
Abstract
Purpose:
To measure the intracompartmental pressures surrounding tibial fractures not exhibiting any clinical evidence of compartment syndrome. Our hypothesis was that pressures often exceed the recommended threshold of fasciotomy despite the absence of compartment syndrome, and hence diagnosis based on pressure measurements alone is unreliable.
Methods:
Thirteen consecutive patients with closed tibial shaft fractures without clinical suspicion of compartment syndrome, and who were planned for intramedullary nailing, were prospectively enrolled. Compartment pressures (P) in all four compartments of the affected leg were measured at the start of surgery and immediately after tibial reaming, and differential pressures (delta P) were calculated based on the diastolic blood pressure prior to induction of anaesthesia.
Results:
No patients required reoperation in the post-operative period, as a result of an undiagnosed compartment syndrome. Using commonly quoted threshold pressure criteria, 62% (using P > 30 mmHg) and 23% of patients (using delta P < 30 mmHg) have been incorrectly diagnosed with compartment syndrome.
Conclusions:
We conclude that raised compartment pressures are frequently seen in patients with tibial shaft fractures; but in most cases, it does not equate to the presence of compartment syndrome. Diagnosis of compartment syndrome based on intracompartmental pressure measurements alone may result in unnecessary fasciotomies in a sizeable number of patients. Compartment syndrome remains a clinical diagnosis, and one which always needs to be considered when managing tibial fractures.
Introduction
Acute compartment syndrome is a true orthopaedic emergency. If not promptly treated, it may result in irreversible ischaemic tissue damage within 6 h, potentially resulting in amputation or significant loss of function of the extremity. 1 –5 Because of the grave medico-legal implications of a missed or delayed diagnosis, the timely and accurate diagnosis of compartment syndrome remains a great clinical concern. 6 –8 Underdiagnosing the condition runs the risk of severe limb morbidity or even mortality, while overdiagnosis leads to unnecessary fasciotomies, with its own associated risks of wound infection and other soft tissue complications.
The diagnosis of acute compartment syndrome is classically made based on clinical symptoms and signs alone, 9 –11 which are to some extent subjective and susceptible to interobserver variability. 12 The use of intracompartmental pressure measurements is one way of introducing objectivity into the assessment and is especially useful for patients who are unable to cooperate with a full clinical examination (e.g. polytrauma, alcoholic intoxication). Commonly used criteria for decompression include an absolute pressure above 30 mmHg (Mubarak et al.; 13 Blick et al.; 1 and Hargens et al. 14 ) or a differential pressure (delta P) below 30 mmHg (Whitesides et al. 15 and McQueen and Court-Brown 16 ). While numerous studies have been performed investigating the utility of the various threshold pressures in diagnosing compartment syndrome, 13 –22 fewer studies have looked at the rates of overdiagnosis of the condition based on pressure measurements.
The purpose of this study was to measure the intracompartmental pressures surrounding tibial fractures, which did not exhibit any clinical evidence of compartment syndrome. Our hypothesis was that pressures often exceed the recommended threshold of fasciotomy despite the absence of compartment syndrome, and hence diagnosis based on pressure measurements alone is unreliable.
Materials and methods
Institutional review board ethics approval was granted for this study. Over a 6-month period in 2015–2016, we prospectively recruited all patients aged 18 to 65 admitted to our hospital with a closed tibial shaft fracture, who were planned for surgical fixation with an intramedullary nail and who did not have any clinical findings suspicious of compartment syndrome. Exclusion criteria included age less than 18 or above 65, patients not planned for operative intervention, a confirmed or suspected clinical diagnosis of acute compartment syndrome, altered mental state for any reason, open fractures and fractures within 5 cm of the articular surface. Informed consent was obtained prior to enrolment.
A total of 28 consecutive adult patients fulfilled the inclusion criteria within the study recruitment period. Of these, four patients were excluded due to concomitant head injuries with decreased conscious level, one due to alcohol intoxication with altered mentation, one due to fracture extending to within 5 cm of the distal articular surface, and a further nine did not consent to participation in the study, leaving 13 patients in the final study cohort.
Timing of the operation was determined by the clinical state of the patient and availability of operating theatre. All measurements of compartment pressures were conducted in the operating theatre at the time of surgery. Patients were anaesthetized (general or regional anaesthesia) as per standard practice for intramedullary nailing of closed tibial shaft fractures, and compartment pressure measurements were performed only after successful induction of anaesthesia to ensure that no pain was experienced by the patient during the measurement.
