
Abstract
Background:
Despite being a common orthopedic injury, the optimal management of proximal humeral fractures remains a topic of debate. Although intramedullary nails have been used to treat these fractures, several complications have been reported with older nail devices. We describe our surgical technique and aim to evaluate the early functional and radiological outcomes of displaced Neer’s two- to four-part proximal humeral fractures undergoing fixation with a contemporary straight intramedullary nail.
Methods:
A prospective cohort study of 22 consecutive patients (mean age 55.7 ± 18.0) with acute displaced proximal humeral fractures underwent intramedullary nailing (Depuy Synthes MultiLoc Humeral Nail) by a single surgeon in a single institution. According to Neer’s classification, 11 had two-part fractures, 9 had three-part fractures, and 2 had four-part fractures. Functional and radiological outcomes, as well as occurrence of complications, were assessed at 12 months postoperatively.
Results:
The mean Constant–Murley score and American Shoulder and Elbow Surgeons score at 12 months were 75.5 ± 12.1 and 81.7 ± 6.2, respectively. Mean range of motion was forward flexion 144.3 ± 28.4, abduction 141.3 ± 30.5, external rotation 58.0 ± 13.9, and internal rotation 62.0 ± 15.2. Mean visual analog scale score was 1.7 ± 0.8. Radiographic fracture union was achieved at a mean of 3 months post-op. One patient underwent a second surgery for screw removal due to a proximal screw backing out. No other complications were found in our cohort. Notably, no patients had clinical signs and symptoms of subacromial impingement and/or rotator cuff tear.
Conclusion:
Our study demonstrated that intramedullary nailing using the contemporary straight nail design is well suited for Neer’s two- and three-part proximal humeral fractures, with good early outcomes and low rates of complications. Results for four-part fractures were, however, inferior in our cohort, suggesting that further studies with larger patient numbers are needed to determine the role of intramedullary nailing for four-part fractures.
Introduction
Fractures of the proximal humerus are common, accounting for 6% of all fractures. 1 Despite its prevalence, to date, the optimal management of proximal humeral fractures remains a topic of debate. 2,3 With the constant advancement in orthopedic implants and fixation techniques, there has been an increase in proximal humeral fractures treated surgically in recent years. 4 The goals of surgery are to obtain anatomical reduction and stable primary fixation to ensure fracture healing and allow early functional therapy without prolonged immobilization. 5 Among the many fixation methods available, proximal humeral locking nails are commonly used, with several studies showing similar outcome results compared to locked plating. 6,7 However, concerns remain regarding its complications, including rotator cuff injury. 8 –11 In view of this, newer generation intramedullary nails have been introduced in a bid to improve fixation and minimize these complications.
Our study aims to evaluate the early functional and radiological outcomes (up to 12 months) of displaced Neer’s two- to four-part proximal humeral fractures using a contemporary locking intramedullary nail design (Depuy Synthes MultiLoc Humeral Nail; Synthes GmbH, Oberdorf, Switzerland).
Methods
This prospective cohort study was conducted in a single center at Khoo Teck Puat Hospital (KTPH), Singapore. Approval from the local research ethics board was granted prior to initiation of the study. All patients provided written informed consent for their participation.
The MultiLoc (Depuy Synthes) Humeral Nail (short) was introduced and approved for use in our local health-care setting since the beginning of 2014. Between January 1, 2014, and August 1, 2015, patients who presented to KTPH with acute closed displaced proximal humeral fractures were recruited and evaluated for eligibility. Inclusion criteria were adult patients (aged 18 years and above) with an acute closed two- to four-part displaced proximal humeral fractures according to Neer’s classification (displacement >1 cm and angulation >45°). 12 Patients with ipsilateral upper limb fractures, pathological fractures, open fractures, and a delay in presentation of more than 14 days were excluded from our study.
