
Abstract
Purpose:
Sensory disturbance around the surgical incision due to injury of the infrapatellar branch of the saphenous nerve can be seen in the anterior cruciate ligament reconstruction. In this research, we aimed to compare the incidence, extent of sensory loss, its clinical effect, and natural course caused by two different skin incisions used for hamstring graft harvest.
Methods:
Vertical incision for 36 patients and oblique incision for 42 patients used for graft harvest were included in this study. Sensory loss areas were documented at 6th week, 3rd month and 6th month. Pin prick examination is used to detect the change in sensation. Digital photographs of hypaesthesia were taken and analysed by computer for area detection. The length of incision and subjective complain of sensory loss were also noted.
Results:
At 6th month, 77% (28/36) of the vertical incisions were associated with persistent sensory loss when compared to the oblique incision (45%, 19/42). The measured area of hypaesthesia was significantly higher in vertical incision (42.4 ± 22.3 cm2) than that in oblique incision (9.3 ± 15.3 cm2) at 6th month. The area of hypaesthesia gradually shrunk in size from distal to proximal in direction. Also, subjective cutaneous anaesthesia was higher in vertical incision (15/36, 41%) than oblique incision (6/41, 14%) at 6th month.
Conclusion:
Oblique incision with less risk of nerve damage is better for graft harvesting. Area of hypaesthesia gradually reduces with time and even recover totally. As a possible complication, nerve injury and its benign prognosis should be explained to the patient before surgery.
Introduction
Anterior cruciate ligament (ACL) reconstruction is an effective and acceptable method for providing ligament stability. Hamstring tendons are an important source of autogenous graft for tendon reconstruction. Use of hamstring graft has gradually increased as the use of anterior one-third part of patella as graft source leads to anterior knee pain, kneeling pain or hypoesthesia. 1 –3 However, hamstring graft harvest has also some risks. Insertions of gracilis and semitendinosus tendons proceed quite close to saphenous nerve and its branches in medial of the knee. Use of minimally invasive techniques has increased for particularly meeting patient expectations. Therefore, the likelihood of a potential nerve injury during graft harvesting is related to the site and type of the surgical incision. 4,5
Saphenous nerve provides sensory innervation of the medial part of the knee, leg and ankle. 5 Saphenous nerve originates from the posterior part of the femoral nerve in proximal of the femur and enters adductor canal in medial of femoral artery. It is divided into two terminal branches as infrapatellar and sartorial after getting off the canal. Infrapatellar branch of the saphenous nerve (IBSN) proceeds to anterior and is divided into inferior and superior branches for innervation of the anteromedial part of the knee. An incision over pes anserine tendons causes risk for IBSN injury. It was reported that the nerve could be injured during blinded graft harvesting from a mini incision or it could be injured due to a blunt trauma at medial part of the knee during the pass of the tendon stripper. 6
A standard incision has not been described in the literature for semitendinosus and gracilis graft harvest. Brown described an oblique incision in parallel with the skin lines in superior of pes anserine. This parallel incision is considered to provide a better vision and lead to less scarring by facilitating skin retraction. 4 Marder et al. recommended a 4 cm of oblique incision at three fingers distal from joint level over the insertion of pes anserine. 7 In cadaver study of Pagnani et al., they reported that insertion site of hamstring tendons is at 1.9 cm distal and 2.25 cm medial of tibial tubercular apex and they recommended graft harvesting figure of four position of the knee for relaxing the saphenous nerve when passing gracilis tendon at posteromedial of the knee. 8 Vertical incision is considered to cause more scar tissue due to being vertical to skin lines and also increase nerve injury risk due to being vertical to IBSN. 9
Nerve injury is a potential complication during tendon harvest. Injuries are more common in superficial sensory nerves although serious complications like sciatic nerve injury have been described. 10 Spicer et al. reported sensory problems in anterior of the knee in 50% of the patients at the second year after graft harvest. 11 Mochizuki et al. described sensory loss in the ratio of 58% following arthroscopic ACL reconstruction. 12 Sanders et al. reported 32% injury in branches of saphenous nerve. Figueroa et al. reported this ratio as 77% in their electrophysiological study. 6,13 There are a limited number of clinical studies comparing different incisions although safe regions have been described in anatomic studies to avoid nerve injury. 6,12,14 There is not a single incision widely accepted for graft harvest. Therefore, in this study, we compared two different incisions, vertical and oblique incisions, used for hamstring tendon graft harvest with regard to infrapatellar branch injury and injury level, and it was aimed to report the clinical effect and natural course of the nerve injury.
