
Abstract
Background:
Total knee arthroplasty (TKA) has been established as a successful surgical treatment in the late stages of rheumatoid joint destruction. The purpose of this study was to review the clinical outcome and survivorship in rheumatoid arthritis (RA) patients undergoing TKA in hybrid technique with a cementless fixation of the femoral component.
Methods:
We analysed retrospectively 66 RA patients who underwent 72 TKAs (P.F.C. Sigma®). Mean follow-up time was 124 ± 41 months. To evaluate postoperative clinical outcome, knee injury and osteoarthritis outcome score (KOOS) and Oxford knee score (OKS) were assessed. Kaplan–Meier analysis was used to calculate survivorship. The primary outcome was revision for any reason.
Results:
Thirty-four patients (36 knees) died and two patients (2 knees) were lost to follow-up. Three patients (four knees) did not agree to participate. Twenty-seven patients (30 knees) were available for assessing clinical scores. The average scores were 85 ± 14 for KOOS and 34 ± 10 for OKS. In three patients (three knees), revision was necessary, including restricted range of motion (n = 1), instability (n = 1), and infection (n = 1). There were no cases of loosening in this cohort study. The survival rates were 100% at 5 years, 97.1% at 10 years (95% CI 89.0–99.2%) and 95.6% at 15 years (95% CI 86.9–98.5%).
Conclusions:
This study confirms that excellent clinical results and a good 10-year survivorship can be obtained with hybrid fixation technique in TKA in the unique population of RA patients.
Keywords
Introduction
Rheumatoid arthritis (RA) as an immune mediated chronic inflammatory disease and mainly affects synovial joints and leads to destruction of bone and cartilage and functional disability. 1 The systemic inflammation process moreover has to be seen as a risk factor for increased prevalence of cardiovascular comorbidities. 2,3 Despite the success of highly effective pharmacotherapy in RA in last decades, rates of total joint arthroplasty (TJA) in RA remain static. Concerning the knee joint being one of the most commonly affected joint, there is even some evidence to support a trend towards an increase of primary total knee arthroplasty (TKA) in patients with RA. 4 TKA has been established as a surgical procedure that provides pain relief, restores function and improves quality of life in RA patients who are pertained to end-stage joint destruction and functional disability. 5,6 RA is the third most common indication for lower limb joint replacement in Northern Europe and North America. 7 Nonetheless, the prevalence of RA in patients receiving TJA is just declared between 3.4% and 5%. 8,9 Thus, most of the studies regarding outcome following total knee replacement are based on patients with osteoarthritis (OA) as underlying pathology. Especially for the subgroup of RA, there is a lack of data that represent long-term results. 8,10,11 As end-stage knee joint arthritis in RA patients is often associated with poor bone stock representing osteopenia, subchondral cysts and osteolysis, it is still being discussed whether fixation of the femoral and tibial components is best performed in cemented, cementless or hybrid technique, 10,12 whereas a cemented fixation is mostly recommended in RA. 10,12,13 Nakama et al. reviewed systematically the benefits and harms of cemented, cementless and hybrid knee implants fixation and noted that it was not possible to provide separate results for the subgroup of RA. 10 The purpose of this study was to review the clinical outcome and survivorship for the subgroup of RA patients undergoing TKA in hybrid technique with a cementless fixation of the femoral component.
Material and methods
Study population
We retrospectively reviewed all patients with the diagnosis of RA that underwent primary TKAs between 1997 and 2001 in our department. RA was defined in accordance with the American College of Rheumatology criteria. 14 The designated follow-up date was May 2013. In total, 66 patients (54 women (59 knees) and 12 men (13 knees)) were found and asked to participate. In case of death, the primary care physician was consulted to receive information about the cause of death and a potentially performed external revision. There were 34 left and 38 right knees. Fifteen knees displayed preoperatively a varus deformity, 17 knees displayed a valgus deformity and remaining 41 knees with no deformity. Nine knees represented pronounced subchondral cysts preoperatively.
Prosthesis and surgical technique
All TKA surgeries were carried out using the posterior cruciate retaining PFC prosthesis (P.F.C. Sigma®, DePuy Orthopaedics, Warsaw, Indiana, USA). Components are manufactured from cobalt chromium molybdenum alloy. The porous femoral components are manufactured using a sintering process. The senior author (B.S.) performed all surgeries using a standard medial parapatellar approach. The posterior cruciate ligament (PCL) was retained in all cases. A ligamentous release was carefully performed in 24 knees to achieve ligament balancing and harmonic patella tracking. Femoral components were inserted using a press-fit technique, and tibial components were fixed with cement (Refobacin-Palacos, Heraeus Medcial GmbH, Weinheim, Germany) with a syringe and finger tapping without vacuum mixing or pulsed lavage. Highly cross-linked polyethylene fixed bearing inlays were inserted. After implantation of the femoral and tibial components, the knees were kept in full extension under the period of cement hardening. A denervation and removal of osteophytes was performed around the patella, and no patella resurfacing was performed in any case. Antibiotic and thrombosis prophylaxis was given to all patients. The patients were allowed to stand on the second postoperative day and advised to comply with limited weight bearing conditions (15 kg) for 3 weeks, following further 3 weeks with gradually increasing weight bearing conditions.
