
Abstract
Purpose:
Hamstring graft fixation on the patellar side during medial patellofemoral ligament (MPFL) reconstruction is usually with transosseous tunnels and can frequently lead to further problems. The aim of our study was to compare and analyse patellar complications in single patellar tunnel versus double tunnel hamstring graft fixation.
Methods:
Twenty-nine knees with MPFL reconstructions (group S) in which the hamstring tendon graft was transfixed using a suspensory fixation method in a single tunnel drilled across the patella were analysed in comparison with 29 knees (group D) with interference fixation of the graft through two tunnels drilled up to a predetermined depth in the patella. Primary outcome measured was any patellar complication like anterior knee pain and patella fracture. Secondary outcomes assessed were future functional instability and failure of reconstruction.
Results:
Anterior knee pain was noted in six patients in group S, of which three patients had removal of the irritating metalwork on the patella. In all, nine surgical interventions were needed in six patients in this group. Three patients in group D complained of knee pain, but no one in this group needed any further surgical interventions (p value 0.02). Symptomatic instability requiring revision surgery or realignment surgery was required in two patients in the group S and none in group D. No patellar fractures were seen in either group.
Conclusion:
Our study showed increasing problems with single tunnel patellar fixation, with more reoperation and failure rates compared to double tunnel fixation. The evidence supports the move towards anatomical double bundle MPFL reconstructions.
Introduction
Traditionally recurrent patellar instability was surgically managed with lateral retinacular release, trochleoplasty, proximal or distal realignment surgery or a combination of these. With the knowledge that the medial patellofemoral ligament (MPFL) is the primary lateral restraint for the patella, and that it is invariably damaged at patellar dislocation, MPFL reconstructions have become more popular to address recurrent patellar instability. 1
Despite several large series of MPFL reconstructions have reported good success rates in addressing patellar instability, 2,3 , there is a significant rate of complications associated with the procedure. 4
Improved understanding of the anatomy and biomechanics of the ligament has, in recent years, shifted the technique from isometric single bundle to a more anatomical double bundle reconstruction. 5,6 Comparative studies of single versus double bundle reconstructions have focussed primarily on the functional outcomes. With the change in the patellar fixation technique, more insight is needed into patellar complications like anterior knee pain, metalwork irritation and patellar fractures. The aim of this article is to analyse the patellar complications in single patellar tunnel graft fixation in comparison with the double tunnel method.
Material and methods
All patients with recurrent patellar instability referred to our specialist knee unit who failed to improve with conservative treatment were listed for MPFL reconstructions. Clinical history and examination, along with standard knee radiographs, were part of the assessment. Patients who had increased Q-angle were further investigated to assess their tibial tuberosity–trochlear groove (TT-TG) distance. Knees with TT-TG greater than 20 mm and/or excessive Q-angles warranted tibial tuberosity transfer (TTT) procedure in addition to MPFL reconstruction. Patients with tight lateral retinaculum (less than one quadrant medial shift) or positive J-sign had lateral retinacular release (LRR) at the time of the reconstruction. None of the patients had generalized ligamentous laxity or a severe trochlear dysplasia.
Our retrospective study looked at all MPFL reconstructions performed since January 2006 to May 2015 by two specialist knee surgeons (Table 1). In the initial years, the looped hamstring tendon graft was suspended in a medial to lateral transpatellar 4.5 mm tunnel with the Endobutton CL Fixation Device (Smith &Nephew, Huntingdon, UK). Since 2013, we have modified the patellar fixation to a double tunnel technique using the two 4.75 mm BioComposite SwiveLock anchors (Arthrex, Sheffield, UK).
Patient demographics.
