
Abstract
Purpose:
Distal radial extraarticular malunions are not uncommon. However, requirements of surgical correction depend on multiple conditions. Traditionally, surgical techniques include closing or opening wedge osteotomies. Each has unique advantages and disadvantages. An oblique osteotomy was developed to simplify the revision surgery.
Methods:
Forty-eight consecutive adult patients with 48 malunions were surgically treated. An oblique osteotomy of 45° vertical to the radial longitudinal axis was performed from medio-distally to latero-proximally. Consequently, the osteotomized fragments were compressed with a bone clamp. The proximal part of the distal fragment was pushed backward to correct the dorsal tilt. A 7-hole buttress plate was inserted volarly and cancellous bone graft was packed. Postoperatively, a short-arm splint or brace without restriction of all five metacarpophalangeal joints was applied for 6 weeks.
Results:
Forty-one patients were followed for an average of 2.8 years (range, 1.1–5.8 years). All malunions healed within 6 weeks. The union rate was 100% and no complications occurred. Radiographically, ulnar variance, volar tilt of radial articulation, and radial inclination restored to acceptable criteria in all patients. Patients with Modified Mayo Wrist Score (MMWS) improved from 17% to 80% (p < 0.001) and Disability of Arm, Shoulder and Hand (DASH) Score improved from 0% to 80% (p < 0.001). The relationship between MMWS and DASH Score was highly correlated (correlation coefficient = −0.90).
Conclusion:
The described approach may be an excellent alternative for treating distal radial extraarticular malunions. The technique is not difficult but the satisfactory rate is high.
Introduction
Distal radial fractures are common and may be caused by either low- or high-energy injuries. 1 Most patients are in old age and fractures may be associated with various degrees of osteoporosis. 2 Practically, displaced intraarticular fractures of the distal radius usually require surgical treatment to restore the articular surface. 3 Minimally displaced intraarticular or most extraarticular fractures of the distal radius normally are treated by closed reduction with stable immobilization. 1,4,5 The function outcome of the wrist is normally satisfactory.
However, some patients may undergo inadequate treatment and fractures become malunions. 4 –6 The wrist function may be immediately compromised or potentially deteriorated progressively. Intraarticular malunions generally cannot be treated predictively and the outcomes are uncontrollable. 7,8 Extraarticular malunions can be treated with various osteotomies. 9,10 After the alignment is restored, various external or internal devices may be used. The success rates may be as high as 83%. 11
An acceptable alignment of distal radial extraarticular fractures has been roughly reported. 4,5,12,13 In principle, the collapsed radius requires to be lengthened. Concomitantly, the three-dimensional frame requires to be restored. Consequently, an optimal stabilizing device is inserted. Postoperatively, the lesion site is well protected until bony union. The wrist range of motion (ROM) exercise is executed as early as possible. Although, in the literature a number of surgical techniques are advocated, none are absolutely convincing. Each technique has unique advantages and disadvantages. None can be confessed absolutely superior to others.
In the literature, an oblique osteotomy has been used in long bone lengthening, which can reduce bone graft amount for scaffold formation. 14 –16 Using a sliding technique, the bony lengthening can be finished easier. The aim of this retrospective study was to investigate using an oblique osteotomy to treat distal radial extraarticular malunions. Consequently, an ideal surgical technique might be recommended.
Materials and methods
From April 2005 to July 2014, 48 consecutive adult patients (≧18 years) with 48 distal radial extraarticular malunions were treated by the described technique at the author’s institution. The author singly treated and followed all patients. These patients aged from 21 years to 72 years (average, 46 years) with a male to female ratio of 3:5. Thirty-four malunions were in the right side and 14 in the left side. All malunions were caused by failed treatment of prior fractures. Prior fractures were caused by 31 low-energy injuries (fall or sliding) and 17 high-energy injuries (motorcycle or bicycle accident, or fall from heights). There were no open fractures. 17 Initial treatment included closed reduction with cast or brace immobilization in 23 fractures, closed reduction by bone setters in 19 fractures, and closed reduction with external fixation in 6 fractures. 1 The period from initial injuries to the described surgical treatment was an average of 3.6 months (range, 2.0–6.2 months). All patients asked for further treatment because of intolerable compromise of daily activity.