Compartment pressures (P) were measured using a Stryker Intra-Compartmental Pressure Monitor (Stryker Surgical, Kalamazoo, Michigan, USA). Radiographs of the injured leg were reviewed prior to the start of the procedure to identify the fracture site, and the sites for measurement of the four compartments (anterior, lateral, superficial and deep posterior) were marked within 5 cm of the fracture site. Cleaning and draping of the leg was performed as per standard surgical procedure, and compartment pressure measurements were performed under aseptic technique. Two sets of four readings were obtained – one set immediately after induction, and one more after the completion of reaming and before nail insertion. All measurements were taken with the leg flat on the operating table and the knee extended to control for variations in compartment pressures due to positioning. The diastolic blood pressure just prior to induction of anaesthesia was recorded for calculation of differential pressures (delta P) using the following formula:

Standard post-operative care was administered after surgery, and all patients were monitored as inpatient for the development of compartment syndrome as well as other complications. Serial examinations of the operated limb were performed and documented.
Statistical significance was assessed through a paired t test using the SPSS system Version 22.
Results
The study included 13 patients, 12 men and 1 woman, with a median age of 37 (25–64) years and injury characteristics as summarized in Table 1. Ten fractures were operated on within 48 h of injury, with one surgery delayed until post-injury day 10 due to concomitant injuries that required more urgent surgery. The average length of hospitalization was 4.5 days, and no patient developed signs or symptoms of compartment syndrome or required reoperation for a missed diagnosis of compartment syndrome during the post-operative period.
Patient characteristics.

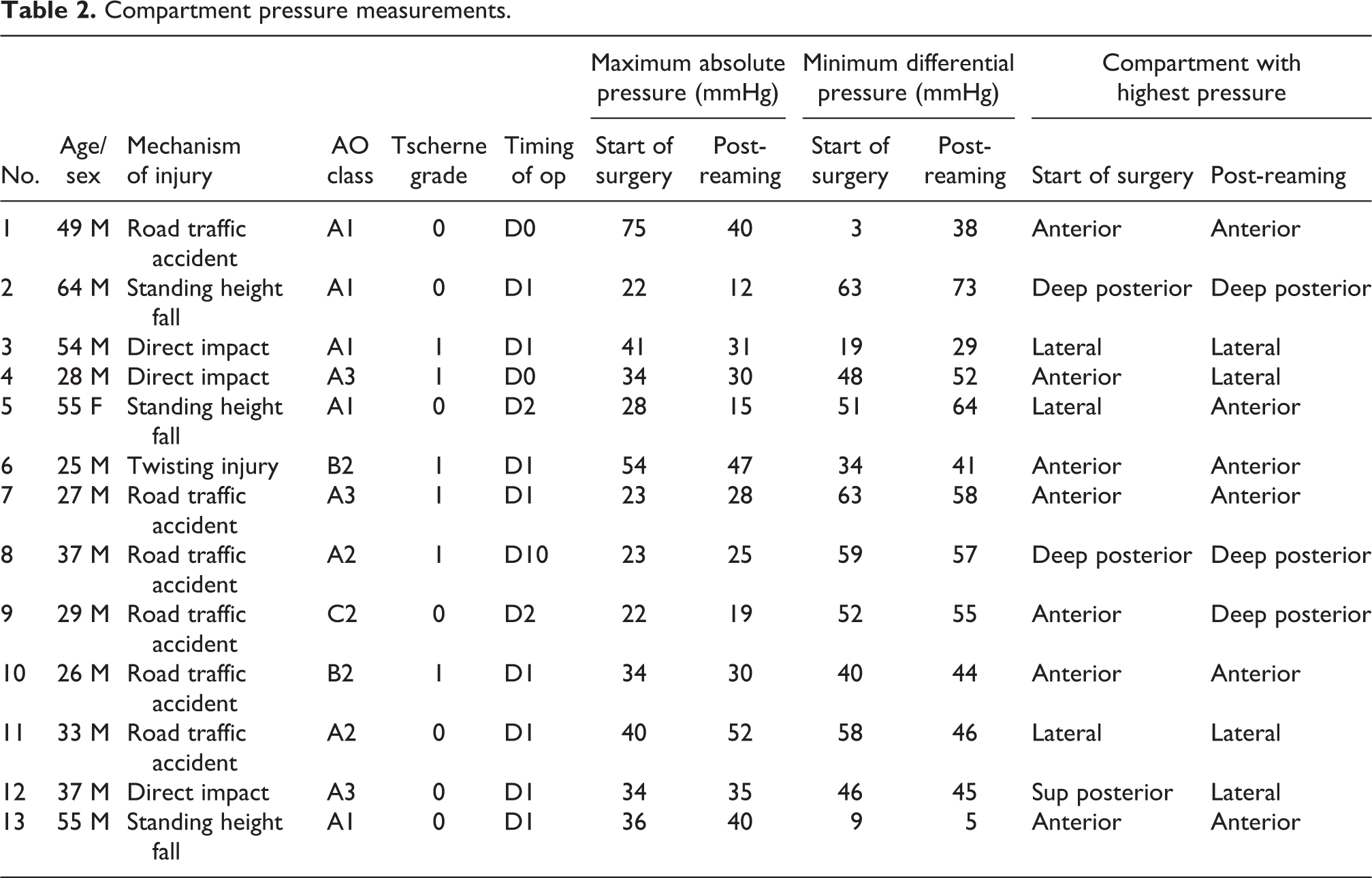
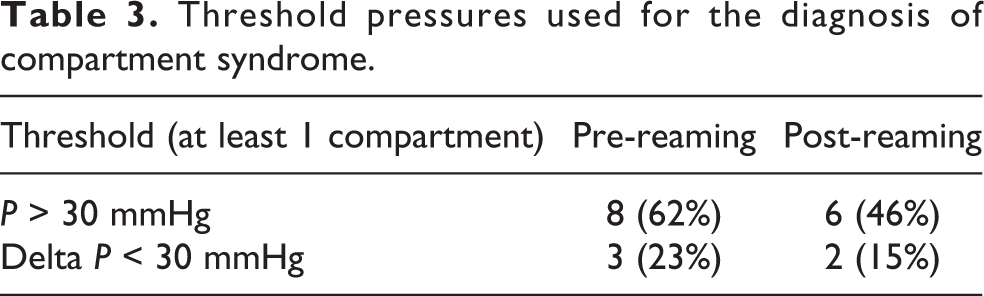