All procedures were done using ipsilateral hamstring graft, which was harvested first. Gracilis tendon was used in all patients except in one patient in group D, where the semitendinosus was used. After arthroscopic assessment through the standard two portals, any other intra-articular pathology was dealt with as necessary. Table 2 shows the associated procedures required in each group. A 3–5-cm medial patellar incision was made and bony tunnel prepared. In group S, the 4.5 mm tunnel was drilled at the medial border of patella at the upper and middle third junction. In group D, two 4.5 mm transverse tunnels are drilled up to a depth of 25–35 mm from the medial patellar margin. The first tunnel is approximately 5 mm distal to the superior-medial corner of the patella and the second tunnel is 15–20 mm distal and parallel to the first. Extra-synovial graft fixation on the femoral side was as described by Howells et al. 2 with fluoroscopic guidance as necessary. The graft was fixed to the femoral tunnel at about 30° of knee flexion using a biodegradable interference screw. All patients were protected in a knee splint for 2 weeks but were allowed full weight as tolerated. An accelerated physiotherapy programme was initiated on discharge from hospital and patients followed at 6 weeks and 6 months post-operatively and then subsequently as necessary (Figure 1a–b).
Associated surgical procedures.

TTT: tibial tuberosity transfer; LRR: lateral retinacular release; ACL: Anterior Cruciate Ligament.
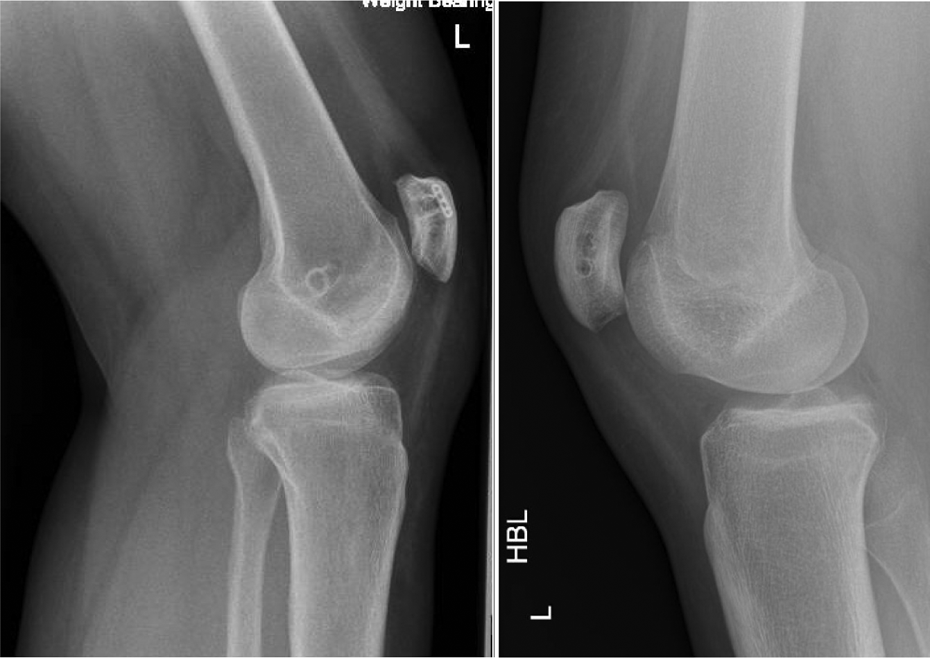
Lateral radiograph of MPFL reconstruction using (a) single tunnel (b) double tunnel patellar fixation. MPFL: medial patellofemoral ligament.
Patellar complications like anterior knee pain, metalwork irritation, patellar fractures and further surgery to address these issues were assessed as primary outcome of the study. Failure of the reconstruction and further instability were the secondary outcomes measured. Appropriate statistical tests were used to compare the data in both groups. Unpaired t-test and Mann–Whitney U-test were used for group comparison. Fisher’s exact test was used for ratio comparison. A p value < 0.05 was defined as a significant difference.
Results
Six patients complained of anterior knee pain related to the patella in group S and so did three patients in group D (p value 0.47). Three patients in the single tunnel group had irritation of the laterally positioned fixation device, and this required removal at 9, 20 and 60 months after the primary surgery (Figure 2). In all, a further of nine surgical interventions were needed in six patients in this group (Table 3). No further surgical interventions was necessary in any patient in group D (p value 0.02). None of the patients in either group was complicated by patellar fractures.

Irritating metalwork at lateral patellar border that necessitated removal in single tunnel patellar fixation.
Subsequent surgical procedures in group S.

LRR: lateral retinacular release; TTT: tibial tuberosity transfer; EB: endoButton fixation device; MPFL: medial patellofemoral ligament.