Methods
Seventy-eight patients (74 males and 4 females) who underwent ACL reconstruction using hamstring autogenous graft between 2008 and 2012 were included in the study. The patients who underwent additional ligament reconstruction due to multiple ligament injury, meniscus repair, previous knee operation, who had a neurologic disease and who were under 20 years or above 50 years were excluded from the study. While a vertical incision was applied to 36 patients, an oblique incision was applied in 42 patients. Mean age of the patients was 31.1 years (31.6 for vertical incision and 30.4 for oblique incision); ACL reconstruction was applied to the left knee of 39 patients (Table 1). An informed consent was obtained from the patients prior to the study. The study was approved by the local ethics committee (registration number 2010/03).
Demographic values of the patients.
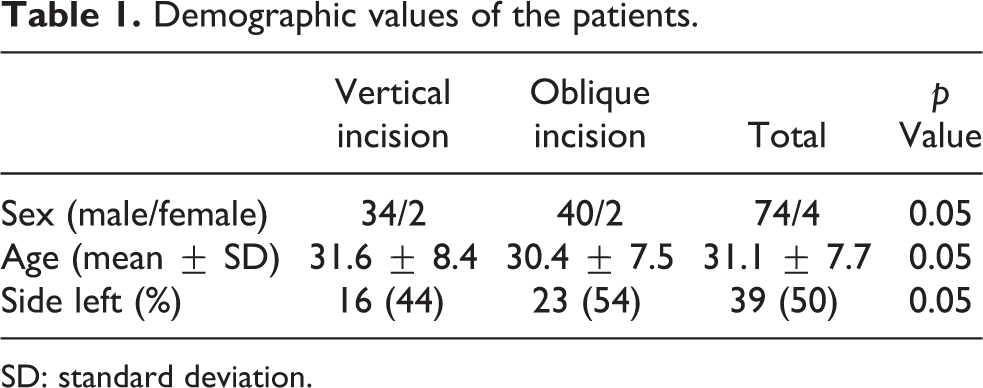
SD: standard deviation.
The patients who were considered to have ACL injury on preoperative clinical and radiological examination underwent reconstruction operation. First, knee was arthroscopically examined, and graft harvest procedure was done after exact diagnosis of ACL injury had been done. The preferred incision was marked after semitendinosus and gracilis tendons had been palpated at the medial of the knee. Vertical incision was done as 4 cm over the palpated tendons at 2 cm distal of the upper limit of central tuberositas tibia and at approximately 2 cm medial (Figure 1). The length of the incision was elongated when required. Oblique incision was done at the safe region described by Boon et al. 14 According to this definition, the incision was done with 50° of angle with the horizontal plane of which the central incision is 3.7 cm medial of tuberositas tibia and 5–5.5 cm distal of the joint line (Figure 2). Gracilis and semitendinosus tendons were palpated after the incision and the overlying sartorial fascia was opened along with the tendon. Two tendons were separated with a blunt dissection. The conjunction of semitendinosus tendon and gastrocnemius was cut before tendon harvest and the tendons were harvested with a close-ended tendon stripper.

A vertical incision patient.

An oblique incision patient.
ACL reconstruction was done with single-incision anatomic technique using standard arthroscopy devices and set. Tibial tunnel was done using the same graft incision with the guide adjusted to 55°. Anteromedial portal was used for femoral tunnel formation. The doubled fourfold hamstring tendon graft was fixed to femur with suspensory ring system. Bioabsorbable screw and staple fixation were used together for fixation of tibia. The same rehabilitation program was used for all patients. Isometric quadriceps exercises were started in the early postoperative period and the patients were given the minimum load that the patient could tolerate. Knee movements were started gradually until 90° of flexion and full extension could be reached at the 4th week. At 6th week, 120° of flexion was allowed and the required patients received rehabilitation.
Clinical sensory examination was done for all patients using a blunt needle at 6th week, 3rd month and 6th month. The points where sensory examination gave abnormal results were marked beginning from the proximal of the incision. These marked points were joined at the end of the examination (Figure 3). Afterwards, the photograph of the obtained area was taken. Area measurement was done (cm2) using Adobe Photoshop program (Adobe Photoshop CS6, 13.0.1) at digital media (Figure 4). So, clinical progression of sensory loss was followed up. Incision size was recorded in clinical follow-ups for all patients. A detailed functional examination was done and subjective scores were noted using International Knee Documentation Committee subjective knee assessment form at clinical follow-ups. 15

Paraesthesia area drawn after physical examination.