A total of 28 patients who met the inclusion and exclusion criteria over the recruitment period agreed for surgery. Of these, six patients were deemed unsuitable for intramedullary nailing due to contraindications for the use of the nail, which included three- and four-part fracture dislocations, head split fractures as well as three- and four-part fractures in the elderly with tuberosity comminution. The latter group of patients would benefit from a shoulder arthroplasty instead. (Out of the six, two underwent open reduction internal fixation with a locking plate due to a head split fracture and a previous humeral shaft plating, respectively, whereas the remaining four underwent reverse shoulder arthroplasty due to tuberosity comminution and/or preexisting rotator cuff arthropathy.) The final number of patients who participated in our study was 22. They underwent intramedullary nailing using the MultiLoc (Depuy Synthes) Humeral Nail (short) by a single senior surgeon (second author).
Surgery was performed with the patient under general anesthesia with or without interscalene brachial plexus block in beach chair position with 45° elevation (Figure 1). A transdeltoid approach was utilized (Figure 2). Ethibond #5 sutures were routinely inserted through the cuff to control the tuberosity fragments in the setting of a three- or four-part fracture or to control the entire proximal humerus fragment in the setting of a two-part fracture. Having confirmed the ability to obtain adequate reduction with the manipulation of the tuberosity and head fragment, a longitudinal split was then made in the supraspinatus tendon over the most likely site of the nail entry point. The split was extended laterally, with care taken to prevent the violation of the cuff footprint at its insertion into the greater tuberosity. Through the cuff split, the entry point for the nail was then identified posterior to the intra-articular portion of the biceps tendon, and about 1.5 cm medial to the most medial edge of the greater tuberosity (also the head–tuberosity junction) in order to ensure rigid and firm purchase of the humeral head fragment, while avoiding damage to the supraspinatus insertion (Figure 3). After developing the entry point and passing the guidewire across the fracture site into the humeral canal under fluoroscopic guidance (Figure 4), the MultiLoc nail was then inserted. The tuberosity fragments, if separated from the head fragment in the case of a three- or four-part fracture, were then reduced anatomically with respect to the head and shaft and fixed with the proximal interlocking screws. The number of proximal interlocking screws (including the screw-in-screws) used for fracture fragment purchase was based on the fracture configuration and bone quality, ranging from three to five screws. We routinely made an attempt to insert the medial calcar screw, except in cases where it cannot be optimally positioned (Figure 5), typically in a small-sized Asian patient in whom the accommodation of a medial calcar screw into the most inferior aspect of the humeral head will inadvertently result in the protruding of the proximal end of the nail beyond the articular surface at the apex of the humeral head. Whenever possible, the stay sutures for the purpose of tuberosity fragment control were then tied to the suture holes on the interlocking screw heads to neutralize the pull of the rotator cuff, very much like how we utilize the suture holes of the proximal humeral locking plate. We believe this will aid tuberosity fixation especially in the case of tuberosity comminution or osteoporotic bone. The supraspinatus tendon split was finally repaired with nonabsorbable Ethibond #2 sutures (Figure 6). The deltoid fascia split was finally repaired.

Patient position on beach chair and optimal C-arm placement for intra-op fluoroscopy.