During the outpatients department (OPD), patients’ wrist and finger functions were examined thoroughly. Gross appearance, ROM, and grip strength were measured and recorded. Neurovascular complications were pursed. Posteroanterior and lateral views of wrist radiographs were taken (Figure 1(a)). Abnormal ulnar variance, volar tilt angle of radial articulation, and radial inclination were measured (Figure 1(b) and (c)). Plans of surgical approaches were explained to patients and families clearly. Surgical indications in this study were abnormal wrist and finger functions associated with at least one of unacceptable radiographic criteria (ulnar variance ≧5 mm, volar tilt angle ≧−10°, or radial inclination <15°). 4,5 Inclusion criteria of this study were all distal radial extraarticular fractures longer than 6 weeks, abnormal wrist and finger functions, and unacceptable radiographic criteria. Exclusion criteria were those malunions not treated by the described surgical technique.

Technical sequence: (a) a distal radial extraarticular malunion requires surgical treatment. (b) Ulnar variance is measured at posteroanterior view of the wrist radiograph. (c) Volar tilt angle of radial articulation is measured. (d) An oblique osteotomy of 45° vertical to radial longitudinal axis is performed from medio-distally to latero-proximally.
Surgical technique
All patients were anesthetized in the general route with endotracheal intubation. They were placed in the operating table in the supine position. A pneumatic tourniquet was routinely used.
Cancellous bone grafts about 3 ml were procured from the ipsilaterally anterior iliac crest first. A direct anterior skin approach was made at the distal radius. The anterior surface of distal radius with articular line was well exposed. An oblique osteotomy with 45° vertical to the radial longitudinal axis was performed using a power saw which is 2 cm proximal to the articular line from medio-distally to latero-proximally (Figure 1(d)). With a bone clamp, the osteotomized fragments were compressed (Figure 2(a)). The wrist was forcefully manipulated toward ulnar and volar directions, and the distal fragment slided medio-distally. The distance of lengthening was evaluated by trigonometric function. Although the osteotomy was uniplanar, after fragment reduction, the wrist and elbow were oriented in functional position. It was done as treatment of distal radius comminuted fractures without cortical contact. The elbow was flexed to 90° and the radius was rotated along the ulna to adjust the gross appearance. After fragments were temporarily immobilized with a bone clamp, the wrist ROM was checked. The proximal part of the distal fragment was pushed backward, which let the longitudinal axis of the distal fragment fit the desired correction of the volar tilt angle (Figure 2(b)). The wrist alignment was checked by an image intensifier. The dorsal aspect of the distal fragment was trimmed with a power saw and bone chips were transplanted to the volar aspect of the distal fragment (Figure 2(c)). A seven-hole buttress plate (Synthes, Bettlack, Switzerland) was bent and inserted on the volar aspect of the distal radius. Cancellous bone grafts were packed in the osteotomy site (Figure 2(d)). The wrist alignment was rechecked by an image intensifier. A short-arm splint in the ulnar side was applied and all five metacarpophalangeal joints were without restriction. After 2 weeks, a wrist brace was applied to replace the short-arm splint at the OPD.

(a) With a bone clamp, fragments are compressed and slide. (b) The proximal part of the distal fragment is pushed backward to restore volar tilt. (c) The dorsal cortex is trimmed and bone chips are transplanted to volar surface. (d) A seven-hole buttress plate is inserted and cancellous bone graft is packed.
Patients were followed at the OPD at 2 weeks and 6 weeks. The wrist brace was removed at 6 weeks and wrist ROM exercise was encouraged as tolerated. They were followed 3 months, 1 year, and whenever necessary. The clinical features and wrist radiographs were checked at each follow-up. The plate was normally not removed except patient’s insistence.
