
Abstract
Purpose:
Hypotensive anesthesia is crucial during arthroscopic shoulder surgery to reduce bleeding and allow for clear visibility. The aim of this study was to compare the clinical efficacy of continuous infusion of remifentanil, nicardipine, and remifentanil plus nicardipine to control hypotensive anesthesia in arthroscopic shoulder surgery.
Methods:
For this study, we enrolled 45 consecutive patients who were scheduled to have arthroscopic rotator cuff repair surgery and randomly allocated them into remifentanil (group R, n = 15), nicardipine (group N, n = 15), and remifentanil plus nicardipine (group RN, n = 15) groups. During the surgeries, these drugs were administered with continuous infusion. We analyzed the mean arterial pressure (MAP) and heart rate during surgery, stay time in the recovery room, visual analogue scale (VAS) scores, use of antiemetics in the recovery room, and postoperative blood urea nitrogen and creatinine changes.
Results:
The VAS score in the recovery room was higher for group R (mean 5.6, SD 1.4) than for groups N (mean 3.9, SD 0.9) and RN (mean 4.0, SD 1.1; p = 0.000). There were no statistical differences regarding other clinical variables among the three groups (all p > 0.05) except for MAP at 120 min of surgery between groups N and RN (N: 84.67 (SD 10.7) mmHg, RN: 65.4 (SD 9.2) mmHg, p = 0.027).
Conclusion:
The continuous infusion of remifentanil plus nicardipine appeared to be advantageous for maintaining hypotensive anesthesia until 120 min of arthroscopic shoulder surgery without rebound pain in a postanesthesia care unit.
Introduction
With the improvements in technology and instrumentation, arthroscopy has become the primary treatment modality for various shoulder disorders such as arthroscopic labral repair, rotator cuff repair, and even Latarjet procedures. 1,2
Compared with open techniques, shoulder arthroscopy allows for smaller incisions, faster recovery, and pain-free muscle contraction and also has cosmetic benefits. During arthroscopic shoulder surgery, clear visibility is essential. 3,4 Various methods have been used to ensure clear visibility during surgery such as using electrocautery to coagulate the blood, using velocity and pressure control pumps for irrigation flow, and mixing vasoconstrictors such as epinephrine with irrigation fluid. 5 However, controlled hypotensive anesthesia is still the most effective method for achieving clear visibility.
For deliberate hypotension during surgery, sodium nitroprusside or nitroglycerin and inhalation anesthetics have traditionally been used, but the use of these drugs was limited because of reflex tachycardia, increased myocardial oxygen demand, and the potential for liver or kidney damage. 6
Some drugs that lower blood pressure (BP) such as remifentanil and nicardipine have been used during general anesthesia with little risk. Remifentanil, an ultrashort-acting opioid, is widely used to induce hypotension during general anesthesia with no kidney damage. However, a number of studies have reported that remifentanil was associated with patients’ developing acute pain tolerance and postinfusion hyperalgesia. 7 –9 On the contrary, nicardipine, a calcium channel blocker that can be used to induce hypotension without development of hyperalgesia or tolerance, 6 is also known to have the effect of preserving kidney function during hypotensive anesthesia, 10 although care should be taken in using it with hemodynamically unstable patients with cardiac problems. 11
There have been a number of studies regarding a variety of drugs to induce hypotensive anesthesia, 6,12 –17 but studies that compared the clinical efficacy of continuous infusion of these BP-lowering drugs are few. We hypothesized that the continuous infusion of nicardipine plus remifentanil might be more effective in controlling hypotensive anesthesia as well as pain than single infusions of either remifentanil or nicardipine. Thus, the aim of this study was to compare the clinical efficacy of continuous infusions of remifentanil, nicardipine, and remifentanil plus nicardipine to control hypotensive anesthesia as well as pain during arthroscopic shoulder surgery.
Materials and methods
This study was approved by the Institutional Review Board and Hospital Research Ethics Committee of the authors’ hospital. We obtained consent from each patient who was enrolled in the study.
Subject enrollment
Between December 2015 and April 2016, we assessed for eligibility in 75 consecutive patients who were scheduled to receive arthroscopic rotator cuff repair surgery. The exclusion criteria were American Society of Anesthesiologists (ASA) physical status grade above 2 (n = 25) or a traumatic rotator cuff tear (n = 3) to rule out other sources of pain and bleeding. We then randomly allocated (www.randomization.com) 47 patients into either the remifentanil group (group R, n = 16), the nicardipine group (group N, n = 15), or the remifentanil plus nicardipine group (group RN, n = 16). As we allocated the patients to each group, a nurse (number I) from the anesthesiologist department who was completely excluded from the measurements after the start of anesthesia administered the infusion pump. We excluded one patient in group R and one in group RN because they were to receive open surgery instead. Finally, we equally allocated 15 patients into each group and analyzed them (Figure 1). Their demographics and baseline characteristics are summarized in Table 1.