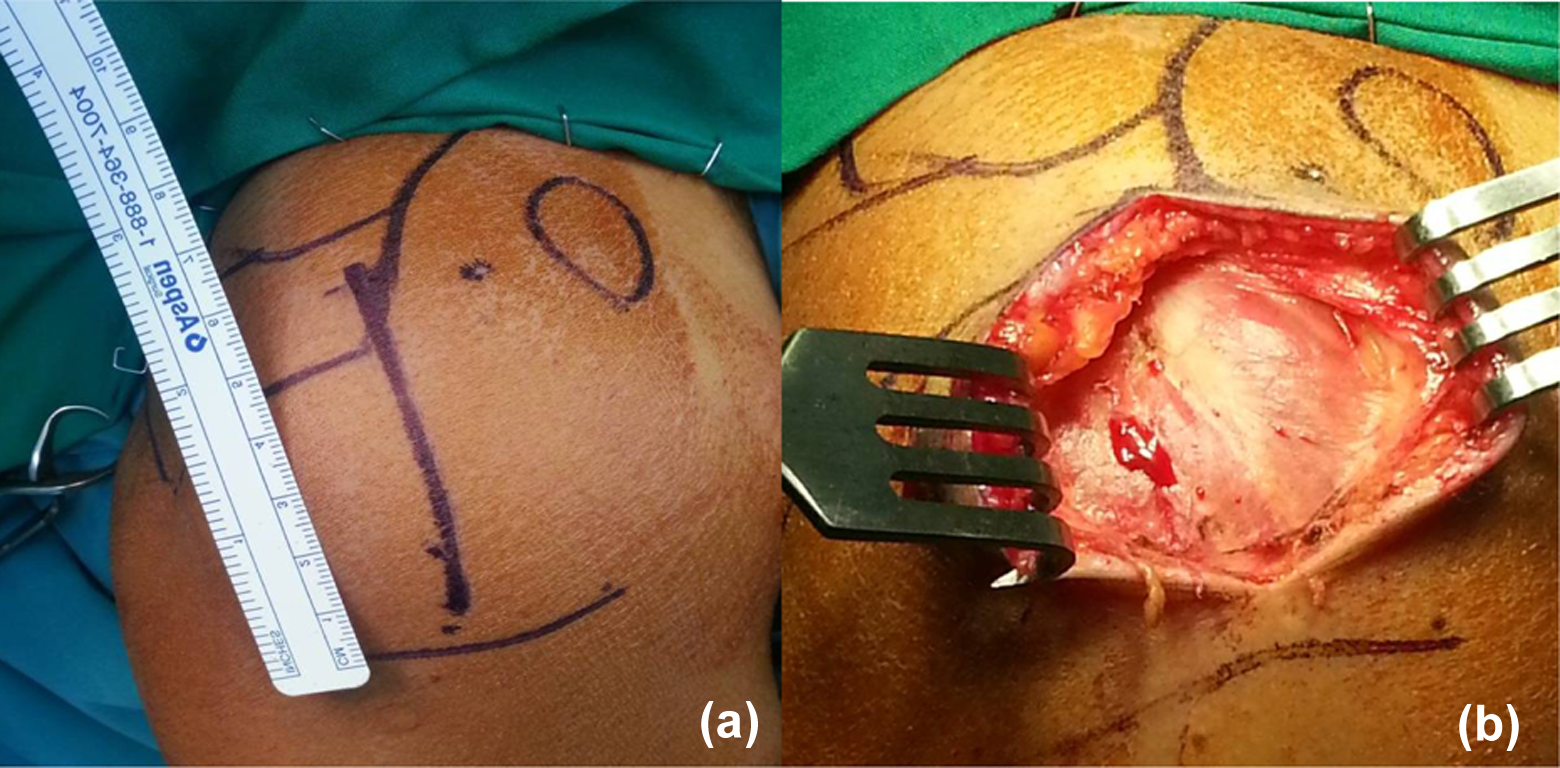
Incision (a) and identification of the raphe between the anterior and middle third of deltoid muscles (b).

Supraspinatus tendon split, identification of nail entry point on the apex of the humeral head, about 1.5 cm away from the cuff insertion onto the greater tuberosity.

Intra-op fluoroscopy images showing intramedullary nailing of a three-part fracture. Identification of entry point in the humeral head away from greater tuberosity, without the use of Kirschner wires to maintain anatomical reduction of head and tuberosities (a), guidewire cannulated through after opening ream (b), indirect reduction of the head fragment with nail insertion, and subsequent insertion of calcar screw (c), insertion of distal interlocking screw (d), insertion of proximal screws after reduction of tuberosity fragment using stay sutures (e).

Intra-op fluoroscopy image showing a case example of proximal humeral nailing where the calcar screw (indicated by the green line) cannot be optimally positioned due to the smaller Asian proximal humeral anatomy. Elevating the position of the nail in this case will result in nail protuberance at the entry point.
