
Abstract
Purpose:
The aim of this study was to compare functional results before and after lunatum excision and scaphocapitate arthrodesis (SCA) using an angular stable circular plate in patients with Lichtman’s stage IIIB Kienböck’s disease.
Methods:
The study included nine patients (six females and three males) with a mean age of 33.2 ± 11 years (range: 18–54 years). Clinical and radiological assessment before and after surgery included wrist extension and flexion, range of motion and grip strength, visual analogue scale (VAS) score to assess pain, modified Mayo wrist scores, and measurements of the scapholunate (SL) angle and modified carpal height ratio.
Results:
The mean follow-up period was 17.33 ± 4.69 months (range: 12–24 months), mean operation time was 56.67 ± 12.5 min (range: 45–75 min) and mean hospitalization time was 3.44 ± 1.13 days (range: 2–6 days). Preoperative mean wrist extension was 23.89° ± 4.17°, mean wrist flexion was 32.22° ± 5.07°, mean grip strength compared to the healthy side was 34% (range: 28–37%) and mean VAS score was 7.6 (range: 7–8). Modified Mayo wrist scores were poor in all of the nine patients. Post-operative mean wrist extension was 27.78° ± 4.41°, mean wrist flexion was 40.56° ± 4.64°, mean grip strength compared to the healthy side was 71% (range: 63–81%) and mean VAS score was recorded as 1.4 (range: 1–2). Modified Mayo wrist scores were good in five and moderate in four patients. No patients had non-union or additional surgery.
Conclusion:
Lunatum excision and SCA using angular stable circular plate fixation provide pain relief with acceptable preservation of the range of motion.
Introduction
Osteonecrosis of the lunatum, known as Kienböck’s disease, was first described in cadavers by Peste, 1 and its radiological characteristics were expounded by Kienböck. 2 The aetiology of Kienböck’s disease is not fully known; however, mechanical, vascular and traumatic causes are thought to play a role. In recent years, although regional vascular and anatomic causes have been considered responsible, there is little clear information on the course of the disease. 3
Following the collapse of the lunatum in Kienböck’s disease, arthrosis develops in the wrist. These changes in the wrist are characterized by limited range of motion and pain in the radioulnar dorsal region. Although there is no consensus on the subject of treatment, surgical treatment is recommended for symptomatic patients. 4 Surgical methods that decrease the load on the lunatum and biological methods that provide revascularization and salvage operations have all been reported. In literature, a significant increase in functional scores has been obtained after surgical treatment regardless of the surgical approach. 5
This study explored the clinical and radiological results pertaining to the application of angular stable circular plate with scaphocapitate arthrodesis (SCA) and lunatum excision in Kienböck’s disease.
Patients and methods
The present study included patients who underwent surgery between April 2012 and January 2014 for grade IIIB Kienböck’s disease according to the Lichtman classification 6 (Figure 1). Patients were excluded if disease grading was other than grade IIIB of the Lichtman classification, if there had been additional prior treatment, if they were asymptomatic or if there had not been a regular follow-up.

Preoperative radiographies and magnetic resonance imaginations: A 54-year-old woman referred to us with pain at left wrist. At the lateral (a) and anteroposterior (b) radiographies, lunatum has collapsed and capitatum has migrated to the proximal. (c) Hyperintensity has been seen at the magnetic resonance T2 weight imaginations, and (d) lunatum has collapsed at the magnetic resonance T1 weight imaginations.
The standard treatment protocol was applied to all patients included in the study by a single surgeon. The skin incision was made with a dorsal longitudinal incision was made and the collapsed lunatum was excised. Then, the scaphocapitate joint cartilage was removed with mini-rounger, the scapholunate angle (SL) was decreased to normal values (30°–60°) and using an angular stable circular plate (Hub Cap Fusion Plates, Acumed®, Hillsboro, OR, USA), SCA was performed. Scapholunate angle and position of the arthrodesis was controlled with the image intensifier. To increase the success of arthrodesis, spongeous autograft taken from the iliac wing was grafted to the arthrodesis site. Intravenous cefazolin sodium 3 × 1 g was administered as prophylaxis 30 min preoperatively and was continued for 24 h post-operatively.
