
Abstract
Introduction:
It has been realized that for osteoarthritis (OA) knee with varus deformity, posterior cruciate ligament (PCL) release resulted in the increase of the flexion gap without significant effect on the extension gap. While the effect of release on gap angle is still obscure. On the other hand, gap distance and varus angle measured under different distraction forces suggest different patterns.
Objectives:
In the current study, mechanical gap balance in displacement and angular alternation of extension and flexion gaps will be evaluated, with PCL fully retained or resected under different distracting forces in varus knees.
Methods:
Fifty cases with medial OA undergoing posterior-stabilized (PS) total knee arthroplasty (TKA) were included in the study. PCL of all the cases were identified intact before resection. After distal femoral and proximal tibial cuts were initially performed and anterior cruciate ligament was excised, joint gap angle and distance in full extension and at 90° flexion were obtained by means of a tensioning device with 10, 20 and 30 inch-pounds (in-lbf) of distraction force. The gap angle and distance were measured three times at each step. After the excision of PCL, the same measurement was performed.
Results:
Both the distance and the varus angles of the knee gap enlarged accordingly with the augment of distraction forces at both extension and flexion with or without PCL resection. As to the gap distance, it remained the same after PCL resection at extension; while at flexion, the gap distance significantly (p < 0.001) enlarged – 1.2, 1.6 and 1.9 mm – under 10, 20 and 30 in-lbf, respectively, after PCL resection. As to the varus angles, it significantly (p < .050) decreased 0.6°, 0.3° and 0.4° at extension; while at flexion, the varus angles decreased 0° (not significant), 0.6° (p < 0.050) and 1.1° (p < 0.001) with 10, 20 and 30 in-lbf, respectively, after PCL resection.
Conclusion:
Our study indicated that the sacrifice of PCL will decrease the varus deformity at both extension and flexion, but with the exception under low distraction force at flexion. A proper distraction tension is of great importance in gap balancing during TKA. Sufficient attention of varus differences should be paid to the gap balance technique when choosing from different techniques, PCL-retained TKA or PCL-sacrificed TKA, as well as and an appropriate distract tension during measurement.
Introduction
The debate on prosthesis design that is preferable for total knee arthroplasty (TKA) is escalating, that is, cruciate-retaining (CR) design or posterior-substitute (PS) design; in other words, whether to retain the posterior cruciate ligament (PCL) or not. In a healthy knee, PCL not only plays a notable role in stability maintenance and kinematic motions but also has different types of mechanoreceptors for proprioception and kinesthesia, 1 which at present is hard to be replaced by any other devices. Besides that, the retention of PCL is resulted in increased stability and promoted femoral rollback, facilitating motions like walking and stair climbing postoperatively. 2 On the other hand, the sacrifice of PCL might contribute to the correction of varus or valgus deformity and the construction of an adaptive soft tissue balance. The proponents of each side are both valid enough with credible theoretical basis and experimentations and related clinical trials often conflict with each other.
The inconsistency of the results between CR TKA and PS TKA might be due to many reasons. Firstly, apart from the cam of the tibial insert, different designs of other parts of prosthesis will further complicate the issue. Secondly, different prostheses are sometimes performed by different orthopaedic surgeons, especially those with distinct surgical techniques, for example, the use of a spacer blocks is always neglected during CR TKA. 3 Furthermore, comparative study between CR TKA and PS TKA is hard to perform, since the pairing according to the degrees of knee deformity is hard to achieve, even for bilateral lower extremities. 4 All these factors mentioned above would increase statistic heterogeneity and bring about systemic biases. Therefore, a comparative experimental study with minimal biases is of great importance in investigating the mechanical performance of PCL in TKA.
In the current study, mechanical balance in displacement and angular alternation of extension and flexion gaps will be evaluated, with PCL fully retained or resected under different distracting forces in varus osteoarthritis (OA) knees. We hypothesized that PCL release would result in more remarkable increase in flexion gap, compared with extension gap. What is more, gap balances might vary under different distraction tensions in aspect of gap distance and varus angle. We intended to elaborate the mechanical role of PCL during TKA, providing comparative in vivo mechanical references for prosthesis type, choosing between PCL-retained TKA and PCL-sacrificed TKA.
