
Abstract
Background:
Valgus-impacted femoral neck fractures treated with internal fixation occasionally result in unsatisfactory postoperative locomotive function, partially due to muscle shortening and a decrease in the moment arm. This study quantifies the degree of diminished abduction strength both clinically and biomechanically.
Methods:
Fifteen patients were enrolled in this study. Twelve patients with fracture healed in valgus-impacted position were further evaluated. Muscular strength around hip was examined, and values between the nonoperated and operated side were compared and analyzed. For the biomechanical study, two three-dimensional models were prepared: model I (control model without displacement) and model II (simulated malunion of a 15° valgus-impacted fracture). Two sets of hip flexion angles in each of the models were simulated with flexion angles of 0° and 23°.
Results:
Mean and standard deviation values for muscle strength from the nonoperative/operative side among the valgus group are as follows: flexion strength was 9.2 ± 4.0/9.2 ± 3.2, extension strength was 5.8 ± 2.8/6.1 ± 3.2, abduction strength at 0° was 9.1 ± 3.7/7.4 ± 3.6, abduction strength at 10° was 6.7 ± 3.0/5.5 ± 2.2, and knee extension strength was 15.3 ± 6.2/15.1 ± 6.0 (kgf). When comparing values between the nonoperative and operative sides, statistical significance was only observed in abduction strength (p < 0.01). The biomechanical models prove that valgus impaction decreases the moment arm by approximately 10% at both flexion angle.
Conclusions:
A significant decrease in abductor strength at 0° and 10° was observed in the valgus-healed group. This may be related to a decrease in the moment arm. Further research should be done to define the acceptable limit of deformity for the satisfactory postoperative functioning.
Keywords
Background
Femoral neck fractures cause major health problem in aging societies, such as in East Asia. Nondisplaced or valgus-impacted femoral neck fractures are generally stable and successfully treated with internal fixation performed in situ without anatomical reduction of the valgus position. 1 The procedure is minimally invasive, operative time is short, and the necessity for blood transfusion is low. 2,3 Furthermore, this treatment enables patients to undergo early rehabilitation. The implants used allow sliding or additional impaction at the fracture site. This sliding movement and valgus impaction itself will stabilize the fracture area and accelerate fracture union, hence lower rates of postoperative delayed union or nonunion. 4
Results of internal fixation treatment are acceptable as long as the fracture heals completely or with minimal displacement. However, we have observed in our outpatient service that some of the patients with valgus-healed femoral neck fractures occasionally complained of muscular weakness at the operative side. This may be due to the fact that femoral neck fractures often combine with muscle shortening and a decrease in moment arm that may lead to weakness during abduction. 5 Hip surgeons agree that same length of femoral shortening results in a larger damage for the shorter muscle, and the gluteus medius is shorter than the surrounding major muscles (iliopsoas, gluteus maximus, and quadriceps). 6 In addition, a valgus deformity may weaken abduction due to a relative lateral shift of the femoral head toward gluteus medius. Although measurement of horizontal displacement on radiographs has been reported, 7 visualization may not accurately reflect the three-dimensional (3-D) view of the moment arm. Mathematical exploration is necessary to calculate the precise value of the moment arm. We believe that a decrease in femoral length and shortening of the moment arm would lead to decreased muscular strength ending to functional impairment of daily activities.
The purpose of this study is to quantify the degree of diminished abduction strength and femoral shortening clinically and to calculate the moment arm biomechanically. Clinical measurements were done during the outpatient follow-up. The influence of valgus deformity on the gluteus medius moment arm is assessed using a 3-D geometric model reconstructed from computed tomography (CT) images.