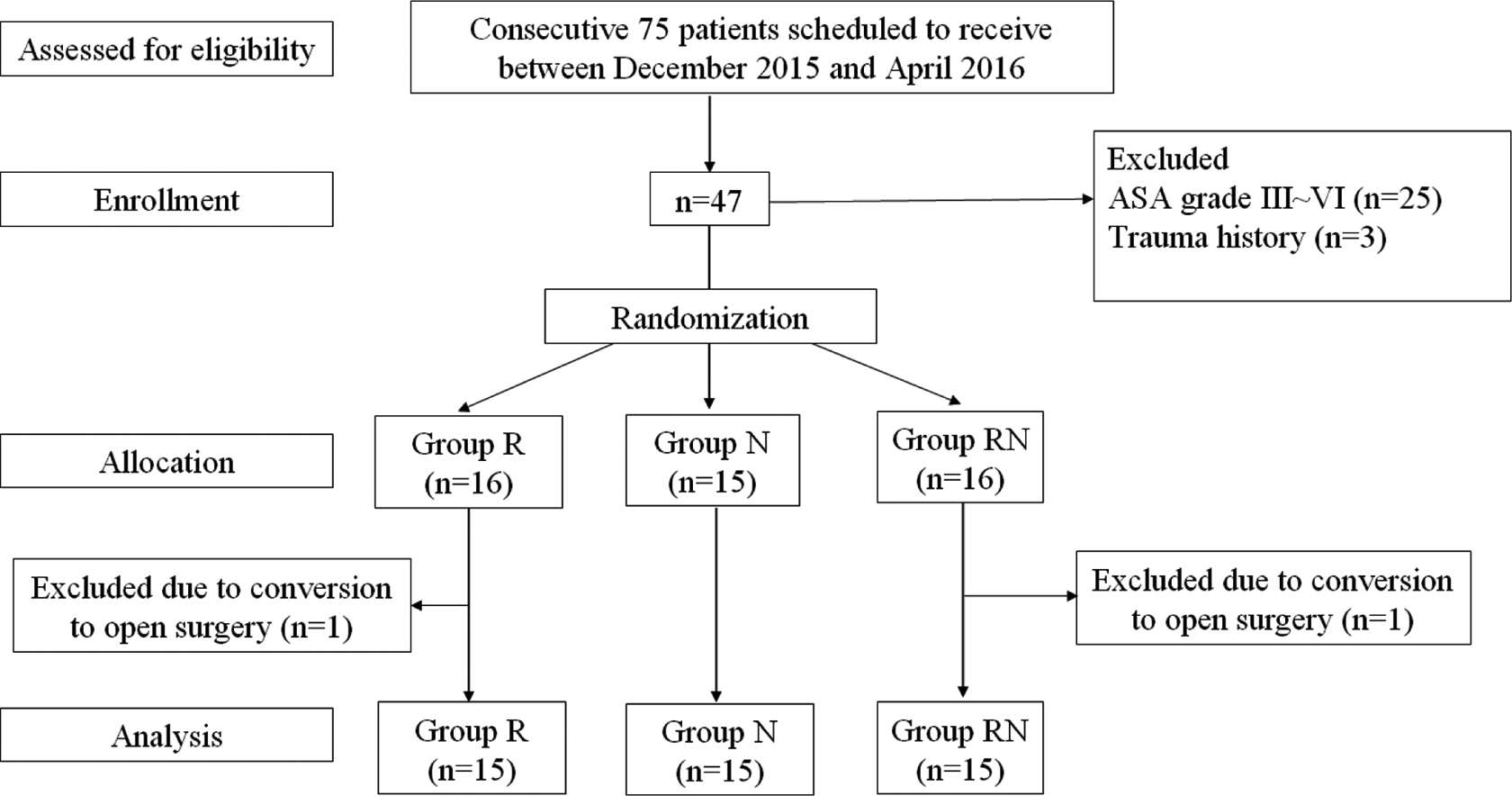
Flowchart of subjects’ enrollment, allocation, and analysis.
Demographics and baseline clinical characteristics of the three groups (R, N, and RN).

R: remifentanil; N: nicardipine; RN: remifentanil plus nicardipine; ASA: American Society of Anesthesiologists; AP: Anteroposterior; BUN: blood urea nitrogen; Cr: creatinine; SD: standard deviation.