Post-operatively, the wrist was immobilized in a short arm brace extending to the palmar crease to allow free motion in the metacarpophalangeal joint. The patients were encouraged to start elbow and metacarpophalangeal joint motion, and the brace was discontinued at 4 weeks. Then, passive wrist joint exercises were started. At the end of the eighth week, active and forced wrist movements were permitted under the control of an experienced hand physiotherapist.
Modified carpal height ratio and ulnar variance were examined on the radiographs. Computed tomography (CT) imaging was performed at the final follow-up examination to evaluate the fusion site (Figure 2). In the evaluation of clinical results, the preoperative and final follow-up examination values of wrist joint extension and flexion movement angles, grip strength, modified Mayo wrist score 7 and visual analogue scale (VAS) pain scores were compared. Pain assessment was carried out by the experienced hand physiotherapist by using a visual chart.
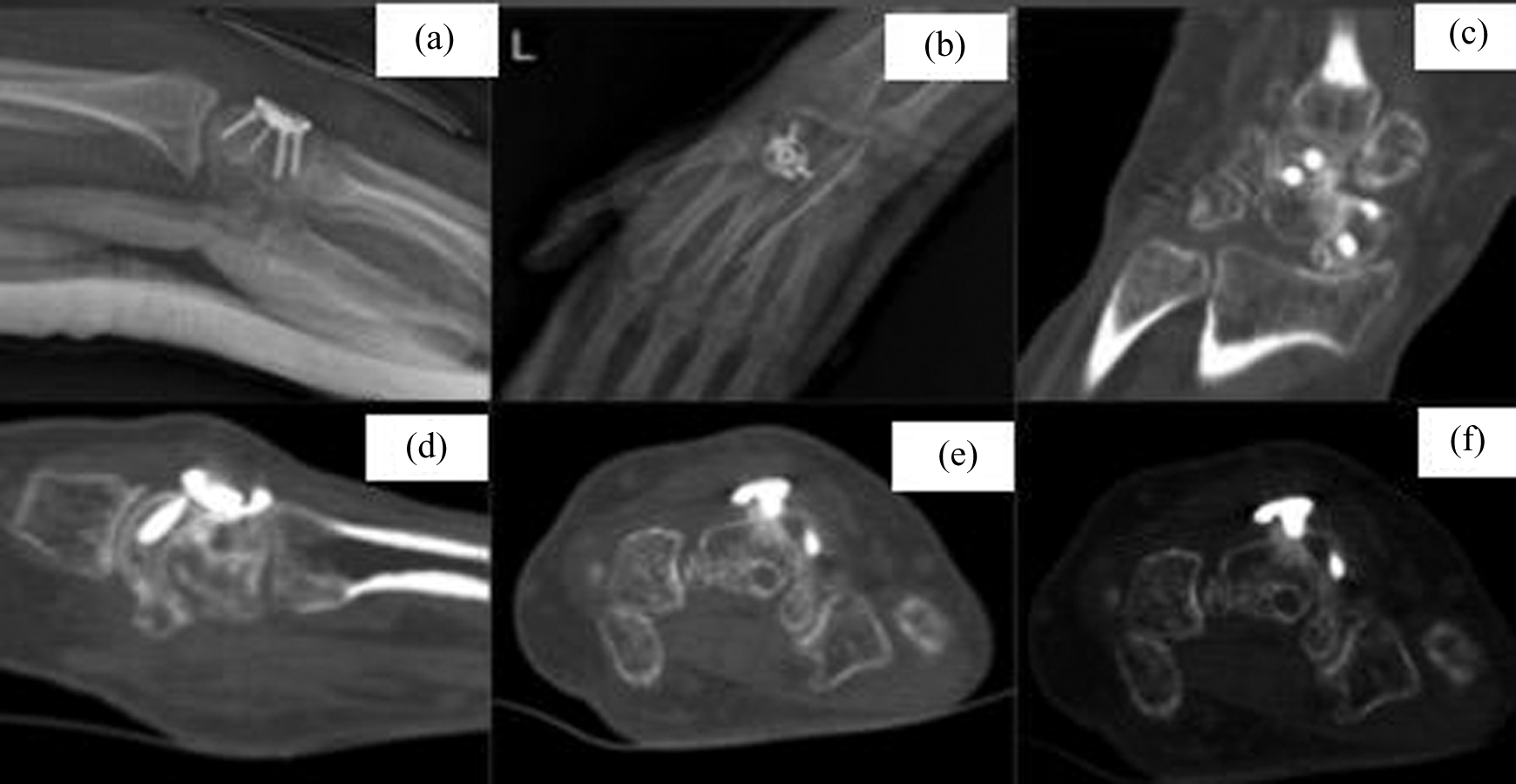
Post-operative radiographies and CTs: Early post-operative lateral (a) and anteroposterior (b) radiographies of lunatum excision and SCA using an angular stable circular plate have been showed. (c), (d), (e) and (f) Post-operative CTs have showed the fusion. SCA: scaphocapitate arthrodesis; CTs: computed tomographies.
Statistical analyses of the data obtained in the present study were conducted using the IBM SPSS Statistics 22 programme (IBM SPSS). When evaluating the study data, descriptive statistical methods (mean, standard deviation and frequency) were used. In the comparisons of quantitative data, the Wilcoxon sign test was used in the comparison of within-group parameters, both pre- and post-treatment. A value of p < 0.05 was accepted as statistically significant.
Results