Materials and methods
Patients
Fifty consecutive patients (40 women; 10 men) enrolled in this study underwent PS TKA in our institution due to OA knee with medial deformities. All the operations were performed by the same surgical team using the same surgical technique. The integrity of PCL was confirmed intraoperatively by the naked eye. Patients with suspicion of potential PCL deformity were excluded from the study. Written informed consent was obtained from the patients, and an approval was also obtained from the institutional research ethics committee.
Measurement device
A tensioning device Balancer (Stryker Orthopaedics, Mahwah, New Jersey, USA) was used (Figure 1) in this study to measure the gap distance as well as the varus angle at the same time. By spinning the handle, the ‘mouth’ of the device opens and measurements (distraction tension, gap distance and varus angle) are obtained with the help of the moving pointers on graduated surfaces.
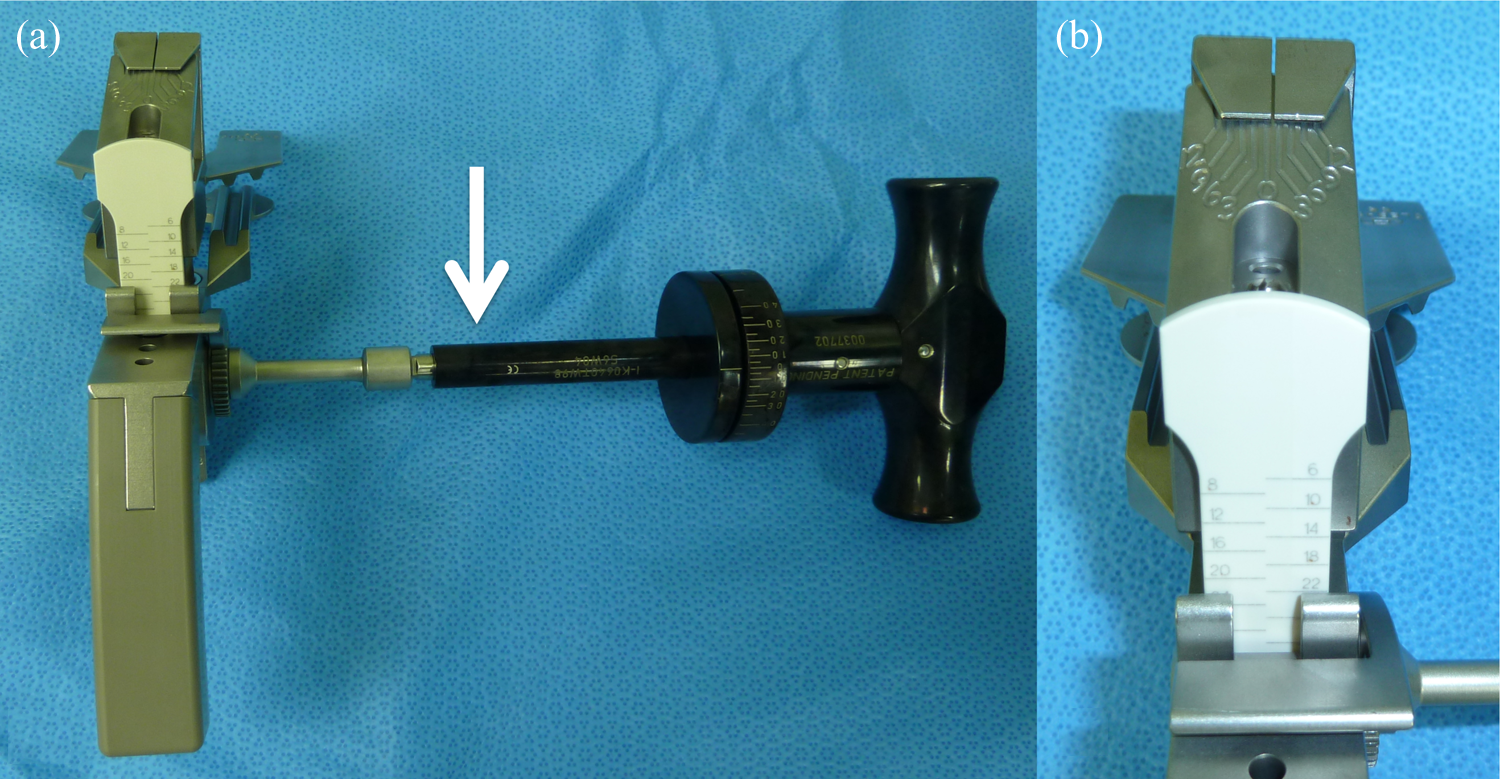
A tensioning device balancer (Stryker Orthopaedics). (a) White arrow indicates the handle. (b) Graduated surfaces on which measurements, such as angular alternation and distraction tension, would be indicated by the moving pointer.