The highest compartment pressures measured at the start of surgery and after tibial reaming and the respective minimum differential pressures, as well as the compartments involved, are shown in Table 2. Taking the highest readings of the four compartments measured at the start of surgery, eight patients (62%) had at least one absolute compartment pressure exceeding a threshold of 30 mmHg. Looking at the differential pressures, three patients (23%) had at least one compartment measurement within 30 mmHg of the diastolic blood pressure. All these patients would have undergone decompressive fasciotomy, if the respective threshold of decompression had been used. Post-reaming, six patients (46%) had at least one absolute compartment pressure exceeding a threshold of 30 mmHg. Two patients (15%) had at least one compartment within 30 mmHg of the diastolic pressure. These results are summarized in Table 3.
Compartment pressure measurements.
Threshold pressures used for the diagnosis of compartment syndrome.
Of note, one patient had maximum absolute pressures of 75 mmHg measured in the anterior and superficial posterior compartments, 72 mmHg in the deep posterior compartment and 67 mmHg in the lateral compartment, with corresponding differential pressures of 3, 6 and 11 mmHg, respectively, at the start of the procedure. Fasciotomy was not performed (according to the study protocol), and he did not develop any evidence of compartment syndrome during the entire post-operative period.
The average pressures in each compartment before and after reaming are tabulated in Table 4. The mean absolute pressure was 28.5 mmHg at the start of surgery and 23.1 mmHg after tibial reaming, though this difference was not statistically significant (p = 0.15). The highest compartment pressures were recorded in the anterior compartment both before and after reaming, with an average absolute pressure of 32.2 mmHg at the start of surgery and 26.5 mmHg after reaming. The superficial posterior compartment demonstrated the lowest average pressures both before and after reaming, measuring 25.1 and 19.2 mmHg, respectively.
Average compartment pressures, by compartment.

SD: standard deviation.