The study included nine patients (six females 66.7% and three males 33.3%); the mean age was 33.22 ± 11 (range: 18–54 years). The right side was operated in two (22.2%) patients and the left side in seven (77.8%) patients. None of the patients were bilateral. The duration of hospital stay was on average 3.44 ± 1.13 days (range: 2–6 days), and the operating time was recorded as 56.67 ± 12.5 min (range: 45–75 min). The mean duration of follow-up was 27.33 ± 4.4 months (range: 24–36; Table 1). Solid fusion was seen on CT images in all patients at the end of 12th week.
Patient demographics and operative details.

SD: standard deviation.
After surgery, wrist extension increased from 23.89° ± 4.17° to 27.78° ± 4.41°, and wrist flexion increased from 32.22° ± 5.07° to 40.56° ± 4.64° (p < 0.05). Compared with the healthy side, the range of movement of the wrist was determined as a preoperative mean flexion 51.85° ± 7.81° and extension 43.33° ± 8.17°, and post-operative mean flexion of 65.34° ± 7.88° and extension 50° ± 16.51° (Table 2).
Radiological and clinical results.

Preoperatively, all nine patients had poor scores on the modified Mayo wrist score assessment; post-operatively, five (55.6%) patients were determined as good and four (44.4%) patients as fair based on the modified Mayo wrist score.
Grip strength values, percent of the healthy side, were determined to be 33.67 ± 2.96 and 71 ± 6.4 preoperatively and post-operatively, respectively (p = 0.008).
Post-operative VAS scores were significantly lower than preoperative scores (post-operative: 1.44 ± 0.53 and preoperative: 7.67 ± 0.5, p = 0.005; Table 2).
All of the patients were ulna negative variance. No statistically significant difference was observed between the pre- and post-operative values of the modified carpal height ratio (p = 1.000; Table 2). The post-operative SL measurements were determined as statistically, significantly lower than the preoperative SL measurements (55 ± 6.61–75.56 ± 5.27; p = 0.007; Table 2). The preoperative disease stage did not change post-operatively.
