
Abstract
Background:
Metatarsus adductus (MA) is a common pediatric foot deformity. Current recommendations suggest observation until 4–6 months, then casting if the deformity persists. Based on our review of the literatures, no randomized controlled trial has been conducted to study the effectiveness of parental stretching in the correction of MA in newborn.
Material and methods:
Ninety-four newborn feet that were diagnosed as MA by clinical examination were enrolled. Feet were randomized into two groups: observation group and stretching group. Outcome measurements were performed to compare success rate between groups.
Results:
According to Pearson’s χ 2 test, there were no statistically significant differences between groups with regard to the overall success of the parental stretching program (p = 0.191). There was also no significant difference between groups for mild degree or moderate-to-severe degree (p = 0.134, p = 0.274, respectively). A more rapid success rate was observed in the stretching group at the first month follow-up, but rate of improvement then decreased. The stretching group tended to have a lower success rate compared to the observation group in moderate-to-severe feet, but the difference was not statistically significant.
Conclusions:
Parental stretching program found no benefit over observation group in this study. Parental stretching program should not be applied for newborn babies with moderate-to-severe MA as the result from the study appeared to have lower success rate compared to observation group. Observe until 4–6 months, then corrective casting for the persisting deformity is recommended.
Background
Metatarsus adductus (MA) is a congenital deformity of unknown etiology with an incidence of 1:1000 live births. 1 –3,9 MA is a deformity within the Lisfranc joint of the foot that causes contracture of the soft tissues around the Lisfranc joint, convex lateral border of the foot, and development of a prominent styloid process. MA causes a normally reversible deformity of the foot, whereby the forefoot becomes adducted relative to the normal position of the hindfoot, and MA is solely a forefoot deformity. 2 –6 Residual or uncorrected deformity may cause abnormal foot posture that may affect normal gait later in life. One author described the physiological changes associated with MA and proposed that long-term MA can force the metatarsals to adopt a varus position that could evolve into metatarsus primus varus deformities. 7
Another MA study reported that resulting osseous change appeared as a hooked or concave position development that was presumed to increase stability and articulation within the tarsal bones. 8 Other deformities discussed in the literature that are thought to be associated with MA include bunions, hammertoes, medial tibial torsion, and intoeing. 5,12 There are, however, no long-term studies that have confirmed these suspected associations. Most cases of MA can be treated with observation and simple passive stretching, 1 –5,10 but approximately 11–14% of cases are persistent and require treatment. 2,16 Current standard treatment recommendations suggest observation after diagnosis until the age of 4–6 months, after which serial casting for deformity correction is advised. 2
There are several outcome studies in MA, with most patients presenting with benign and self-limiting MA. 1,4 –6,11,13 –16 A recent meta-analysis emphasized the importance of an accurate initial severity assessment in MA for purposes of identifying appropriate treatment strategy. In mild MA, observation is recommended. More severe MA should be treated with casting or bracing. This study also emphasizes the lack of prospective, randomized clinical trials. 16 We hypothesized that the clinical outcomes of parental stretching in newborn MA feet would be comparable between the two groups of infants with mild MA, but that outcomes would be better in moderate-to-severe MA, as compared to the observation group.
Data and recommendations in the literature regarding the treatment of MA are contradictory and inconclusive. Few prospective studies have investigated the benefits of foot manipulation in newborns with MA feet, with inconsistent results reported from the studies that have been conducted. 9,16 Our review of the literature revealed a lack of high-level data regarding the nonsurgical treatment of MA. Based on our review of the literature, no randomized studies in the treatment of MA have been conducted. Accordingly, the objective of this randomized controlled trial was to compare the effectiveness of treatment by parental stretching versus observation in newborn MA feet.
Methods
The study protocol was approved by ethics committee. Informed consent was obtained from parents. Data was collected from newborns diagnosed with MA in our hospital. We enrolled 94 newborn feet diagnosed as MA, then randomized into two groups. Parental stretching program was educated in the first group and observation in the other (Figures 1 and 2). MA was diagnosed using Blake’s heel bisector method. The flexibility was differentiated into “flexible,” “semiflexible,” and “rigid.” The flexibility was determined by holding the heel in neutral and abducting the forefoot away from the midline of the foot. Flexible MA was reported when the deformity was correctable past the midline of the foot (abduction of the forefoot). If the forefoot was corrected to the midline of the foot, the MA was considered semiflexible and if not, it was reported as rigid MA. 3,4,15
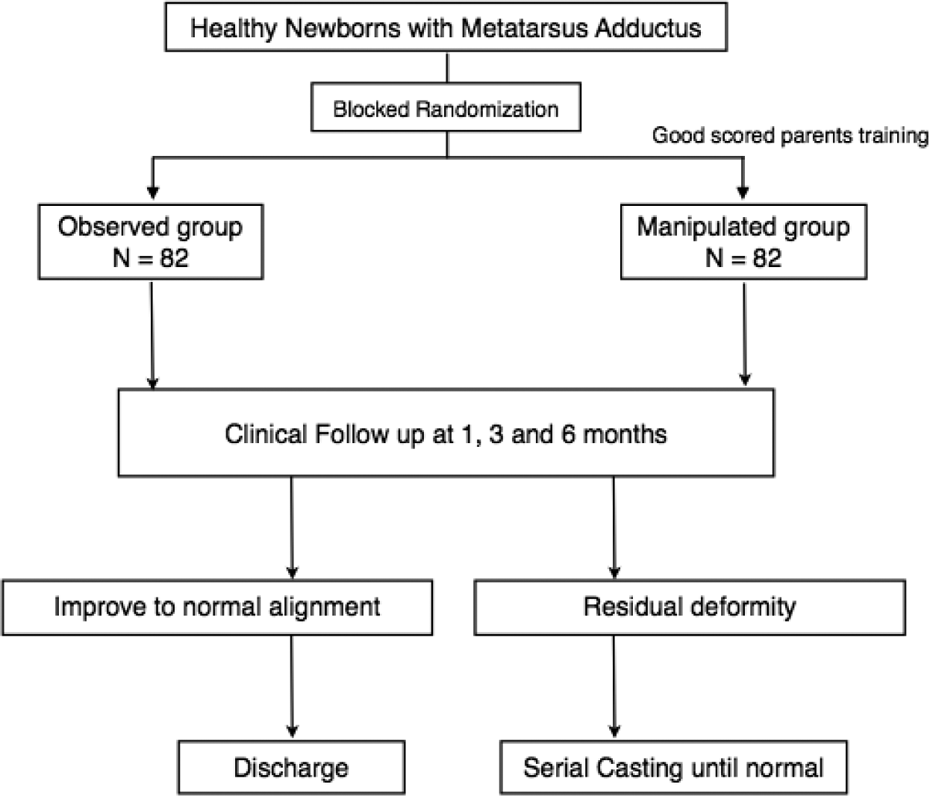
A consort flow diagram for enrollment and analysis in protocol.