Surgical procedure and measurement method
Femur was cut with the surface perpendicular to the mechanical axis of the femur, defined as the line connecting the femoral head and the intercondylar notch of the distal femur. Tibia was cut at the level 10 mm below the lateral surface centre perpendicular to the mechanical axis of tibia, defined as the line connecting the centre of the proximal tibia to the centre of the ankle using extramedullary technique devices. After the initial distal femoral and proximal tibial cuts were performed, with anterior cruciate ligament (ACL) excised according to standard surgical procedures, 10, 20 and 30 in-lbf were applied to distract the femoral–tibial gap using the balancer at 90° of flexion (Figure 2) and full extension. The gap distances and varus angles were measured three times at each steps. After the complete excision of PCL, the same measurement procedures were performed once again.

The application of the balancer in the measurement of gap distance and angular alternation using a specific distraction force with 90° of flexion.
Statistical analysis
IBM SPSS Statistic software 22.0 (IBM, Armonk, New York, USA) was used for the statistical analysis of the results. The average of the measurements repeated three times was calculated. The gap distances and angular alternation under different contraction forces at extension or flexion before and after PCL excision was compared using a paired Student’s t test. p-Value <0.05 was considered statistically significant.
Results
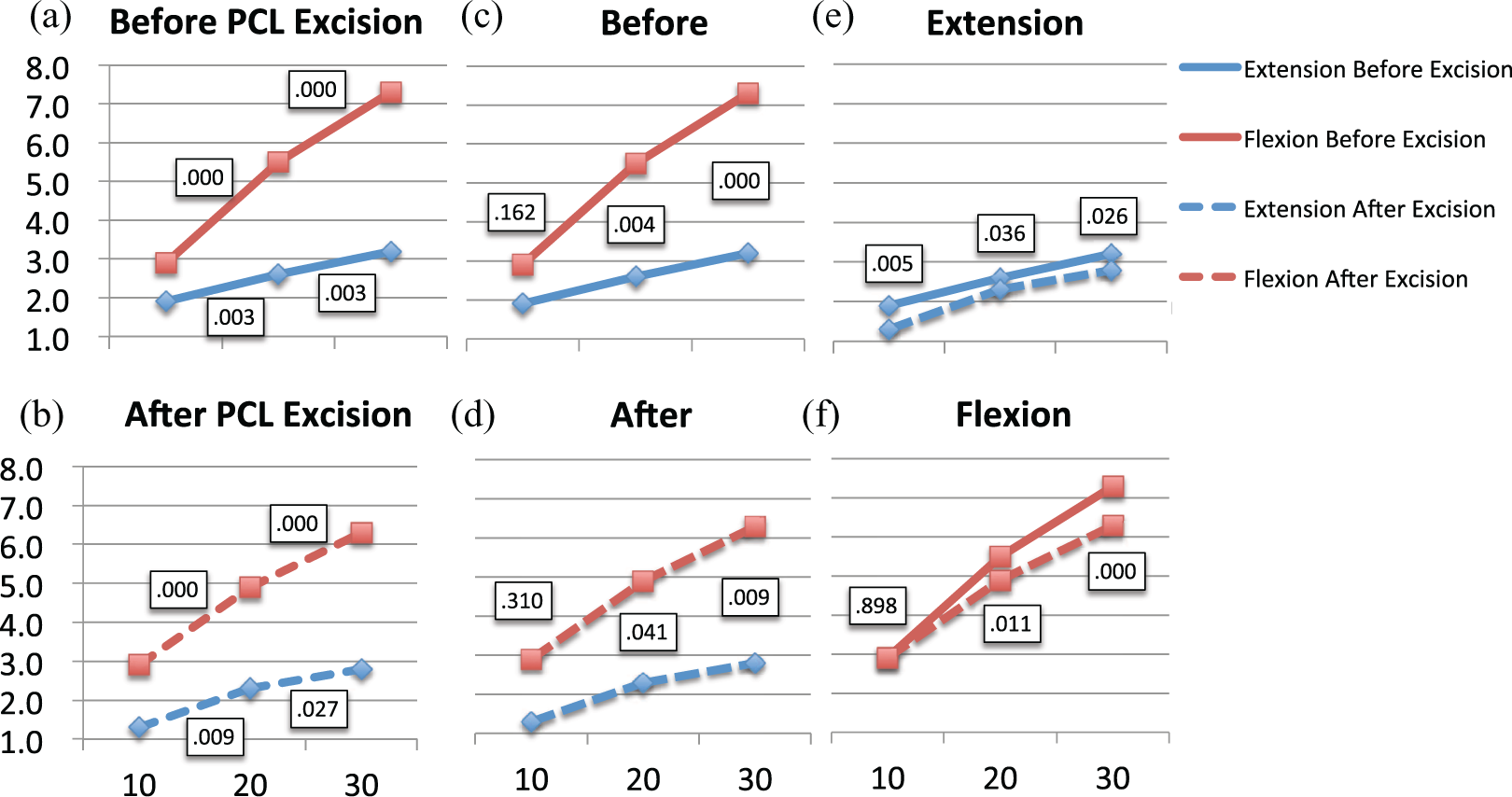
The average values of gap distance and varus angle with 10, 20 and 30 in-lbf are listed in Table 1. Both the gap distances and the varus angles of the knee gaps enlarged significantly and accordingly with the augment of distraction forces at both extension and flexion with or without PCL resection (Figures 3(a) and (b) and 4(a) and (b)).