Measurement of paraesthesia area with computer assistance.
Two independent sample t-test was used for the comparison of incision length and demographic data of the patients. χ 2 independent test was used for the comparison of the categorical variables between groups. F analysis was used for the comparison of paraesthesia areas and a p value of <0.05 was accepted as statistically significant. Statistical analysis was done using SPSS (SPSS for Windows version 12) program. A priori statistical power analysis was performed with the percentage of the persistent sensory loss at 6th month as the primary outcome variable. We predicted that up to 75% of the patients operated with vertical incision would have sensory loss as Sabat and Kumar informed in their study. 16 Sample size calculations to obtain a power of 80% estimated that 36 patients would be needed in each group to detect a difference of 50% in the oblique incision group with an α level of 0.05 (two-sided), and a β level of 0.20.
Results
At 6th week, while 28 of 36 vertical incision patients (77%) still had paraesthesia, 19 of 42 oblique incision patients (45%) had paraesthesia and the difference was statistically significant (Table 2). Paraesthesia areas were seen to be larger in vertical incision group and the difference was statistically significant. Paraesthesia areas were seen to extend to distal beginning from the inferior half of the incision and to tuberositas tibia in lateral. Paraesthesia area was seen to decrease from distal to proximal in all patients. Saphenous nerve injury, neuralgia or reflex sympathetic dystrophy developed in none of the patients.
Outcomes of incision surgery by group.

When the patients were questioned with regard to complaints, complaint ratio was seen to be less than the measured ratio. However, the ratio of subjective complaints was significantly lower in oblique incision group compared to vertical incision group (Table 2). It was concluded that the patients did not recognize this problem or they neglected it. The patients who had subjective complaints were seen to have larger paraesthesia area. There was not a statistically significant difference between groups with regard to incision length and the other demographic data. A statistically significant difference was not found between groups with regard to International Knee Documentation Committee (IKDC) subjective knee assessment scores.
Discussion
Injury of IBSN is a potential complication following knee operations. 17,18 Although arthroscopic methods decrease incision size, the injury risk for saphenous nerve and branches is high due to proximity to surgical site. Mochida and Kikuchi reported 22.2% sensory disorder in IBSN following knee arthroscopy. 18 This risk increases particularly in the procedures like meniscus repair where incision and instrument use are required in posteromedial part of the knee. 19 The ratio of IBSN injury following ACL reconstruction may be related to autologous graft harvesting. Although the use of hamstring graft is recommended in order to avoid from the complications like anterior knee pain seen following patellar tendon harvest, saphenous nerve and IBSN injury may be encountered. 20 Some authors report that IBSN injury incidence is higher in patellar tendon autologous harvesting compared to hamstring graft harvesting. 7 Nerve injury was not reported when quadriceps tendon was used. 7
Saphenous nerve is the longest branch of femoral nerve and also it is the nerve branch, which proceeds longest in the body. 21 It proceeds along the posterior of sartorius muscle after passing the adductor canal. It goes on the surface of gracilis tendon in posteromedial of the joint line and gives patellar and sartorial branches thereafter. 20 This proximity explains the high risk for nerve injury during tendon harvest. 14 The nerve extends to distal together with the major saphenous vein in medial of tibia and is terminated with superficial peroneal nerve in dorsal of the second metatarsal. The nerve contains only sensory fibres and provides innervation of the medial of the knee, anterior of patella (infrapatellar branch), medial of the tibia crest, posteromedial of the cruris and medial of the foot. 22 Injury of the infrapatellar branch was reported to lead to sensory loss particularly in anteroinferior of patella, and thereby the problems like squatting and walking on the knees were seen. 23
The ratio of IBSN injury is suggested to be directly related to the incision during hamstring graft harvest. 16 Sgaglione et al. reported 37.5% infrapatellar paraesthesia in the patients undergoing primary ACL repair by strengthening with hamstring tendon; however, it should be considered that the ratio is also related to medial arthrotomy which is known to increase nerve injury. 24 Cory et al. in his ACL reconstruction patients, reported nerve lesion 6% in the hamstring autograft group and 31% in the patellar tendon group. 25 Spicer et al. reported the presence of sensory symptoms in anterior of the knee in the ratio of 50% and 86% of them were reported to be associated with IBSN in ACL reconstruction patients in whom hamstring tendon is used. 11 Kartus et al. reported 20% difficulty to walk on knees in the patients who were used hamstring tendon. 26 Soon et al. reported 4% saphenous nerve or IBSN sensory changes following ACL reconstruction using hamstring tendon. 27 The frequency of nerve injury was reported to be able to be related to the location, type and direction of the incision used for hamstring tendon harvest. The incision vertical to IBSN is considered to imperil the nerve. 9 This explains the nerve injury in vertical incision. Horizontal incision is a safer incision and IBSN injury is seen less. However, inferior branch of IBSN is under higher risk in horizontal incision. Incision is parallel to IBSN in oblique incision and the risk for nerve injury is less. 16 Tillet et al. reported no sensory symptoms in the patients in whom hamstring tendon harvesting was done with an oblique incision. 28 In this study, IBSN injury was seen less in oblique incision compared to vertical incision and mean paraesthesia surface area was measured smaller in the injured patients.