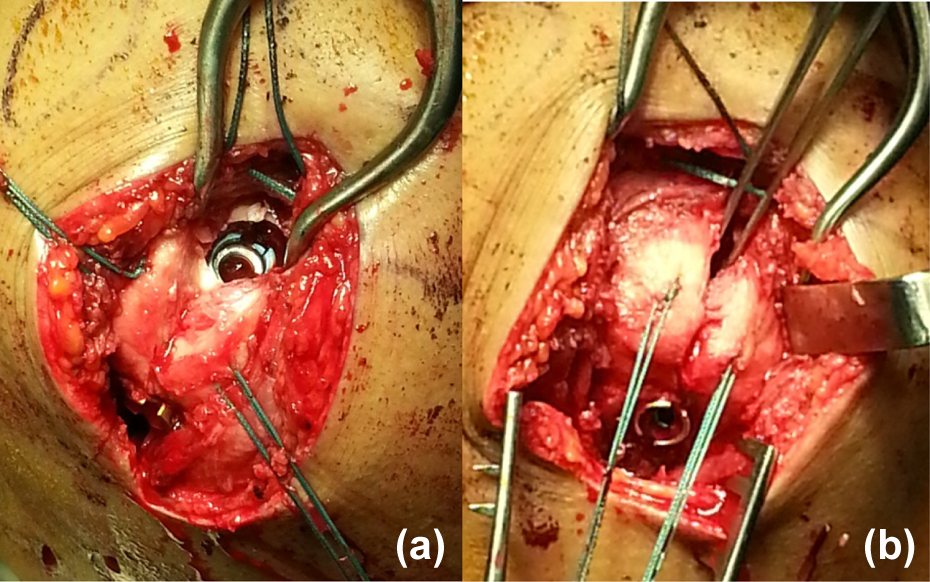
Position of the nail on the humeral head, away from the cuff insertion onto the greater tuberosity (a), use of Ethibond sutures to repair the supraspinatus split and augment tuberosity fixation through suture holes on the interlocking screws (b)
A sling was put on post-op and weaned progressively during the course of the first 6 weeks. Rehabilitation was initiated by the physiotherapist on the first post-op day, starting with pendular exercises for the first 2 weeks. From the third week onward, progressive passive- and active-assisted range-of-motion exercises, as tolerated by the patients, were started. Active range-of-motion and strengthening exercises were permitted from the sixth week onward, with the aim of regaining full range of motion as early as possible. All patients in our study were compliant with physiotherapy.
Patients were routinely followed up in the outpatient setting at 2, 6, and 12 weeks post-op and thereafter 3-monthly intervals up to 12 months for functional and radiological assessments. Functional outcomes were determined by using the Constant–Murley score and American Shoulder and Elbow Surgeons (ASES) shoulder score. Active range of movement of the injured shoulder was measured using a goniometer. External rotation was measured with shoulder adducted at the side, whereas internal rotation was measured with shoulder abducted at 90°. Assessment on clinical evidence of rotator cuff disease was performed based on strength on abduction, external rotation, and internal rotation, as well as the presence or absence of Neer’s and/or Hawkin’s sign, arc of pain, and supraspinatus tenderness. A visual analog scale (VAS) was used for assessment of pain. Radiographs of with three views—anteroposterior, lateral, and axillary—were obtained. Radiological outcomes were determined by two assessors based on evidence of union and time to union (months). Radiological union was determined when there is bridging callus in three out of the four cortices on radiographs. Neck–shaft angle was measured using the humeral shaft axis and line perpendicular to the articular segment or anatomic neck of the humerus.
Complications assessed included varus malunion (neck–shaft angle ≤110°), osteonecrosis of humeral head, nonunion, loss of reduction in tuberosities (displacement >5 mm), screw cutout or back-out, refracture, infection, neurologic injury, and clinical signs and symptoms of subacromial impingement and/or rotator cuff tendon tears.
Results
All 22 patients had a minimum of 12 months of follow-up. The mean age was 55.7 ± 18.0, with a male to female ratio of 7:15. In all, 12 of the patients sustained fracture on their dominant arm. According to Neer’s classification, 11 had two-part fractures, 9 had three-part fractures, and 2 had four-part fractures. A summary of study population demographic and injury characteristics is shown in Table 1.
Demographic characteristics of patient cohort.