The average values of gap distances and varus angles under different distraction forces in extension and flexion gaps.

PCL: posterior cruciate ligament.

The statistic differences in gap distances. (a) and (b) Between 10 and 20 in-lbf and 20 and 30 in-lbf of contraction forces before/after PCL excision; (c) and (d) between extension and after before/after PCL excision; (e) and (f) between before and after PCL excision at extension/flexion. in-lbf: inch-pounds; PCL: posterior cruciate ligament.
The statistic differences of varus angle. (a) and (b) Between 10 and 20 in-lbf or 20 and 30 in-lbf of contraction forces before/after PCL excision; (c) and (d) between extension and after before/after PCL excision; (e) and (f) between before and after PCL excision at extension/flexion. in-lbf: inch-pounds; PCL: posterior cruciate ligament.
Gap distances before and after the sacrifice of PCL
The gap distances measured were significantly larger at extension than at flexion both before and after the excision of PCL (Table 1, Figure 3(c) and (d)). Differences in gap distance between extension gap and flexion gap were 7.8 , 8.6 and 8.3 mm before PCL sacrifice and were 7.3 , 6.9 and 6.4 mm after PCL sacrifice with 10, 20 and 30 in-lbf. During extension, the gap distances remained the same after the resection of the PCL, with no significant differences (p = 0.051, 0.194 or 0.612, respectively); while in flexion, the gap distances enlarged – 1.2 , 1.6 and 1.9 mm – showing significant (p = 0.000, 0.000 and 0.000, respectively) difference for each distracting force (Table 1, Figure 3(e) and (f)).