Tendon stripper was also reported to be able to lead to nerve injury during tendon harvesting. 8,18,29 However, tendon stripper–related nerve injury was reported to be rarer than incision-related problems. 5 Sanders et al. suggested that tendon stripper leads to injury in sartorial branch of saphenous nerve; however, incision-related nerve injury is related to IBSN. 6 It was reported that nerve injury could be reduced by some techniques performed during ACL reconstruction with arthroscopic surgery. Mochida and Kikuchi reported 30 mm medial of the medial border of the mid-patellar line and 10 mm medial line of patellar tendon as the safe area in cadaver study. 18 Tifford et al. recommended to make a horizontal incision parallel to the joint when the knee is at 90° of flexion from the safe area recommended by Mochida. 9 Kelly and Marcnicol recommended transillumination technique in order to determine saphenous nerve during arthroscopy due to its proximity to vena saphena magna. 30 In cadaver studies, oblique incision was reported to be far from IBSN compared to the other incisions and provided a safe area for tendon harvest. 12,28 Kodkani et al. reported that two incisions, one is at 1 cm distal of tuberositas tibia, another at flexion line of the knee, are safer in hamstring tendon harvest. 31 All authors accept the knee to be kept in flexion and thigh is recommended to be kept in external rotation during graft harvest. So, saphenous nerve goes to posterior and draws away from the surgical site. 8,20
Saphenous vein and IBSN injuries are complications which may still be seen following arthroscopic surgery. IBSN can still be seen although less even if an oblique incision is used for hamstring graft harvest as in our study. The patient should be informed preoperatively about that this condition may spontaneously resolve. Paraesthesia area gradually decreases postoperatively and even may disappear in follow-ups. Yasuda et al. reported that paraesthesia in graft area completely disappeared in 3 months in patients whose hamstring graft was harvested with an oblique incision from the undamaged side. 32 Paraesthesia in graft area gradually decreased and completely recovered in some patients. Complete recovery may be expected in higher ratios in long-term follow-ups. Recovery was reported to stop at the end of 1 year and paraesthesia became permanent. 21 Sabat and Kumar reported that postoperative paraesthesia is not so severe to influence the daily life of the patient and the patients do not think that this is a problem. 16 When the patients were questioned for subjective complaints, paraesthesia rate was lower than found in clinical examination also in our study.
Our study had limitations. The first limitation was the observer bias. Paraesthesia area examination was done only by one researcher. Because of our hard-working polyclinic conditions, another observer was not able to be eligible. Presence of the incision may also affect the patients’ response to physical examination and give clues about the study. The follow-up period was short, and longer follow-up period was required for detecting fate of the injury. Additional methods like electrophysiological studies would have been more useful for the analysis of the nerve injury level.
Injury to the IBSN can be seen during hamstring graft harvest. Oblique incision with less risk of nerve damage may be better for graft harvesting in ACL reconstruction. Area of hypaesthesia gradually reduces with time and even recover totally. Sensory loss does not impair normal daily activities in most of these patients. As a possible complication, nerve injury and its benign prognosis should be explained to the patient before surgery.
Conclusion
Injury to the IBSN can be seen during hamstring graft harvest. Oblique incision with less risk of nerve damage may be better for graft harvesting in ACL reconstruction. Area of hypaesthesia gradually reduces with time and even recover totally. Sensory loss does not impair normal daily activities in most of these patients. As a possible complication, nerve injury and its benign prognosis should be explained to the patient before surgery.
Footnotes
Author contribution
SS collected and analysed all the data and prepared the manuscript. SZ and BS designed the study and helped in writing the manuscript. All the authors recruited patients, performed the operations and followed up the patients.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.