Monitoring and anesthesia protocol
Electrocardiogram, pulse oximetry, heart rate, BP, temperature, and capnograph were monitored for the patients’ safety during the operations and during early recovery in the postanesthetic care unit (PACU). Anesthesia was induced using propofol (2 mg/kg), fentanyl (1 µg/kg), lidocaine (1 mg/kg), and rocuronium (0.6 mg/kg) for muscle relaxation. Mean BP (MBP) was measured using noninvasive BP monitoring, and mean arterial pressure (MAP) was monitored as well. The hypotensive anesthesia, which we defined as MAP at 50–65 mmHg and target range percentage during deliberate hypotension was calculated. We decided the MAP at 50–65 mmHg as the target or lower limit of safety BP from the references of previous studies to be effective in reducing blood loss and avoiding serious complications due to organ hypoperfusion. 18 –20 The hypotension-inducing drugs were administered by continuous infusion, and when the MAP did not reach the target, the study drug was increased in steps. The anesthesia maintenance protocol during surgery was as follows: Remifentanil was infused with 0.1–0.2 µg/kg/min in group R; nicardipine was infused with 1–4 µg/kg/min in group N; and remifentanil 0.1–0.2 µg/kg/min with nicardipine 1–4 µg/kg/min was infused in group RN.
Surgical procedures
A single surgeon, the first author, performed all of the arthroscopic shoulder surgeries. The patients were maintained in the lateral decubitus position during the surgery, and the surgeon performed synovectomy, biceps procedures, and debridement for torn rotator cuff tendons in the glenohumeral joint. Subacromial decompression was routinely performed to acquire a flat acromion undersurface, not to remain the source of external impingement. The anteroposterior diameter and retraction of the tear were measured with a calibrated probe, and the footprint was prepared with a motorized burr. The rotator cuff was repaired with suture bridge techniques in each case in this study, and after the surgery, each patient received an abduction brace to protect the repaired cuff before the extubation.
Outcomes Measurement
A nurse anesthetist (number II) who was completely unaware of the protocol of this study assisted in measuring the various outcomes during the anesthesia; MBP, MAP, and heart rate were measured at 10, 30, 60, 90, and 120 min after the initiation of the anesthesia, and the infused fluid volume was checked at the end of each operation. In addition, we calculated the ratios of on-target and above-target MAP times to total surgery time.
Another nurse from anesthesiologist department (number III) assessed the patients’ visual analog scale (VAS) for pain scores (0–10 with 10 as the worst pain), stay time in the PACU, and use of antiemetics in the PACU (to evaluate postoperative nausea and vomiting [PONV]). We also assessed pre- and postoperative blood urea nitrogen (BUN) and creatinine (Cr) levels to check kidney function.
Sample size calculation
From the pilot study of five subjects in each of the three groups, we calculated the effect size as 0.62 and the total sample size as 45 (15 at each group) with a power of 80% at a type I error level of 0.05.
Statistical methods
We performed all statistical analyses with SPSS 20.0 (SPSS Inc., Chicago, Illinois, USA) and considered p values less than 0.05 to be statistically significant. To compare the continuous variables by group, we used the Kruskal–Wallis test, and we used the Tukey test for the multiple post hoc comparisons. We used either Fisher’s exact test or the χ 2 test to analyze the categorical variables and repeated-measure analysis of variance for the serial comparisons of MAP and heart rate.
Results
During the 120 minutes of anesthesia of each arthroscopic shoulder surgery, the MAP and heart rate in each group generally decreased (Figures 2 and 3). The MAP in group RN was lower than that in other groups but statistically nonsignificant except at 120 min of anesthesia (group R (n = 4): 76.7 (SD 6.5) mmHg; group N (n = 4): 84.7 (SD 10.7) mmHg; group RN (n = 6): 65.4 (SD 9.2) mmHg, p = 0.020; see Figure 2 and Table 3). There were no statistically significant differences in anesthesia time (p = 0.343) or operation time (p = 0.500) for the three groups with 120 min of anesthesia. Group N recorded the highest heart rate, but there were no statistically significant differences by group for any duration of anesthesia (all p > 0.05; Table 4). Group R was checked for bradycardia at 120 min of surgery, and there was a significant difference between that group and group N (R: 56 (SD 3.7), N: 73 (SD 7.0), p = 0.010). In group R, hypotensive anesthesia was maintained for only 15% of the surgery time compared with 34% of the time in groups N and RN, but these differences were also not statistically significant (p = 0.09; Table 2). The VAS pain score in the PACU was significantly higher in group R than in the other two groups (p = 0.000; Table 2). However, there were no significant differences by group in antiemetic use, PACU stay time, or renal function (BUN and Cr) (Table 2).