Angle alternation before and after the sacrifice of PCL
The varus angles measured were also significantly larger at flexion than at extension both before and after the excision of PCL (Table 1, Figure 4(c) and (d)). Differences in varus angle between extension gap and flexion gap were −1.0°, −2.9° and −4.1° before PCL sacrifice and were −1.6°, −2.6° and −3.5° after PCL sacrifice with 10, 20 and 30 in-lbf. At extension, the varus angles decreased 0.5°, 0.3° and 0.3° significantly (p = 0.005, 0.036 and 0.026, respectively); while in flexion, the varus angles decreased 0.6° and 1.1° with 20 and 30 in-lbf with significance (p = 0.011 and 0.000) and yet remained the same with 10 in-lbf (Figure 4E and F).
Discussion
The most important finding of the present study is that the sacrifice of PCL will decrease the varus deformity at both extension and flexion, with the exception of under low distraction force (10 in-lbf) at flexion. By searching the PubMed database with the strategy of ‘TKA PCL gap flexion extension’, we finally located eight articles 5 –12 concerning the differences in the gap balance after PCL resection after viewing the titles and the reference lists of related articles (Table 2). Among these studies, the results of Kadoya et al. 7 and Park et al. 10 suggested that the distance of medial gap increased more compared with the lateral gap, in other words, decreasing the degrees of the varus deformity, which are consistent to our work with high distract force (20 and 30 in-lbf). Conversely, Baldini et al.’s 8 research agrees with the present study that under low distraction force the degree of varus deformity remains the same. These facts suggested that different distracting tension applied to the joint gap will result in different measurement of the varus angles, which might eventually influence the surgical strategy during TKA. When changing from CR-TKA (PCL retained) to CS-TKA or PS-TKA (PCL sacrifice), extra attention should be paid to the gap balance technique during TKA and an appropriate distract tension.
Medial and lateral gap increase at extension and flexion after sacrifice of PCL in previous studies.
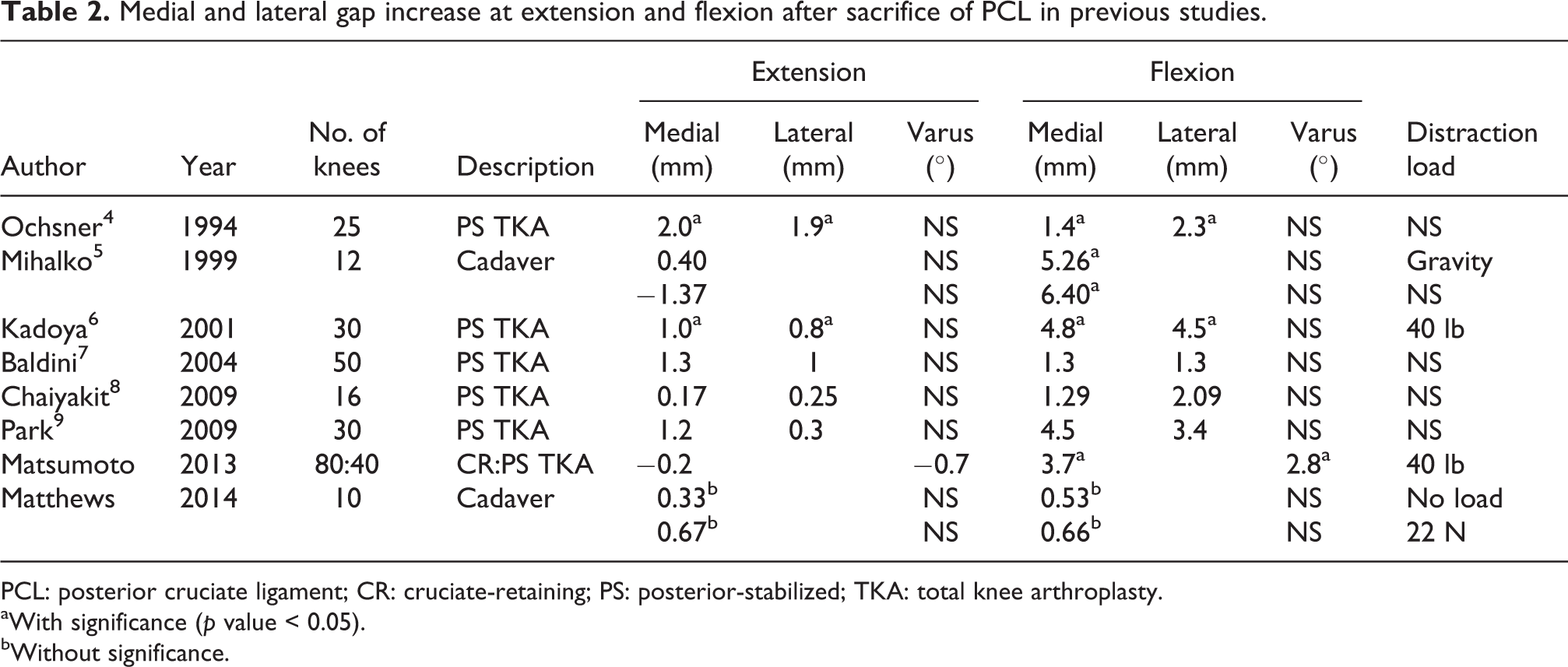
PCL: posterior cruciate ligament; CR: cruciate-retaining; PS: posterior-stabilized; TKA: total knee arthroplasty.
