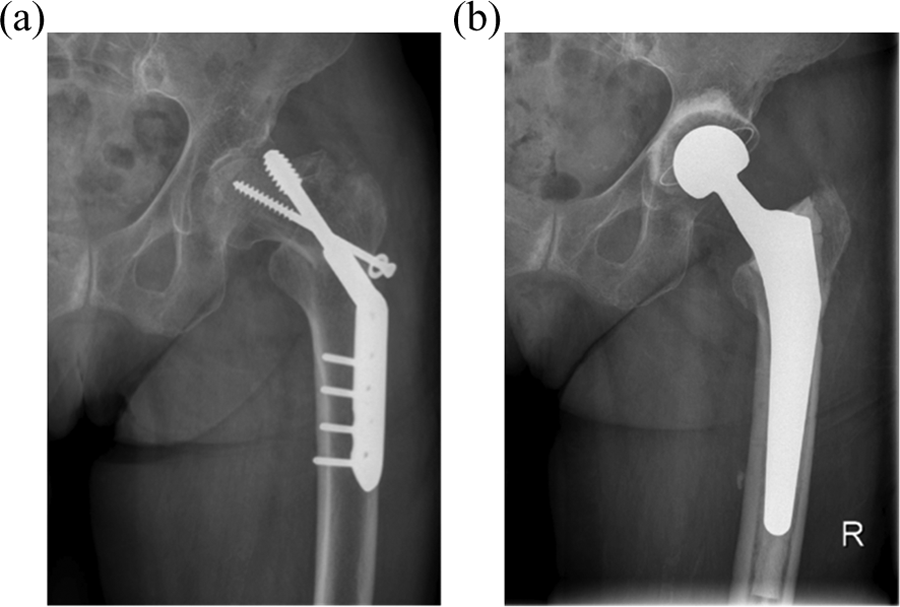
(a) Female patient, aged 80 years, treated with internal osteosynthesis for intertrochanteric fracture. Radiograph demonstrating cranial cutout of DHS on the left side 12 days postoperatively. (b) Same patient. Radiograph showing revision of failed osteosynthesis with complete removal of the DHS and THA with standard cemented components. DHS: dynamic hip screw; THA: total hip arthroplasty.

(a) Male patient, aged 70 years, treated with internal osteosynthesis for intertrochanteric fracture. Radiograph demonstrating medial cutout of the PFN blade on the right side. (b) Same patient. Radiograph showing revision of failed osteosynthesis with complete removal of the PFN and THA with a standard uncemented cup and uncemented revision stem. Early infection was treated 14 days postoperatively with one debridement, including head and liner replacement. PFN: proximal femoral nail; THA: total hip arthroplasty.
Complications
Seventeen of 80 patients (21%) underwent one or more surgical revisions, including five acute infections, five hematomas, five periprosthetic femoral fractures (PPFs), one early infection followed by PPF, and one dislocation. Thirteen patients underwent primary revision within 3 weeks postsurgery. None of the five patients with hematoma required a second revision, and all index components were still in situ at follow-up. Primary revision for acute infection was also initiated within 3 weeks postsurgery, and no late infection (after 6 weeks) was documented. By contrast, 5 of 6 PPFs occurred considerably later (2−56 months) after a fall from standing height and were treated with osteosynthesis and/or stem replacement. One PPF occurred intraoperatively during implantation of a revision stem. Only one reported dislocation initially required an open reduction (including modular head exchange) and subsequently a closed reduction to restore hip joint stability. At 13-month postoperative follow-up, this patient was mobile with a frame. No more revisions were reported or documented. Thus, failure of THA for revision of any cause was documented in 6 of 80 patients (7.5%): 3 with modular head and liner replacement and 3 with resection arthroplasty for infection control.
Follow-up
At follow-up after a mean period of 5.5 years postsurgery (range: 1−10 for the total samples), 28 of 80 patients (35%) were deceased (Figure 4). Mortality at 30 days, 6 months, and 12 months was 5%, 7%, and 9% (7 of 80), respectively. Telephone interviews with relatives of all deceased patients revealed that none had received surgical interventions other than those already recorded. Therefore, 73 of 80 (93.5%) of the THAs were in situ at the time of follow-up or death.

Survival analysis with Kaplan–Meier curve depicting the censored data. After a mean follow-up period of 5.5 years, 65% of the patients were still alive.
After a mean period of 4.6 years (range: 1−9) postsurgery, 52 alive patients were available for follow-up. The interview revealed a mobility status with a mean Parker score of 6.6 (range: 0−9) and 23 patients achieved maximum scores. Subjectively, 49 of 52 patients were satisfied with the THA and only 3 were unsatisfied because of persisting hip pain.
Statistical results
Descriptive data were divided into dichotomous and trichotomous variables for statistical analysis. The influence of 13 variables (Table 1) on revision for any cause or 1-year mortality was statistically tested. The analysis revealed that surgical revision rate was significantly higher when a revision stem was used: The revision rate was 34.5% (10 of 29) because of 4 infections, 4 hematomas, and 2 PPFs. Other variables were not associated with higher revision rate. Moreover, no variables were found to significantly influence 1-year mortality, perhaps due to the low number of cases (n = 7). The 1-year mortality rate of the 17 patients who underwent revision was not significantly increased compared to that of patients without revision (Table 1).
Discussion
Despite THA as a “salvage” procedure for failed osteosynthesis after proximal femoral fractures represents a surgical challenge, 13,15,24 it is not recommended to perform re-osteosynthesis after failed internal fixation: A multicenter study demonstrating high complication rates following re-osteosynthesis recommended THA as the only valid salvage procedure for complications after intertrochanteric fracture treatment. 11
This study had several strengths. First, the inclusion and exclusion criteria were precisely defined and the frequency of treated patients was high. Second, the incidence and prevalence of failed osteosynthesis in the study group is clearly described (Figure 1), with an incidence of 4.8% within 10 years of enrollment. However, the incidence is likely to be underestimated, because we have excluded patients.