The changes in mean arterial pressure (MAP) during the surgery by group.
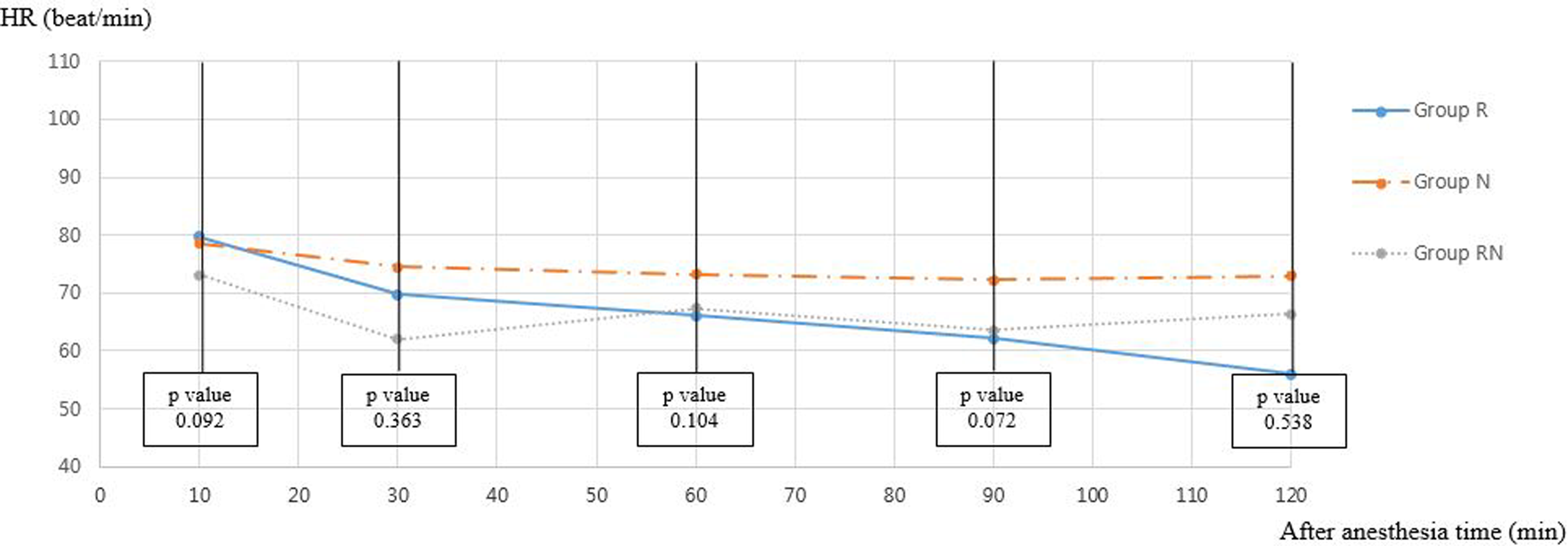
The changes in heart rate (HR) during the surgery by group.
Clinical outcomes by group.

VAS: visual analog scale; R: remifentanil; N: nicardipine; RN: remifentanil plus nicardipine; PACU: postanesthetic care unit; BP: blood pressure; Cr: creatinine; BUN: blood urea nitrogen; SD: standard deviation.
*p Value < 0.05 is statistically significant.
Multiple comparisons of intraoperative BP (Blood Pressure) by group.

R: remifentanil; N: nicardipine; RN: remifentanil plus nicardipine.
Multiple comparisons of intraoperative HR (Heart Rate) by group.

R: remifentanil; N: nicardipine; RN: remifentanil plus nicardipine.
Discussion
In the current study, single continuous infusion of remifentanil and of nicardipine was not superior at maintaining hypotensive anesthesia; however, the mixed use of remifentanil with nicardipine showed superiority to the single infusions at 120 min after the start of general anesthesia. In addition, the remifentanil plus nicardipine group had significantly lower postoperative VAS pain scores in the PACU compared with group R.