aWith significance (p value < 0.05).
bWithout significance.
Besides that, PCL sacrifice will generally result in a larger gap space at flexion and the same extension gap in both the present study and the previous studies. In the present study, the gap distance at flexion increased significantly after the resection of PCL by 1.2 to 1.9 mm with distracting tension of 10 to 30 in-lbf and yet remained the same at extension. Furthermore, the gap distance trended to increase accordingly to the distracting tension at both extension and flexion before and after PCL sacrifice, which might explain the variety of results of the previous studies, especially the studies of Mihalko and Krackow 6 and Matthew et al. 12 who used different distracting forces. This fact also indicated that the evaluation of the joint gap distance might be inaccurate without an appropriate consideration of the expansion force.
As to the choice of surgical technique between CR TKA and PS TKA, a recent meta-analysis collecting 14 Randomized Clinical Trials (RCTs) concluded that there is no clinical-relevant difference between CR TKA and PS TKA in terms of radiological and clinical outcomes, while PS TKA is superior to CR TKA with respect to range of motion (ROM), 13 which might be the result of increased flexion gap and decreased varus angle after PCL sacrifice. One more reason that CR TKA is not preferred is that most of the PCL insertion is likely to be sacrificed fully or partially during preparation of the tibial plateau, 14,15 which will potentially influence the clinical outcome. Although many landmarks, such as fibula head, 16 had been proposed to improve the procedure, priority should always be given to a more insured surgical technique. The present study might play a role in providing the basic experimental evidence, supporting the results of a better outcome after the resection of PCL.
CS TKA is claimed to have good good anterior–posterior constrain via a highly conforming anterior buildup even after the excision of PCL. However, it sometimes could not restore the posterior stability with PCL sacrifice. 17 One meta-analysis that included 20 RCTs (up to 19 May 2014) was published, 18 comparing retention (CR) or sacrifice (CS) of the PCL in TKA. Although a slight favour of PCL sacrifice (CR) on post-operative flexion angle and KSS functional score was presented, there was no significant results as to other outcomes measured, concluding no clinically relevant differences between retention (CR) and sacrifice (CS) of the PCL in TKA. However, just as the author claimed that the current meta-analysis was based on moderate to low quality studies, high-quality evidence is still needed for further recommendation. At the same time, another 10-year observational study that included 414 knees suggests conflicting results that CS TKA performed better in post-operative clinical scores, such as Knee Society Clinical Rating System (KSCRS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Short Form 12-item (SF-12), and knee ROM compared to CR.19 However, the comparison between CR TKA and CS TKA has not drawn a conclusion yet.
Conclusion
The present study is the first comparative study adopting varus degree alternation instead of medial and lateral gap difference after the resection of PCL under different distraction tensions in TKA patients. Our study indicated that the sacrifice of PCL will decrease the varus deformity at both extension and flexion, but with the exception of under low distraction force at flexion. A proper distraction tension is of great importance in gap balancing during TKA. Sufficient attention of varus differences should be paid to the gap balance technique when choosing from different techniques, PCL-retained TKA or PCL-sacrificed TKA, as well as and an appropriate distract tension during measurement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.