Surgical data
The mean operative time was 97 ± 22 min. One patient was found intraoperatively to have a 3 × 2 cm full-thickness tear of the supraspinatus tendon (Figure 7). The nail was inserted through the cuff tear, and the tear was successfully repaired with nonabsorbable Ethibond #2 suture, followed by reattachment to the greater tuberosity using suture anchors at the end of surgery. No intraoperative complications were found. Mean hospital stay was 3 ± 2 days. One patient required post-op blood transfusion.

A 71-year-old female with two-part right proximal humeral fracture and intra-op findings of full-thickness supraspinatus tendon tear (a), which was repaired at the end of surgery (b).
Radiographic results
All fractures achieved union. Radiographic fracture union was achieved at a mean of 3 months post-op (Figure 8). The mean neck–shaft angle at 12 months was 129° ± 13°. No radiographic evidence of osteonecrosis of the humeral head was identified.

Preop radiographs (a and b) of a three-part proximal humeral fracture. Initial post-op (c and d) and 12 months post-op (e and f) showing fracture union without complication. The same patient demonstrating maximal abduction of his left shoulder 9 months post-op (g).
Clinical results
At 12 months post-op, mean Constant–Murley score and ASES score were 75.5 ± 12.1 and 81.7 ± 6.2, respectively. Mean range of motion was forward flexion 144.3° ± 28.4°, abduction 141.3° ± 30.5°, external rotation 58.0° ± 13.9°, and internal rotation 62.0° ± 15.2°. Mean VAS score was 1.7 ± 0.8. These are shown in Table 2.
Outcome results at 12 months post-op.
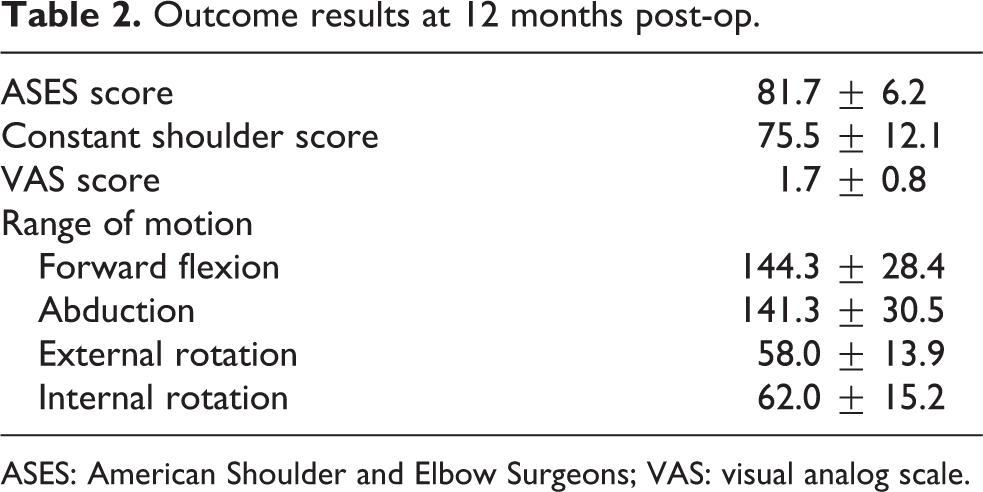
ASES: American Shoulder and Elbow Surgeons; VAS: visual analog scale.
Analyzing each group according to Neer’s classification, worse functional outcomes were observed in the four-part (Constant–Murley score 54.5 ± 7.8 and ASES score 71.7 ± 4.7) compared to the three-part (Constant–Murley score 83.5 ± 6.4 and ASES score 83.3 ± 4.7) and two-part groups (Constant–Murley score 80.0 ± 14.1 and ASES score 84.2 ± 3.5). However, our patient numbers were insufficient to make any conclusion of statistical significance.
Complications
One patient underwent a second surgery for screw removal due to a proximal interlocking screw backing out. No other complications were found in our cohort. Notably, no patients had clinical signs and symptoms of subacromial impingement and/or rotator cuff tear post-op.