Discussion
The aetiology of lunatum osteonecrosis, known as Kienböck’s disease, is not fully known, particularly in patients with Lichtman grade IIIB Kienböck’s disease where loading on the lunatum is increased after scaphoid flexion; it has been shown that this increased load causes rapid collapse, thus accelerating the course of disease. 8 Advanced grade III and IV Kienböck’s disease has been successfully treated with lunatum replacement, lunatum excision, proximal row carpectomy, wrist fusion and limited carpal fusion. 9,10
In a study by Watanabe et al., although no osteoarthritic changes were observed on the radiological examination of grade IIIB Kienböck’s disease, cartilage damage was observed arthroscopically in the radiolunate joint. This pathology also occurs in the capitolunate joint. 9 Following that study, as proximal row carpectomy was not observed to be completely appropriate, lunatum excision and intercarpal arthrodesis, as recommended by Nakamura et al., were emphasized as more suitable. 10 Takase and Imakiire subsequently reported lunatum excision together with intercarpal arthrodesis as successful treatment for Kienböck’s disease. 11
In limited intercarpal arthrodesis (LCA), the aim is to fix the scaphoid bone in an appropriate position in arthrodesis between the carpal bones, thus preserving the carpal height and decreasing the load on the lunatum. 8,12,13 Scaphoid–trapezium–trapezoid (STT) arthrodesis 14,15 and SCA 16 –18 decrease the load on the lunatum in Kienböck’s disease. However, although symptomatic relief is provided by another LCA method of capitatum–hamatum arthrodesis (CHA) in Kienböck’s disease, there is no change in carpal loading. 19 In biomechanical studies, it has been shown that besides CHA, a significant decrease in loading on the lunatum was achieved in SCA and STT arthrodesis. 20 Li et al. stated in a recent biomechanical study that compared with SCA, STT arthrodesis has much greater value in preventing rotatory semidislocation of the scaphoideum, as well as in maintaining the stability of the wrist. 21 In the present study, SCA was applied following lunatum excision in all patients without significant change in carpal height.
SCA has been defined as a method in which outcomes as successful as those of STT are obtained. 13 In this technique, the non-union rates are halved. 8 This method has been shown to provide effective treatment with low rates of non-union and can be applied arthroscopically in combination with other techniques. 8,22 However, radiographic signs of radioscaphoid arthritis were often observed in patients with long-term follow-up. 23 Long-term follow-up in our study is needed to determine this complication.
In SCA, wrist flexion has been shown to be decreased by 43–54% and wrist extension by 40–54% compared with the unaffected side. 8,13,24 This decrease in wrist joint range of movement has been reported to be less that in STT arthrodesis. 25 Grip strength has been shown to increase with SCA. This increase has been reported as 75–151%. 8,13,24 In the present study, a statistically significant increase was achieved in grip strength and wrist joint range of movement with LCA, but did not match the levels of range of movement and grip strength of the unaffected side. Statistically significant positive changes were observed in patient satisfaction and the pain scale.
In several studies, it has been reported that the wrist could progress to arthrodesis given the high complication rate together with LCA. 26 In studies where a corticocancellous autograft with a screw or staple has been used in SCA, revision surgery has been required at different frequencies due to non-union. 8,13,22,27,28 The main reason for this difference in fusion rates reported in the literature may be insufficient stabilization at the fusion site. In comparative studies by Tambe et al., high rates of non-union were reported in LCA with K-wire or screw fixation. 26 When rigid fixation of the fusion was done with grafting, problems related to non-union were decreased to a minimum. In the present study, fixation was obtained with the use of the special plate, and successful arthrodesis was achieved. Furthermore, 100% union was achieved in all patients with the same surgical approach.
Limitations of the present study were low sample size and the retrospective nature of the evaluation. Multicentre studies could increase the number of patients and together with comparative studies would be beneficial to show the effectiveness of this treatment.
Conclusion
With the use of an angular stable circular plate in SCA and lunatum excision, successful functional results can be obtained with low rates of complications and high rates of union.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.