Clinical evaluation
To evaluate postoperative clinical outcome, knee injury and osteoarthritis outcome score (KOOS) 15 and Oxford knee score (OKS) 16 were assessed at follow-up time. An OKS of ≥ 36 was categorized as “very satisfied”, ≥ 27 points as “satisfied” and ≤ 25 as “unsatisfied” patients. 17 KOOS was graduated accordingly to the population-based reference data. 18
Statistical analysis
All data were analysed using Graph Pad Prism (GraphPad Software Inc., San Diego, California, USA). Kaplan–Meier analysis was used to calculate survivorship. 19 The survival endpoint was revision for any reason. Ninety-five percent confidence intervals (CIs) were calculated.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Each patient gave informed consent prior to surgery, and the institutional ethics committee approved the study (ref. no. 4026; University of Erlangen-Nuremberg).
Results
The mean follow-up time of all patients was 124 ± 40 months (range 10–182 months), whereas follow-up time for living patients was 152 ± 14 (range 128–182) months. The mean age at the time of surgery was 62 ± 11 years (range 33–80). The average duration of RA after diagnosis was 22 ± 11 years. At follow-up date, 34 patients (36 knees) have died (mean lifetime after surgery 100 ± 42 months). No relation between the cause of death and the performed knee arthroplasty was observed. Two patients (two knees) were lost to follow-up and three patients (four knees) did not agree to participate. Following 27 patients (30 knees) were available for assessing clinical scores (Figure 1).

Flow diagram illustrating passage of patients through retrospective analysis.
The average scores for KOOS were 85 ± 14. For OKS, we obtained 34 ± 10. During the observation period, in three patients (three knees), revision was necessary (4.16%). One patient was affected of a pronounced extension lag (74 months postoperatively) and underwent polyethylene exchange, one patient had been revised for instability (106 months postoperatively) and one patient had a delayed infection (126 months postoperatively) after an externally performed inlay revision. She underwent prosthesis removal, debridement, antibiotic suppression and reimplantation after a period of 6 weeks. There were no revisions because of implant loosening.
Figure 2 shows the survival of the implant. The mean revision rate with revision for any reason was 4.1%. The 5-year survival rate was 100%; after 10 years, 97.1% (95% CI 89.0–99.2%) and revealed 95.6% (95% CI 86.9–98.5%) after 15 years (Figure 2).
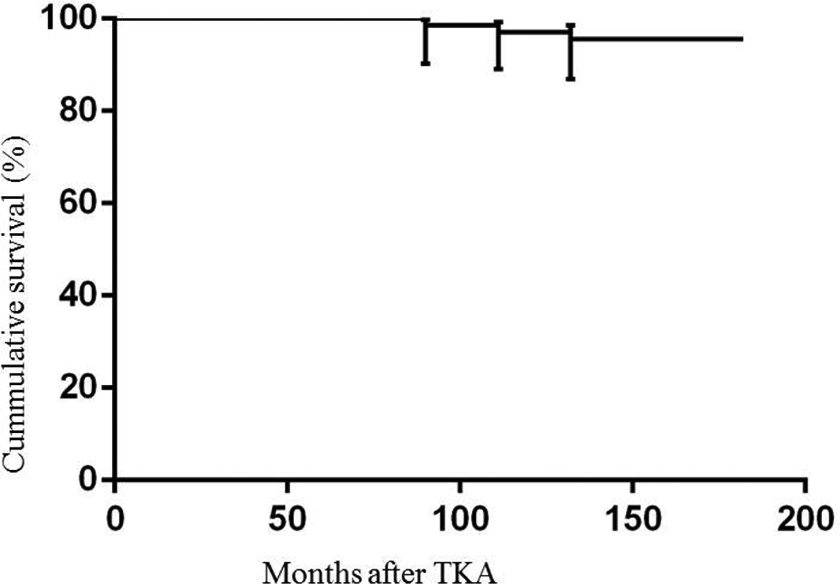
Survival curve shows patients after TKA with the end point being revision for any reason. TKA: total knee arthroplasty.