Discussion
Multiple surgical fixation methods have been employed in the treatment of displaced proximal humeral fractures. These include percutaneous wire fixation, intramedullary nail fixation as well as plate fixation. The use of intramedullary nail is an attractive option, from both a biological and biomechanical standpoint. It has the proposed advantage of preservation of the periosteal blood supply and surrounding soft tissue envelope, and its intramedullary location confers greater biomechanical stability than other fixation techniques. 13 However, several complications such as avascular necrosis, proximal screw migration, loss of proximal fixation, malunion, infection, impingement, and rotator cuff pain and dysfunction have been reported. 14 –17 In particular, older, angled/curvilinear nail designs, such as the Polarus nail, were associated with high complication rate and reoperation rate. 18 –23 The introduction of new straight nail designs, such as the MultiLoc nail used in our present study, was aimed to address some of these complications. Its central insertion point was designed to (i) confer greater biomechanical stability by engaging the cranial part of humeral head which has higher bone density, (ii) avoid potential insertion through fracture site and causing iatrogenic greater tuberosity fracture, and (iii) reduce rotator cuff morbidity by avoiding the critical hypovascular zone of the rotator cuff at its insertion into the greater tuberosity. 24 –27 Furthermore, specifically for the MultiLoc nail, biomechanical studies have shown that the “screw-in-screw” option allows augmentation of proximal fixation through screw purchase in the strong posteromedial region of humeral head to counter varus collapse, and the ascending calcar screw provides extra support to the medial hinge, which could benefit the treatment of unstable proximal humeral fractures limiting the risk of secondary loss of reduction. 28 –30 The only direct comparison clinical study to date, Lopiz et al. further supported the use of the MultiLoc nail for proximal humerus fixation and showed that when compared to curvilinear nails, straight (MultiLoc) nail demonstrated lower rates of rotator cuff-related symptoms and reoperations. 31 Their findings of a favorable outcome and a low rate of complications was similarly observed in our study.
We are of the opinion that proximal humeral fractures that are nondisplaced or minimally displaced can be managed nonoperatively. In the senior author’s practice, about 50% of all proximal humeral fractures that he encounters are suitable to be treated nonoperatively. For displaced proximal humeral fractures, despite the Proximal Fracture of the Humerus Evaluation by Randomisation (PROFHER) trial. 32 Concluding that there was no difference in patient-reported clinical outcomes over 2 years between surgical and nonsurgical treatment, we are of the same opinion as other authors who have highlighted the limitations of the PROFHER study and prefer surgical treatment in this group of patients, more so for younger patients who is fit from an anesthetic point of view. 33 With specific relevance to our study, it should be noted that in the PROFHER study, the majority of the patients who received surgery underwent plate fixation, with only 4 out of 109 underwent intramedullary nailing. Hence, the findings of that study should not be extrapolated to imply that displaced proximal humeral fractures treated with intramedullary nailing and nonoperative treatment will result in similar outcomes. It should also be noted that in the surgical arm of the PROFHER study, none of the patients underwent reverse shoulder arthroplasty. It is increasingly recognized that the reverse shoulder arthroplasty provides a more predictable functional outcome over hemiarthroplasty for the treatment of displaced, comminuted proximal humeral fracture in the elderly. 34,35
The question of whether all proximal humeral fractures are suitable for intramedullary nailing remains a subject of debate, as several studies have shown contrasting results. Similar to our study, most authors reporting on the use of an intramedullary device for the treatment of proximal humeral fractures do not recommend nor include head split fractures and fracture dislocations in their series. In terms of the fracture types suitable for intramedullary nailing, Zhu et al. advised to limit its use to two-part surgical neck fractures with an intact proximal osseous ring. 7 Likewise, Bernard et al. reported a 45% reoperation rate in three- and four-part proximal humerus. 21 On the other hand, Konrad et al. demonstrated equivalent outcomes with plate compared with nail fixation of three-part proximal humeral fractures. 6 This is supported by a recent randomized controlled trial which concluded that locking plates and locking intramedullary nails produce similar results for two- and three-part surgical neck fractures. 36 Noticeably, four-part fractures seem to have the worst results. 8 It has to be noted that the majority of our patients (20 out of 22) had two- or three-part fractures. While we note that our two patients with four-part fractures had worse outcomes compared to those with two- or three-part fracture, our numbers are insufficient to arrive at any well-substantiated conclusion. It is the senior author’s personal opinion and observation since he started using the MultiLoc nail that the patients with displaced proximal humeral fractures who benefit most from the use of MultiLoc nail were those with two- or three-part fractures. Compared to his past experience in fixing these fractures with the proximal humeral locking plate prior to the introduction of the MultiLoc nail, the main benefit seems to be the much earlier return of motion and lower complication rate. This unsubstantiated observation of ours is echoed by other authors who reported less pain in the early postoperative period 6 and a lower complication rate 7 with the use of the nail to treat displaced proximal humeral fractures.