Materials and methods
Clinical study
Thirty patients with stable femoral neck fracture osteosynthesized mainly with dual sliding and compression screw system (KiSCO Co. Ltd. Kobe, Japan) from 2012 March to 2014 December were selected from our trauma database. Exclusion criteria included the following: (1) less than 60 years of age at the time of surgery, (2) less than a 6-month follow-up period, (3) bilaterally operated hip, (4) presence of dementia, (5) inability to ambulate, (6) presence of central or spinal nerve disorder or Parkinson’s disease screened by the attending physician, (7) presence of nonunion or avascular necrosis at the hip joint, and (8) mortality. After applying the exclusion criteria, a total of 15 patients were enrolled in the present study (Figure 1). Twelve of the 15 patients with fractures healed in a valgus-impacted position, but without shortening at the medial cortex, were further evaluated. All patients had no major intra and postoperative complications and completed the postoperative rehabilitation program.
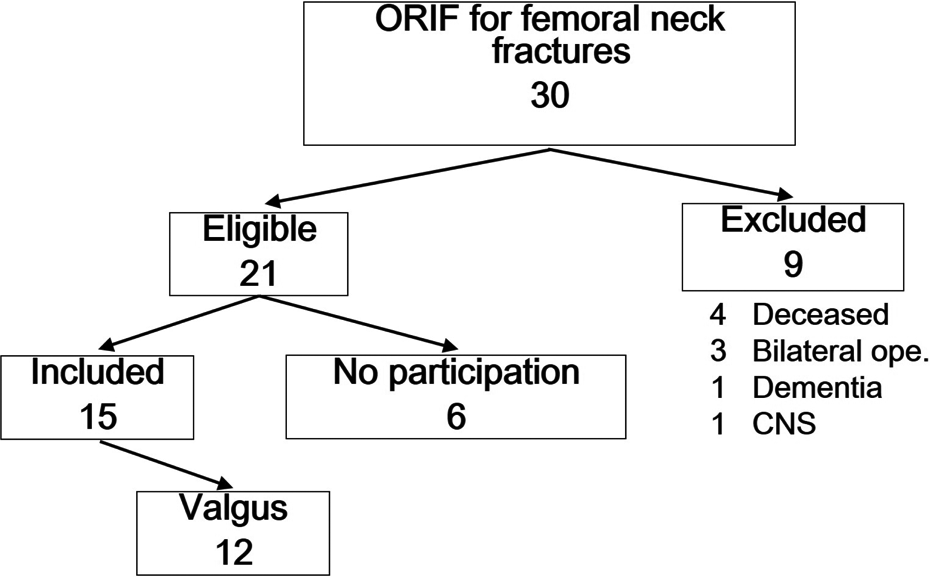
Flowchart describing the inclusion of patients.
Measurement of muscular strength
Strength of maximum isometric forces around the hip joint during flexion, extension, and abduction at angles of 0° and 10°, as well as during knee extension, was measured throughout the follow-up period. Radiographic examinations were also performed. Muscle strength was measured with a handheld dynamometer (μ tas F-1; Anima, Tokyo) by two physical therapists. 8 Muscular strength on hip flexion was measured with the patient in the sitting position. Muscle strength on extension was evaluated in the prone position with the contralateral hip flexed to prevent contraction of the quadriceps. Strength on abduction was measured in the supine position with the hip and knee extended. The legs were held in internal rotation to prevent contraction of the quadriceps muscle that may augment weak hip abduction. Knee extension strength was measured in the sedentary position without the legs touching the floor. 9 Means of three measurements for each position were evaluated, and values between the nonoperated and operated leg were compared and analyzed. All patients were tested similarly at our rehabilitation center.
Shortening was defined as vertical translation of the femoral head against the femoral shaft on anteroposterior radiographs. These values were calculated using the formula: (parameter on nonfracture side) − (parameter on fracture side), as a difference from the nonoperative to the operative side. Valgus angle at fracture site was measured on anteroposterior radiographs after fracture consolidation.
The moment arm of the gluteus medius was not determined on our plain radiographs, since we believe this would not reflect accuracy of measurement.
Statistical analyses
All data were analyzed using the software program Statistical Package for the Social Sciences (version 14.0; SPSS Inc., Tokyo, Japan). All means and standard deviation values were calculated from the nonoperative and operative sides in all 15 patients. Muscular strength between the nonoperative and operative side was compared using the Wilcoxon signed rank test. Similar statistical analysis was performed in 12 valgus-healed patients.