A bone union was defined as clinically, no pain and tenderness; radiographically, solid callus had connected both fragments. 18 A nonunion was defined as a fracture was still not healed after 1-year treatment or necessity of further surgical treatment to achieve a union. 19 A malunion was defined as a fracture being healed in unacceptable radiographic criteria. 4 –6
The wrist function was evaluated by Modified Mayo Wrist Score (MMWS) and Disability of Arm, Shoulder and Hand (DASH) Score. 20,21 The former was executed by the surgeon and the latter by patient himself. MMWS evaluated pain (25 points), satisfaction to work (25 points), active flexion–extension arc (25 points), and grip strength (25 points). It was divided into four grades and a satisfactory outcome consisted of an excellent or good grade (≧80 points). However, active supination–pronation arc was not evaluated. DASH Score included 30 items and each scored to five points. It was calculated as ([sum of n response/n] − 1) × 25, n ≧27 items. A total score was 100 points and an acceptable value was less than 20 points. 4,5,22
To compare the effects of surgical treatment, χ 2 test or paired Student’s t-test was used. P < 0.05 was considered statistically significant. Besides, Pearson product-moment correlation coefficient was used to investigate the relationship between MMWS and DASH Score.
Results
Forty-one patients were followed for at least 1 year (average, 2.8 years; range, 1.1–5.8 years). Seven patients were lost to regular contact despite the maximum efforts. All osteotomy sites healed within 6 weeks with a union rate of 100% (41/41, Figures 3 and 4).

Case 1: (a) A 43-year-old man sustained a right distal radial extraarticular malunion after failed cast treatment for 3.2 months. (b) The lesion was treated with the described technique. (c) A satisfactory wrist function was achieved for a 5.8-year follow-up.

Case 2: (a) A 56-year-old woman sustained a right distal radial extraarticular malunion after failed cast treatment for 2.5 months. (b) The lesion was treated with the described technique. (c) A satisfactory wrist function was achieved for a 5.4-year follow-up.
There were no peri and postoperative complications (deep infection, nonunion, malunion, and donor-site complications).
Preoperatively, the ulnar variance was an average of 9.6 mm (range, 5–12 mm). At the latest follow-up, it became an average of 1.1 mm (range, −2 to 3 mm, p < 0.001). Preoperatively, the volar tilt angle was an average of 0.8° (−7° to 8°). At the latest follow-up, it became an average of 2.0° (−3° to 6°, p = 0.10). Preoperatively, the radial inclination was an average of 14.1° (range, 5–22°). At the latest follow-up, it became an average of 19.8° (range, 15–27°, p < 0.001).
Preoperatively, the maximal active flexion of the wrist was an average of 25.6° (range, 10–60°). At the latest follow-up, it became an average of 58.5° (range, 40–80°, p < 0.001). Preoperatively, the maximal active extension of the wrist was an average of 25.4° (range, 10–40°). At the latest follow-up, it became an average of 46.6° (range, 30–60°, p <0.001). Preoperatively, the active flexion–extension arc of the wrist was an average of 44.3% of the contralateral wrist (range, 15–85%). At the latest follow-up, it became an average of 79.3% of the contralateral wrist (range, 70–95%, p < 0.001).
Preoperatively, the grip strength was an average of 56.3% of the contralateral wrist (range, 30–80%). At the latest follow-up, it became an average of 83.7% of the contralateral wrist (range, 70–95%, p < 0.001).
Preoperatively, the MMWS was an average of 45.9 points (range, 30–80 points). At the latest follow-up, it became an average of 78.5 points (range, 65–85 points, p < 0.001). Preoperatively, the DASH Score was an average of 36.3 points (range, 22–58 points). At the latest follow-up, it became an average of 16.5 points (range, 10–30 points, p < 0.001).
Satisfactory MMWS improved from 17% (7/41) to 80% (33/41, p < 0.001). Patients with unsatisfactory wrist function were due to mild ROM limitation, slight hindrance of working, and mild decrease of grip strength. Pain was minimal or unnoticed. Acceptable DASH Score improved from 0% (0/41) to 80% (33/41, p < 0.001, Tables 1 to 3). Patients with unacceptable DASH Score were associated with various degrees of limitation of daily or social activities.
Clinical data for patients with distal radial extraarticular malunions treated with the described technique (n = 48).