The rate of cutout in our cohort was higher than that of a multicenter study that enrolled only 57 cutouts among 4109 total intertrochanteric fracture cases treated by nailing, but cases were likely missing or undetected. 11 However, the reasons for cutout and other causes of osteosynthesis failure were not the target of the present study and not evaluated further. Third, no patients were lost to follow-up with regard to the end points of the study.
Our demographic data were similar to those of other studies 12,17,25 and ASA classification 26 revealed that the geriatric patients had comorbidities. In addition to the ASA score, we also assessed dementia or cognitive impairment. Our statistical analysis demonstrated no difference in revision rate or 1-year mortality in patients with dementia when compared to those without.
Treatment of failed osteosynthesis predominantly (48 of 80; 60%) included standard cemented and uncemented components as described before. The selection of surgical technique and components was at the surgeon’s discretion and depended on the quality of bone substance. Specific revision components must be available in the operating room but do not necessarily represent the primary option. 14,24 Thakur et al. evaluated 15 patients consistently treated with revision stems, but without clarifying how many other patients were treated using a standard stem. 16 Haidukewych and Berry used a standard prosthesis in only 9 of 60 arthroplasties. 13
Despite the high rate of standard components, 29 revision stems were also used at the surgeon’s preference, but the use of an uncemented revision stem was associated with a significantly higher revision rate. No other influencing factors were detected in our analysis; therefore, with the exception of subtrochanteric fractures, we no longer recommend routine use of a revision stem.
The incidence of PPF in our cohort was 7.5% and higher than that in similar studies. 14,24 However, five of six PPFs occurred after a fall from standing height, raising the question of whether these events represent a complication per se or a new entity. We did not find significant evidence of a relation between PPF and preexisting screw holes of the initial hardware within the proximal femoral cortex in a present study of peri-implant femoral fractures 8 but cannot exclude this possibility from the present study because of the small number of cases.
The acute postoperative infection rate was increased (6 of 80; 7.5%), but no late infection was observed until follow-up. All infections were related to positive microbiological findings. Nevertheless, three of six infections were controlled by surgical debridement without THA failure.
Some research reported higher dislocation rates. 14,15,17,24,27 It remains unclear to what extent dislocation is related to surgical approach and/or femoral head size: Exaltacion et al. found a 7% dislocation rate in only 20 patients treated by a posterior approach, with unspecified femoral head size. 17 Two recent studies with larger cohort reported dislocation rates of 3.4% and 4.9%, respectively. Using a femoral head size of 28 mm, Enocson et al. found no difference in total complication rates between antero- and posterolateral approaches but did not specifically analyze dislocation. 24 Archibeck et al. analyzed a large population (n = 102) but provided no information on surgical approach or femoral head size. 14 Using routinely a larger-diameter head size (36 mm), we observed only one dislocation. Haidukewych and Berry similarly reported one dislocation in 60 patients. 13 The beneficial impact of larger diameter head sizes for protection of dislocation has already been demonstrated. 25,27 Importantly, additional fixation must be established in patients with unstable trochanteric major to avoid such complications. Accordingly, trochanteric fragment fixation with wires or hook plates was necessary in one-third of cases, with no associated increase in revision rate. Additionally, the study revealed the same revision rate for femoral neck and intertrochanteric fracture, despite THA of failed intertrochanteric fractures being considered more technically demanding. 25 Nevertheless, the surgical revision rate was 21%, including five patients with hematoma, which is higher than a similar study. 14 However, revision of hematoma was not associated with the failure of THA. The authors like to emphasize that revision of hematomas is often neglected without giving reasons within national THA registries. 28
The postoperative mortality rate in the first year was 9% due to geriatric patient comorbidities and not the treatment itself. Thus, THA was associated with a lower than expected 1-year mortality compared to the results of Müller-Mai et al. who reported 1-year mortality of 26.9% among 7905 patients who underwent initial surgical treatment for proximal femoral fracture. 1 This difference may be related to the lower average age (74.3 vs. 81.5 years). Recent clinical studies provided no mortality data, 14,17 –24 although one research found a similarly low mortality rate of 10% (6 of 60 patients). 13 A total of 52 (65%) of 80 patients were finally available for follow-up. The Parker score demonstrated limited mobility (mean score: 6.6; range: 0−9). Nevertheless, 23 of 52 patients achieved the maximum score (i.e. unlimited indoor and outdoor mobility). However, the activity identified by telephone interviews is more representative for patient morbidity rather than hip joint status per se.
Finally, the retrospective study has several limitations: The level of evidence is low (level 4), and the results reflect no long-term data. Moreover, further THA-related complications and revisions may occur in the future, particularly aseptic loosening or PPF. Femoral densitometry data were available in only few cases, and no information on previous osteoporosis therapy, for example, bisphosphonate, was available. No clinical and/or radiological follow-up was performed. Thus, radiological evidence on stem subsidence, potential aseptic loosening, or heterotopic ossifications was not available as well as no clinical examination based on a valid questionnaire, for example, Harris hip score, was conducted.
Conclusion
In this retrospective cohort study, THA after failed osteosynthesis for treatment of proximal femoral fractures was associated with an increased surgical revision rate, but dislocation was documented only once. In most cases, a standard implant with a large 36-mm femoral head size was sufficient. However, uncemented revision stem demonstrated significantly higher number of revisions—compared to standard cemented or uncemented stem. One-year mortality was lower than expected, and 94% of the THAs are still in situ until patient’s death or last follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.