Biomechanical study
3-D models of the hip joint were virtually created to allow for a more accurate and superior method of evaluating the degree of reduction of the moment arm in valgus deformity.
Preparation of the geometric model
A 3-D geometric model of the bony structures of the pelvis and proximal femur was recreated from axial CT images (cortical and cancellous bone maps of the femur) of a healthy 83-year-old female volunteer without any bone impairment. CT images were taken at 0.625 mm intervals. Construction of the model was with patient consent and was approved by the Ethical Committee of Konan Hospital.
For model production, all data were converted to Digital Imaging and Communications in Medicine files using 3-D slicer4 ver. 4.5.0-1 (The Brigham and Women’s Hospital, Inc.). The 3-D reconstructed solid geometric models were subsequently imported into the engineering modeling software, solid modeling computer-aided design software—SolidWorks 2013 (Dassault Systems SolidWorks Corp., Vélizy-Villacoublay, France). The abductor muscle was outlined as a line connecting from the point of the outer surface of the ilium, and approximated as the center of the middle division of the gluteus medius to the tip of the greater trochanter, reflecting CT view of muscular attachment (Figure 2). The moment arm (effective lever arm) was defined as the 3-D length of a straight line originating from the center of femoral head and terminating at a point 90° to the gluteus muscle line. 10 Two basic models were prepared: model I (control model without displacement) and model II (simulated malunion of a 15° valgus-impacted fracture, no angulation at the lateral view, AO/OTA 31-B1.2). Two sets of hip flexion angles in each of the models were simulated from the alterations in hip flexion position in a gait cycle, that is, (1) flexion angle of 23° (heel touch) and (2) flexion angle of 0° (Figure 3). The flexion angle of these models was based on an electromyogram study that showed activity of the gluteus medius muscle elevated during (1) and (2) in a gait cycle. 11 Hip rotation and abduction–adduction were fixed at 0°.

A black line at the sagittal view of pelvis designating gluteus medius course.

Computerized models of the hip joint revealing model I, nondisplaced model (left) and model II, simulated malunion of a 15° valgus-impacted fracture (right). The dotted line represents gluteus medius. The left right arrow indicates the moment arm or distance from the center of femoral head to the gluteus muscle line.
Results
Clinical study
Mean age of the 15 patients at osteosynthesis was 78 years (range, 60–90 years), and the mean postoperative follow-up period was 19.5 months (range, 7–39 months). Two patients were male (13%) and 13 were female (87%). All the fractures were classified into AO/OTA 31-B1.1 1 for 3 patients and 31-B1.2 for 12 patients.
The mean and standard deviation values for muscle strength measured in different directions from the nonoperative/operative side are as follows: muscle strength during flexion was 9.2 ± 4.1/8.6 ± 3.3, strength at extension was 5.9 ± 2.6/6.0 ± 3.0, abduction strength at 0° was 8.5 ± 3.7/6.6 ± 3.7, abduction strength at 10° was 6.2 ± 3.1/4.8 ± 2.4, and knee extension strength was 14.6 ± 5.8/14.0 ± 5.7 (Figure 4). Upon comparison of values between the nonoperative and operative sides, only values for abduction strength at 0° and at 10° demonstrated statistical significance (p < 0.05).
Bar graph depicting differences in mean muscle strength between the nonoperative and operative side in all patients. Only the values for abduction strength at 0° and at 10° demonstrated statistical significance (p < 0.05).