DASH: Disability of Arm, Shoulder and Hand; F: female; FEA: flexion–extension arc; M: male; RI: radial inclination; UV: ulnar variance; VT: volar tilt.
Clinical data for patients with distal radial extraarticular malunions treated with the described technique (n = 48).
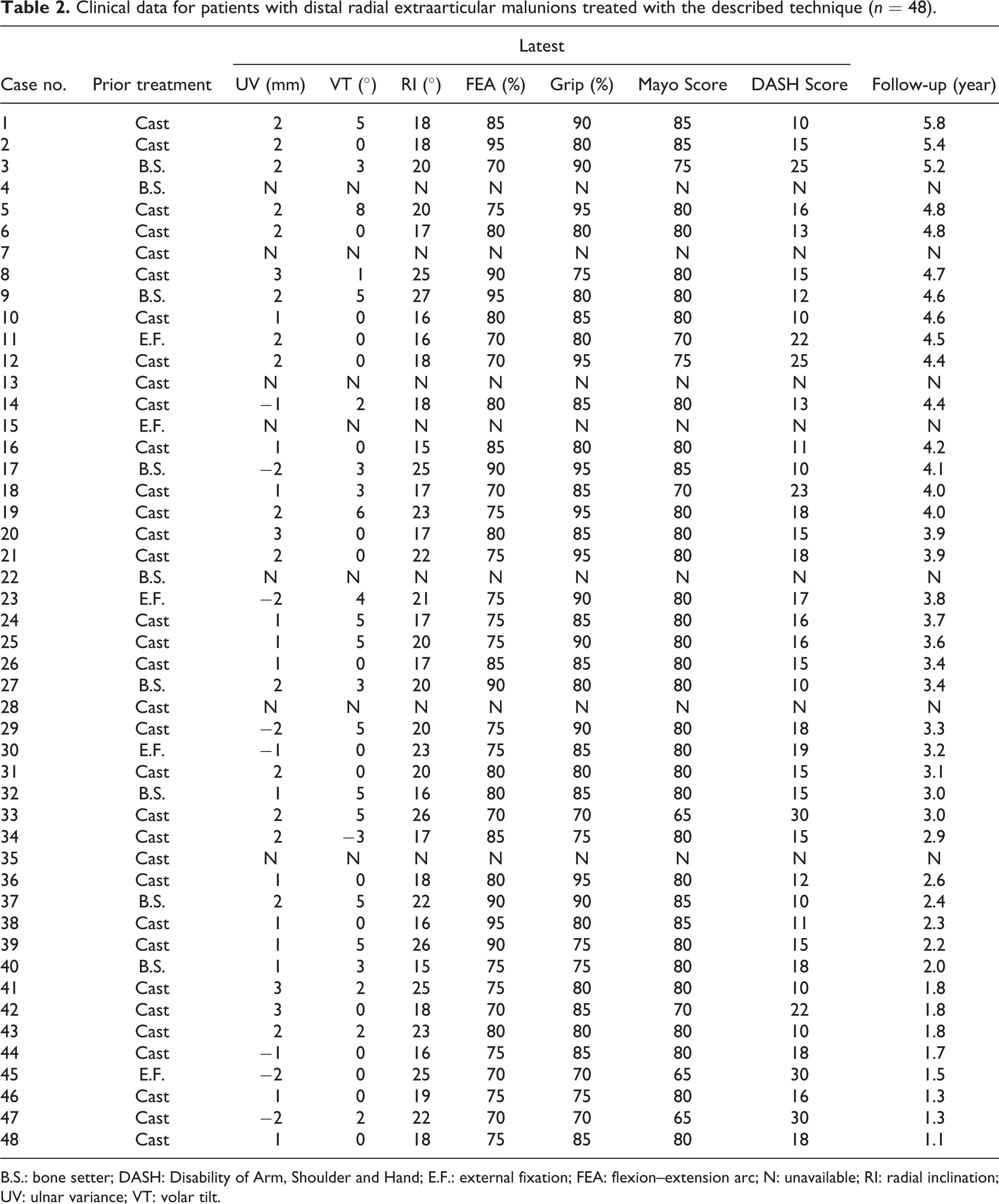
B.S.: bone setter; DASH: Disability of Arm, Shoulder and Hand; E.F.: external fixation; FEA: flexion–extension arc; N: unavailable; RI: radial inclination; UV: ulnar variance; VT: volar tilt.