Discussion
This study found that a significant proportion of patients (up to 62%) with closed tibial shaft fractures and who clearly did not have clinical evidence of compartment syndrome may be overdiagnosed and hence undergo unnecessary fasciotomy, if the commonly cited threshold pressure of 30 mmHg is strictly adhered to. Using a higher threshold of 40 mmHg, or a differential pressure threshold of within 30 mmHg of the diastolic pressure resulted in a lower, but still significant, proportion of cases (23%) that may be overdiagnosed.
These findings are in keeping with other studies in the literature. In a study by Øvre et al., 23 18 (29%) of 63 patients with tibial fractures treated with intramedullary nailing underwent fasciotomy based on an absolute pressure threshold of 30 mmHg detected on continuous tissue pressure monitoring. The authors concluded that this pressure threshold seems to give an unacceptably high rate of fasciotomies. McQueen and Court-Brown found similar high pressures in their series of 116 patients with tibial fractures whose anterior tibial compartment pressures were monitored – 45% had absolute pressures above 30 mmHg and 23% above 40 mmHg. They recommended using a differential pressure of under 30 mmHg, which in their series resulted in only three patients (2.6%) requiring fasciotomy. 16 Prayson et al. further demonstrated that a majority of isolated lower extremity injuries (up to 95%) exhibited baseline pressure readings that would typically be considered indicative of compartment syndrome, when actually none of the patients they studied developed compartment syndrome. 24
A significant inherent limitation of the common practice of taking one-time compartment pressure measurements is that it merely provides a snapshot of the state of flux the body is continuously experiencing. It needs to be remembered that both tissue pressures and blood pressure are constantly in a dynamic balance in the trauma patient undergoing surgery, who is constantly subject to anaesthetic agents, ongoing blood loss, mechanical manipulations and other painful stimuli. The duration of exposure to an elevated tissue pressure or a depressed diastolic pressure is possibly as important a factor to consider as the threshold pressure value alone, which one-time pressure measurements fail to account for.
An interesting finding from our study was that tibial reaming appeared to decrease compartment pressures in this study. While not observed in all cases, the mean pressures were lower after reaming, although this difference was not statistically significant, given the limited sample size. This apparent decrease in pressures following reaming may be related to alterations in local circulation caused by reaming, although this conclusion can by no means be made based on this study alone.
The evidence in the literature is mixed with regard to this issue. Most studies suggest at least a transient rise in intracompartmental pressures during nailing with reaming, though this rise may not be persistent and/or clinically significant. 25 –29 Again, the results of our study could be attributed to the fact that single measurements may not adequately demonstrate transient pressure changes that may indeed have occurred in the compartment, and the readings obtained may be dependent on the timing they are taken after completion of reaming. Nonetheless, we postulate that the pressure increases would need to be sustained to have a significant clinical effect on the development of compartment syndrome, and such sustained pressure increases would be detectable irrespective of the measurements being taken shortly after the completion of reaming.
This study has a number of limitations. Firstly, the length of follow-up is limited to the duration of the patient’s hospitalization. While it is highly unlikely that an acute compartment syndrome be completely missed in the post-operative period, ideally a longer period of follow-up could be implemented to document the absence of any long-term sequelae of a missed diagnosis (e.g. contractures or chronic sensorimotor dysfunction). Secondly, the sample size is fairly small. While this is sufficient to demonstrate that commonly quoted pressure thresholds are overly conservative, and compartment syndrome may be overdiagnosed when these threshold values are utilized, a larger sample size would allow greater confidence in prescribing more selective threshold values.
The main strength of our study lies in its prospective design, homogeneous study population and findings that are immediately relevant to clinical practice. Our findings suggest that the mere presence of a tibial fracture necessarily elevates compartment pressures, and clinicians should be wary of immediately attributing such elevations to the presence of compartment syndrome. While no better alternative may be available to assess the intubated, comatose or intoxicated patient, our study is a timely reminder that one-time compartment pressure measurements has only a limited role in fully cooperative patients, and should never be used in the place of good clinical judgement and careful serial examinations.
Conclusion
We conclude that raised compartment pressures are frequently seen in patients with tibial shaft fractures, and this degree of elevation is usually not significant enough to result in acute compartment syndrome. Commonly quoted threshold values for absolute compartment pressures and differential pressures, when used in conjunction with standard compartment pressure measurement techniques, may result in overdiagnosis of acute compartment syndrome and unnecessary fasciotomies in a sizeable number of patients. For all intents and purposes, compartment syndrome remains a clinical diagnosis, and one which always needs to be considered when managing tibial fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.