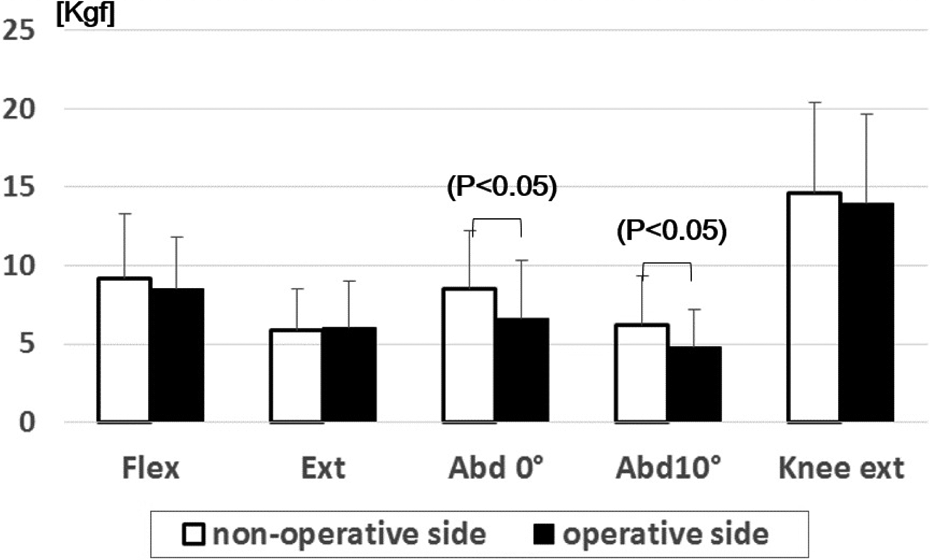
Regarding the valgus-healed group, mean age of the 12 patients was 78 years (range, 60–90 years) and the mean postoperative follow-up period was 21 months (range, 7–39 months). Only one patient was male. The amount of vertical shortening of the femoral head against the femoral shaft was 2.9 ± 2.5 mm (0.1–5.7 mm). Average valgus angle was 8.9° (ranging from 3.4 to 18.1). Mean and standard deviation values for muscle strength measured in different directions from the nonoperative/operative side are as follows: flexion strength was 9.2 ± 4.0/9.2 ± 3.2, extension strength was 5.8 ± 2.8/6.1 ± 3.2, abduction strength at 0° was 9.1 ± 3.7/7.4 ± 3.6, abduction strength at 10° was 6.7 ± 3.0/5.5 ± 2.2, and knee extension strength was 15.3 ± 6.2/15.1 ± 6.0 (Figure 5). When comparing values between the nonoperative and operative sides, statistical significance was only observed in abduction strength both at 0° and at 10° (p < 0.01).

Bar graph showing the values between the nonoperative and operative sides in the valgus-healed patients. Statistical significance was only observed in abduction strength both at 0° and at 10° (p < 0.01).
Biomechanical model
We measured the 3-D length of moment arm on the 3-D reconstructed solid geometric models. Moment arm measurements at a flexion angle of 23° were 47.9 mm in model I (control model without displacement) and 42.9 mm in model II (simulated malunion of a 15° valgus-impacted fracture). Measurements at 0° of flexion was 50.4 mm in model I and 45.3 mm in model II. The moment arm ratio between both models (model II divided by model I) was 0.896 at a flexion angle of 23° and 0.899 at 0° of flexion. These ratios prove that valgus impaction decreases the moment arm by approximately 10%.
Discussion
Femoral shortening in femoral neck fractures
In this study, an average femoral shortening of 2.9 mm (range, 0.1–5.7 mm) was observed in the valgus-healed group. Postoperative shortening at the fracture site is a common occurrence, as the configuration of parallel threaded screws allows for postoperative sliding which aids in accelerating and stabilizing bone healing. In a recent questionnaire involving 203 surgeons, majority (83%) reported that postoperative shortening of the femoral neck occurred commonly, despite ensuring direct bony contact between the proximal and distal fragments during surgery. 12,13 Song et al. 14 reported a mean femoral neck shortening of 3.7 mm in impacted fractures of less than 15°. Hence, these data show that minimal to moderate shortening of the femur occurs in valgus-healed femoral neck fractures.