Discussion
In the late stages of RA, the only remaining treatment is surgery and replacement of the joint surfaces with a non-constrained bicondylar or (semi-)constrained TKA. 10 In our study, we retrospectively observed patients after TKA which was exclusively done for a rheumatoid joint destruction. The mean age of patients in this study (62 ± 11 years) appears quite young. This finding can be confirmed regarding study populations dealing with the subgroup of RA in TKA. Danoff et al. declared in his systematic review that RA patients were on average 10 younger at the time of surgery than OA patients. 20 Sledge reviewed 351,103 TKAs and found that RA to be on average younger at the time of surgery than OA patients (RA: 64.3 years vs. OA: 66.6 years; p < 0.001). 8
The number of patients who died during the observation period is noticeable high. More than half of patients (51.2%) died and revealed an average lifetime after surgery of 100 ± 42 months. This observation could be explained by high global mortally rates in RA. 2,21,22 Meta-analysis of observational studies found that morbidity and mortality risks caused from cardiovascular causes were close to 50% and up to 60% higher than those of the general population. 2,23 –25 Cardiovascular diseases are recognized as the leading cause of death in RA patients, accounting for nearly 40% of their mortality. 26 Moreover, RA has been associated with increased prevalence of further comorbid disorders such as pulmonary diseases or kidney failure, conferring significant morbidity and mortality. 27,28
Clinical outcome and survival analysis
The post-operative OKS has been established as an accurate predictor of the level of patient satisfaction. 17 As we could obtain an average OKS score of 34 ± 10, our results can be classified in the category satisfied. Accordingly to the population-based reference data for the KOOS published by Paradowski et al., the average score of 85 ± 14 has to be seen as age appropriated. 18
Our long-term results of hybrid fixation in TKA in RA patients demonstrated excellent implant survival after 5, 10 and, respectively, 15 years (Figure 3). In the most recent reports, TKA in patients with RA has shown excellent long-term survivorship. Meding et al. reported a 15-year survivorship excluding infection for cemented TKA of 96.5%, 29 and Rodriguez et al. reported a 15-year survivorship of 91% and 96.5% for PCL retaining and PCL scarifying implants. 30 In a follow-up study performed by Gill and Joshi enclosing 66 RA TKAs in cemented technique, an implant survival of 90.7% after 19 years could be obtained. 31 Lee et al. reviewed 112 RA patients following TKA including 45 knees performed in cemented technique, 69 knees in cementless technique and 62 knees fixed in hybrid technique. They published a survival with endpoint being revision for any reason for all patients of 84.7% at 10 years and mentioned a trend for better survival with cemented fixation; however, the difference was not significant. 32 Cemented implants are recommended to be preferred in poor bone quality and osteoporosis such as in RA. A cementless or hybrid fixation has been associated with the advantage of having a shorter surgical time and benefits in arthroplasty revision as the cement is not interlocked with the bone. 33 Regarding literature concerning full cementless fixation in RA, Viganó et al. described a 10-year survival rate of 98.4%. His study population contained patients with an average age of 49.5 years. 34 It could be argued that these patients are not representative as they had possibly a better bone quality than elderly patients concerning the process of osteointegration. However, there are only limited data available to evaluate the clinical outcome of TKA in hybrid fixation technique. Following our data may help to support the approach of hybrid fixation in TKA in RA.

Posteroanterior and lateral radiographs of a right knee. (a) Demonstrating advanced osteoarthritis and valgus malalignment. (b) The same patient 2 month following bicondylar hybrid TKA. (c) The same patient 168 month after bicondylar hybrid TKA. TKA: total knee arthroplasty.
Study limitations
The study has several limitations. As more than half of the patients died, the high rate of mortality led the number of patients to decrease during the observational period. This finding is similar to many studies dealing with long-term results in patients with RA. 31
Secondly, we did not analyse the causes of deaths, comorbidities or the administered medication taken by the patients. The retrospective analysis limits the significance of the clinical outcome as we are not able to compare them to preoperative status. Finally, a control group with cemented femoral components was not included. Further investigations representing a randomized follow-up design comparing data between cemented and hybrid technique with RA patients are needed. Radiological surveillance is warranted to comment on asymptomatic loosening. However, performing all TKAs with the same surgical approach and carried out by one surgeon, the use of one prosthesis design and the long follow-up time with a low rate of lost to follow-up (2.7%) and the clearly selected cohort of RA patients fortify the drawn conclusions of our study.
Conclusions
Our study confirms that excellent clinical results and a good 10-year survivorship can be obtained in TKA performing a hybrid technique with a cementless fixation of the femoral component in the unique population of RA patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.