Comparison of various parameters for preoperation and latest follow-up (n = 41).
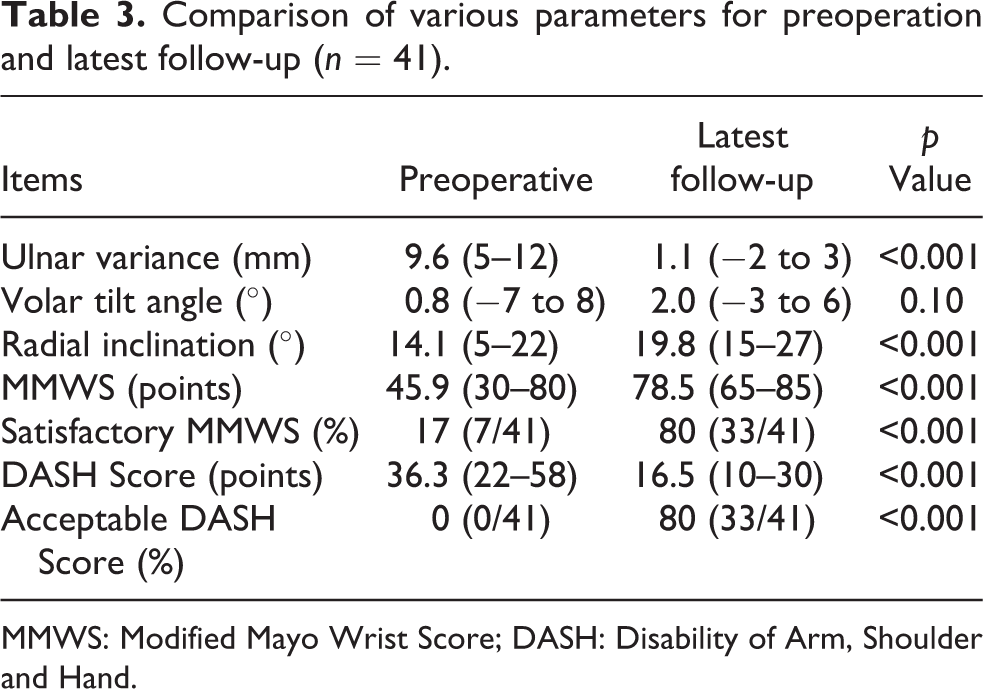
MMWS: Modified Mayo Wrist Score; DASH: Disability of Arm, Shoulder and Hand.
The preoperative relationship between MMWS and DASH Score was highly correlated (correlation coefficient = −0.92). At the latest follow-up, the relationship between MMWS and DASH Score was also highly correlated (correlation coefficient = −0.87).
At the latest follow-up, plates were removed in 34% (14/41) of patients and none were because of implant irritation.
Discussion
Biomechanical characteristics of the wrist have been thoroughly studied. 23 –25 The three-dimensional frame of the distal radius can deeply affect the wrist function outcomes. In the early stage of distal radial extraarticular malunions, the tendon pathway may be greatly rerouted. The wrist and finger functions may be greatly injured. In most situations, the collapsed distal radius introduces ulnar head impaction, and the trifibrocartilage complex is compromised. 4,5 The radial articulation with dorsal tilt may impair wrist flexion function. A decreased radial inclination may impair ulnar deviation function. In the current series, all three critical parameters (ulnar variance, volar tilt of radial articulation, and radial inclination) are totally corrected and wrist function achieves marked improvement. 26
A malunited distal radius with positive ulnar variance is commonly associated with distal radioulnar articulation diastasis. 4,27 The surrounding ligaments are stretched widely. To close a wide radioulnar articulation, an oblique radial osteotomy from medio-distally to latero-proximally is developed. After fragments slide with slant compression, the distal fragment migrates toward the ulnar head and ulnar variance is corrected concomitantly. With maintenance of the radial length, the proximal part of the distal fragment is pushed backward to restore volar tilt of radial articulation. In the current study, such a modified technique has restored an acceptable three-dimensional frame of the distal radius.