Decrease in moment arm found in valgus-healed femoral neck fractures from biomechanical consideration
A valgus-impacted femoral neck fracture, due to its inherent stability, is difficult to correct by closed means. Treatment is usually in situ internal fixation, leaving the valgus deformity postoperatively. Several authors have reported that horizontal shortening of the femur may be related to alterations in the length of the hip abductor moment arm. 14,15
Though many surgeons recognize the importance of evaluating the moment arm, assessment by plain radiography may not always be accurate. First, radiographic evaluation of horizontal displacement would be unreliable as the amount of lower limb rotation changes with each radiograph. 14 Second, radiography can only provide a two-dimensional representation of a 3-D construct. Although radiographs can give an estimate of the changes in the moment arm, there is a need for a more accurate method of evaluation. 10 Our present biomechanical study using 3-D geometric model provides results of moment arm length. We have shown that the hip abductor moment arm shortens by approximately 10% with a 15° femoral neck valgus impaction.
Muscular strength and function decreases secondary to femoral shortening or valgus deformity
One of the key results documented by this current clinical research is that significant muscular weakness, especially during hip abduction, occurs on the operative side of the valgus-healed group, probably secondary to femoral shortening and decrease in the moment arm. In this study, several valgus-healed patients complained that they could not walk smoothly due to fatigue on the operated side. These statements are coincident with Song et al., 14 where the group with a greater degree of valgus impaction scored worse than those with less impaction in postoperative Harris hip score. These data suggest that diminished function was observed among valgus-healed group.
A recent multicenter study using a questionnaire demonstrated that patients with severe shortening of the femoral neck accompanied a significant reduction in hip abductor strength and postoperative function. 13 In another study of patients undergoing rehabilitation, diminished strength of multiple lower extremity muscles, including hip extensors and abductors, was shown to have a deleterious effect on gait speed and on maintaining upright balance during the stance phase of walking. 16 These two articles clearly demonstrate functional deterioration among postoperative patients with weakened muscles.
Not many orthopedic surgeons seem to give much attention or importance to examine postoperative muscular strength. In this study, the younger and more physically active patients did not notice weakened muscular strength during the outpatient follow-up period. This observation is in agreement with Zielinski et al., 13 where advanced age and a higher degree of disability lead to a more evident decrease in total muscle strength, as the surrounding muscles are unable to compensate and complement each other. We could rehabilitate the impairment, but muscular deficiency derived from diminished moment arm will expectedly remain. Some of our patients more than 10 years postoperatively also revealed declined muscular strength (not included in this 15 case series). Thus, surgeons should conduct examination of muscular strength in the daily outpatients practice to anticipate further presence of a functional impairment.
Limitations
There are several limitations to this study. First, the study design was retrospective with a small number of subjects for evaluation. In the current study, the number of patients was limited by the stringent inclusion and exclusion criteria. Moreover, the loss of patients in this geriatric age group is inevitable, which may diminish the weight of the results. 6,17,18 Second, blinding could not be applied to the study as the physicians and medical staff were aware of the laterality of the operated side. Third, in our study, the gluteus medius muscle was represented by a single line at the center of the middle fiber, since the maximal increase in the abductor moment arm is most evident in the middle fiber. 19 Future studies utilizing next-generation models consisting of several lines representing the gluteus medius muscle are necessary. Fourth, follow-up period was unequal in this retrospective study. However, our consecutive follow-up study more than 10 of these patients revealed continued decline in muscular strength in their majorities. Therefore, difference of follow-up period may not be influential in comparative result of bilateral muscular strength.
Conclusions and future direction
This preliminary study demonstrates that a valgus-impacted fracture may cause muscular impairment that can possibly lead to the postoperative functional disorder. Although a certain degree of femoral shortening is generally acceptable by surgeons, for some patients postoperative functioning is unsatisfactory. Further studies can compare between valgus-healed fracture and healed fracture with normal alignment. A novel approach involving the use of length stabilizing devices or fibular allografts that minimizes femoral shortening has been proposed 20 but still remains controversial. Afterward, we should investigate the limit of the valgus deformity to acquire satisfactory functional results.
Footnotes
Authors’ contribution
MN analyzed and wrote this manuscript. YS and MT frequently discussed about the content of the manuscript and guided the view and main course of the manuscript. Young fellows, YK and YT, took care and interpreted the data of these patients. CY and MW were not only chief contributors for the patients’ measurement but indicators of new finding among physical therapists. KA and YN contributed significantly for biomechanical research of 3-D measurement. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.