The hypotensive anesthesia was effective in reducing blood loss without the risk of organ hypoperfusion, 21 and therefore, it could be used as a routine anesthetic procedure for orthognathic surgery, especially bimaxillary osteotomy. 22 In one meta-analysis, the use of deliberate hypotension in orthopedic surgery was also supported for reducing blood loss and transfusion requirements. 21 However, some of the literature has still questioned the efficacy of hypotensive anesthesia, 13 and there are few studies on its clinical efficacy during arthroscopic shoulder surgery. Hypotensive anesthesia during this surgery was believed to be essential for successful operations because it allowed for clear visibility. Breckon 23 insisted that the anesthesiologist’s role during shoulder arthroscopic surgery is to help maintain a bloodless field by manipulation of the BP and to provide adequate perioperative analgesia. The author also insisted that deliberate hypotensive anesthesia has the advantage of decreased blood loss helping to maintain a clear surgical field and reduce operation time. The effectiveness of hypotensive anesthesia regarding less bleeding and clear visibility in other surgical fields was also present. Atighechi et al. 24 reported that bleeding disturbs the visibility of surgical field and increases operation time during functional endoscopic sinus surgery. Guney et al. 25 and Rodrigo 26 reported that induced hypotensive anesthesia can reduce bleeding and improve the surgical fields during nasal or orthognathic surgery. However, we observed that the hypotensive anesthesia, which we defined in the current study as MAP between 50 and 65 mmHg, was not easily maintained throughout the full anesthesia period. Although the patients were administered continuous infusions of BP-lowering drugs as planned, we could never achieve MAP below 65; the low-dose infusion rate (0.1–0.2 µg/kg/min) might be insufficient to induce hypotensive anesthesia. However, considering the hemodynamic stability and the possibility of severe bradycardia when using more than 0.2 µg/kg/min of a remifentanil infusion, 27,28 it would be appropriate to adopt the current study protocol. In fact, the surgeon in this study (the first author) never complained of the uncontrollable bleeding that impairs visibility during surgical procedures.
Remifentanil is a rapid-onset, short-duration opioid, and anesthesiologists frequently use it to safely and temporarily reduce BP during surgery. However, we observed the inferiority of single remifentanil infusions for maintaining a hypotensive state throughout the anesthesia, which was 15% of the total surgery time. Nicardipine is a calcium channel blocker that is commonly used for acute hypertension control in anaesthetized patients. 29 Unlike nitroglycerin, which has been commonly used to lower BP, nicardipine has been used more frequently recently because there is little incidence of rebound hypertension, platelet malfunction, or impaired renal function. 10,15,30
One of the known side effects of nicardipine use is tachycardia during surgery, and it was known as a secondary effect of the hypotension. However, we observed no tachycardia cases in this study.
In general, the single continuous infusion of nicardipine also lowered the BP, but it was not as effective as remifentanil plus nicardipine at a late stage of anesthesia. Arthroscopic shoulder surgery commonly uses large volumes of irrigation fluid during the operation; we observed the mean used fluid volumes to be 450–600 dL throughout the current study. These large volumes of irrigation fluid could have caused painful swelling of the shoulder and increased BP due to the pain, and this would be likely to occur near 120 min of anesthesia. Remifentanil-induced hyperalgesia, or acute tolerance, is a well-known side effect of remifentanil overuse; it usually occurs in a dose-dependent manner, and therefore, combining remifentanil with nicardipine might reduce the use of remifentanil itself and effectively prevent the remifentanil-induced hyperalgesia or rebound pain late in surgery or even in the PACU. Guignard et al. 7 reported that a large dose of infused remifentanil (0.3 µg/kg/min) caused acute opioid tolerance and hyperalgesia, and Joly et al. 8 found that a large dose of intraoperative remifentanil (0.4 µg/kg/min) increased peri-incisional wound hyperalgesia and allodynia; in addition, one study found that even a low dose of remifentanil infusion could cause hyperalgesia. 9 The remifentanil infusion at 0.1–0.2 µg/kg/min in the current study also induced hyperalgesia, and this result was in line with previous studies.
There was no correlation between intravenous BP-lowering drugs and PONV; the low dose of remifentanil in the current study setting appeared to make no difference in PONV. There were no cases of renal damage in this study because we used drugs with lower renal toxicity.
There were a number of limitations in this study. First, we could not evaluate the effects of the induced hypotension for visibility during the surgery, because there were no objective measurement tools for the visibility during arthroscopic surgery. Second, a number of other factors could have affected the hypotension such as the surgical technique and environment. Third, we did not include patients with ASA grades above 2 in this study, and these could be the main cohort for arthroscopic rotator cuff surgery. However, the target MAP should be set more higher in patients with higher ASA grades for safety, 18 which could distort the uniform study design, therefore other previous study with shoulder arthroscopic surgery was also performed in ASA grade 1 or 2. 31
The strength of our study was that this was the first study to prospectively evaluate the clinical efficacy of continuous infusions of nicardipine and remifentanil in shoulder arthroscopic surgery.
Conclusion
The continuous infusion of remifentanil plus nicardipine might have advantages for maintaining hypotensive anesthesia until late in surgery as well as preventing remifentanil-induced hyperalgesia compared with single continuous infusions of remifentanil or nicardipine.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.