Although the authors who first described the surgical technique with regard to the use of the MultiLoc nail recommended the use of Kirschner wires for the maintenance of fracture reduction, 37 we find this challenging in the setting of comminuted and osteoporotic bone. We also find the maintenance of fracture reduction with multiple Kirschner wires prior to creation of the nail entry point difficult, and the subsequent nail insertion with multiple wires in situ challenging. We prefer the use of multiple strong Ethibond #5 sutures to initially control the individual fracture fragments and to obtain satisfactory and transient reduction on fluoroscopy. Without maintaining fracture fragment reduction with wires, we then pull our cuff sutures, and indirectly the head fragment, laterally out of varus to allow access to the entry point for the straight nail, which is relatively more medial than that for older nail designs. Once the entry point of the nail is developed and the guidewire cannulated across the fracture, we then introduce the nail, which indirectly reduces the head with respect to the shaft. In the case of a displaced two-part fracture, which is typically displaced in a varus direction, this indirect reduction maneuver is extremely effective in achieving and maintaining anatomical reduction, and relatively easy to perform. We acknowledge the potential danger of nonanatomical reduction of the head to shaft using this indirect reduction technique, but with familiarity, we find it possible to identify the correct entry point of the nail without prior anatomical reduction with Kirschner wires.
There are several limitations in our study. Due to our limited sample size, we were unable to perform statistical analysis for comparison among the groups. As our patients only had a short follow-up period of 12 months, we could potentially underreport the incidence of avascular necrosis of humeral head in our study. Nevertheless, it remains contentious if the occurrence of avascular necrosis is always predictive of a worse clinical outcome. 38 Lastly, even though none of our patients experienced symptoms and signs of subacromial impingement and/or rotator cuff tear postoperatively, the exact incidence of iatrogenic rotator cuff tear, reported to be as high as 13% by Gracitelli et al., 36 was unclear in our study as no magnetic resonance imaging or ultrasound imaging was performed to assess the integrity of the rotator cuff postoperatively.
Despite these limitations, we do feel our study has its merits and hence worth reporting. As to our knowledge, this is the first study reporting on the use of the MultiLoc nail for the treatment of proximal humeral fractures in an Asian population. This is important for two reasons. First, plate fixation for proximal humeral fixation remains the most common fixation method in this region despite its notable failure rates, 39,40 and the need for an alternative device is long overdue. Second, the use of the MultiLoc nail in an Asian population in our study raises a technical point that may have subsequent implications in subsequent proximal humeral nail designs, specifically the location of the medial calcar screw in relation to the proximal tip of the nail, to ensure better adaptability to the smaller Asian anatomy. Our technique of achieving and maintaining fracture reduction is also different from what has been described in the literature and hence worth sharing. Last but not least, we believe our study further supports the current literature evidence of a favorable outcome for Neer’s two- and three-part displaced proximal humeral fractures when treated with a contemporary intramedullary nail. It is currently the fixation device of choice in our practice when faced with these fracture types.
Conclusion
Our study demonstrated that intramedullary nailing using the MultiLoc nail is well suited for displaced Neer’s two- and three-part proximal humeral fractures in our Asian population, with good early functional and radiological outcomes as well as low rates of complications. Results of four-part fractures were, however, inferior in our cohort, suggesting that further studies with larger patient numbers are needed to determine the role of intramedullary nailing for four-part fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.