The orientation of the distal radius after fractures may be greatly changed. All three parameters may be involved concomitantly. Stabilization of acute fractures with internal or external devices requires the wrist in volar flexion and ulnar deviation. 28 Thus, all three parameters may be restored. However, for the malunited distal radius, the distal radius is generally collapsed with significantly increased ulnar variance and decreased radial inclination. As for volar tilt of radial articulation, the severity is generally mild because of prior treatment. In the current series, the preoperative volar tilt angle was an average of 0.8° (−7° to 8°). Therefore, correction is simple. The radial height is not studied in the current series. Anatomically, once the radial inclination is restored, the radial height generally become acceptable.
In the literature, distal radial corrective osteotomy may be performed by a closing or opening wedge technique. 4,5,9,10 Each technique has unique advantages and disadvantages and is suitable to various situations. A closing wedge osteotomy can correct dorsal tilt of radial articulation and requires no bone grafting. However, it cannot lengthen the collapsed radial fragment and concomitant ulnar shortening is often necessary. 6,9,29 An opening wedge osteotomy can provide a contrary effect but bone grafting is often necessary. Mahmoud et al. reported opening wedge osteotomy without bone graft in 30 patients. Twenty-two patients were followed and all osteotomy sites healed. Because of only a 73% follow-up rate, the reliability is doubted. 30 Furthermore, plate stability may be deeply injured. Plate loosening or breakage has occurred occasionally. 6,9,31 Prommersberger et al. reported that 55% of 49 opening wedge osteotomies had gross residual deformity. 31 In the current technique, fragments are connected closely and bone grafting is greatly reduced (for widening the osteotomy site). A traditional buttress plate is feasible and a locked plate is not always necessary.
Placing a plate on the distal radius volarly or dorsally has been debated. 4,5 Although placing a dorsal plate with an opening wedge osteotomy is easy for the collapsed and dorsal tilt radius, the plate can introduce many complications (extensor tendon impingement or rupture). 6,32 Currently, volar placement of a plate is favored widely. 6,9 In the current study, a buttress plate is placed volarly and no impingement is worried.
A postoperative short-arm splint or brace with all five metacarpophalangeal joints without restriction for 6 weeks should be reasonable. Normally, the local bone is somewhat osteoporotic, and the bone stock may be small. Steady stabilization of fragments may be unpredicted. Practically, a locked plate may be useful but its high price may restrict its wide use. Moreover, locked plate fixation may introduce a bulged mass because of mismatched bone-implant contours. 33 Especially, the locked plate is placed in the dorsal side to treat the collapsed and dorsal tilt radius with an opening wedge osteotomy. 32
In the current study, a high correlation between MMWS and DASH Score is found (p = −0.92 and −0.87, respectively) preoperatively and at the latest follow-up. For such lesions, both surgeons and patients may achieve a consistent viewpoint. In other words, either score may be studied only and follow-up can be simplified.
Limitations of the current study are as follows: (1) there is no randomized controlled comparison with other surgical techniques. Whether the current technique is superior cannot be concluded. However, theoretically and clinically the current study possesses its unique advantages and achieves a satisfactory result. The reliability of the current technique should be high. (2) The current study does not compare supination–pronation function of the wrist. It is because MMWS does not study supination–pronation arc. However, theoretically once three-dimensional frame of the distal radius is restored, ROM of the wrist can be restored in all directions. 9 (3) The current series had no patients with severe dorsal tilt radial articulation. The correction of dorsal tilt is therefore not statistically significant (p = 0.10). However, practically the described technique should be effective for most severe cases. (4) The satisfactory rate is not especially higher than that of other osteotomies. The purpose of the current study focuses on simplifying surgical procedures and a satisfactory rate is acceptable of around 80%.
In conclusion, the described approach may be an excellent alternative and an optimal choice for treating distal radial extraarticular malunions. The technique is not difficult but the union rate and satisfactory rate are high.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.