Symptomatic instability requiring revision surgery or realignment surgery was required in two patients in the group S and none in group D. The first was a 16-year-old young lady, who had patellofemoral chondroplasty performed prior to MPFL reconstruction. Her persistent instability warranted revision MPFL reconstruction using contralateral hamstring graft. However, she still had symptoms from patellofemoral joint due to chondral changes and further arthroscopic procedures were needed. A 20-year-old nursing student had failure of the reconstruction just over a year from surgery and underwent a TTT procedure elsewhere. Another 16-year-old lady had persistent pain but no complaints of instability after MPFL reconstruction. At arthroscopy, patellar chondral instability and lateral tilt required LRR. The MPFL reconstruction was intact with less than 25% lateral subluxation of the patella possible at 20° of knee flexion. The patellar fixation device on the lateral margin was also removed at the same time.
Discussion
In the past decade, MPFL reconstruction has gained popularity as the primary surgery for recurrent patellar instability. However, it is not a technique bereft of complications and failures. A systematic review of 25 studies of MPFL reconstruction reported a complication rate variable from 0% to 85.2%. 4 The overall cumulative complication rate reported was 26.1%, suggesting that caution needs to be exercised in surgical procedure, as many of these complications are due to technical error. 7 Although the most worrying complications are recurrent instability and patellar fractures, other frequently reported problems like knee stiffness, patellofemoral pain may necessitate return to operating theatre. 8
Persistent knee pain is frequently reported in these patients. In a large series of 240 MPFL reconstructions, Enderlein et al. reported that a third of their patients had some discomfort at the reconstruction region on medial side. 3 They found that 69% of patients had evidence of patellofemoral chondral injury at the index surgery. The degree of cartilage damage may be associated with post-operative chronic knee pain. 9 In our series, 12 of 58 (20%) knees had patellofemoral chondroplasty performed at the time of MPFL reconstruction. Nine patients in all (15%) had ongoing knee pain in the follow-up period. It is often difficult to ascertain how much of the pain is due to patellofemoral articular changes or to the prominent metalwork. The patients need to be counselled about this potential complication.
Patellar fixation device used in the single tunnel group required removal in three patients in our study (Figure 2). In a longitudinal study comparing EndoButton fixation versus graft anchor fixation in the patella, Astur et al. have reported similar rates of patellar discomfort with the EndoButton. 10 Their series had more complications in the single tunnel group compared to the double tunnel group, including one patella fracture. The study found that unlike the double tunnel group, patients in the single tunnel group had better functional outcomes at 2-year follow-up, compared to patients with 5-year follow-up.
A comparative study of single bundle versus double bundle MPFL reconstructions, using single and double patellar tunnel fixations, respectively, found better functional outcomes in the double bundle group, especially in the long term. 11 The study found that 26.9% of single bundle group was considered to have patellar instability, compared to 4.54% of the double bundle group. They argue that the anatomical double bundle reconstruction reproduces the anatomical structure, restores the biomechanical characteristics of the MPFL, and in the early rehabilitation period is much stronger than the single bundle in providing traction force against patellar displacement.
A devastating complication of the reconstruction is fracture of the patella. Parikh and Wall reported a series of five patellar fractures after MPFL reconstruction and noted three patterns: transverse fracture, superior pole/sleeve avulsion fracture, and medial rim avulsion fractures. 12 Surgical factors that needed attention include avoiding patellar tunnels that traverse the entire width of the patella, reduced tunnel size, maintaining an adequate bone bridge in dual tunnel fixation, avoiding devascularization of the superior pole of the patella, graft tendon choice in favour of gracilis tendon and avoiding over-tensioning of the graft. Fortunately no patellar fractures were reported in our series.
The drawbacks of this study include small numbers, short follow-up, and absence of objective scores. However, the study contributes valuable information into patellar complications that are more commonly associated with the single tunnel group than the dual tunnel group. This information, coupled with studies that report functional outcomes, shows favourable technique that surgeons can use with anatomical double tunnel MPFL reconstruction. Careful surgical technique is still critical for a successful outcome and to avoid complications.
Conclusion
Our study showed increasing problems with single tunnel patellar fixation, with more reoperation and failure rates compared to double tunnel fixation. The evidence supports the move towards anatomical double bundle MPFL reconstructions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.