A consort flow diagram for enrollment and analysis in protocol.
After informed about the diagnosis to the parents, all demographic data of the patients were collected. Severity and flexibility were recorded. The newborns were randomized to either parental stretching program or observation group using block randomization. An appointment was made in observation group for clinical examination at 1 month, 3 months, and 6 months. If the deformity persisted at the last follow-up, serial casting for deformity correction will be performed.
Foot manipulation technique was demonstrated to parents of stretching program group by using information sheet and video presentation (VDO) demonstration, illustrated by author or coauthor (Figures 3 and 4). Parents were trained to achieve satisfactory score of at least 8 from total score of 10 by our criteria. An appointment for clinical examination was done at 1 month, 3 months, and 6 months. Parents were instructed to stretching 10 times/day. They were supplied with printed instructions included the timetable for stretching program. All patients were personally cared for by the author. The result was determined clinically at 6 months based on the appearance of the foot by Bleck grading method. If the line pass second toe, then we consider for normal alignment. The Heel bisector method is a subjective measurement based on the observer’s interpretation of the shape of the foot and where a line would bisect its oval appearance. Attempt to minimize error was conducted by having a single observer, blinded to the patient name and treatment status, to do all measurements.

Hindfoot holding position.

Foot manipulation technique.
Data collection included sex, age at study entry, treatment types, numbers of clinic visits, and lengths of follow-up. Finally, parents completed an exit interview reporting feelings about problems associated with their child’s treatment protocol.
Foot manipulation technique
Stretching group newborns were positioned in the supine position. Parents were instructed on how to abduct the forefoot while controlling the position of the hindfoot. The calcaneus was held stationary and the forefoot was bent by simply abduction at the level of the first metatarsal head, with counterpressure applied over the cuboid without forcefully pronating the foot. Care was advised to avoid creating valgus moments on the heel when applying abduction force on the forefoot. Passive abduction was applied to the forefoot until the first toe passed the heel bisector line. This position was then maintained for 10 seconds before the start of the next manipulation (Figures 3 and 4). Parents were instructed to perform this manipulation on both feet at least 10 times per day. A treatment record form was provided to help parents to keep track of how many manipulation treatments had been performed.
Statistical analysis
Statistical analysis was performed using SPSS software (IBM version 20), and p values < 0.05 were considered significant. General demographic data of patients (such as age, sex, head circumference, body length, affected feet side), parents, and birth history were collected and analyzed. Efficacy of treatment was determined by success rate at the time of last follow-up. Results of each group were compared using the Pearson’s χ 2 or Fisher exact test for categorical variables and the student t-test for continuous variables. Kaplan–Meier analysis was used to compare time to success among the group (Figure 5)

The graph shows a Kaplan–Meier survival curve for stretching group and observation group.
Results
The total number of 91 patients was allocated and randomized by using block randomization. Thirty-seven patients were excluded because of loss to follow-up. The remaining 54 patients with 94 affected feet (left side 6 feet, right side 8 feet, both sides 80 feet) were analyzed (Figure 2). The demographic data of the patients was shown in Table 1. Among the affected 94 feet, there were differences in disease severity according to Blake heel bisector grading, 55 feet were classified in mild form, 36 feet were moderate, and 3 feet were severe by clinical examination. At the last follow-up, 28/40 feet from observation group became normal and 40/54 feet in stretching group became normal. Success rate of mild MA was 62.5% in observation group and 80.6% in stretching group with no statistical significance (p = 0.134). Success rate of moderate-to-severe MA was 81.5% in observation group and 65.2% in stretching group, though this difference was not significant (p = 0.274; Table 2).
Demographic data of the patients.

aMean values.
The comparison of success rate between the groups at the end of study.
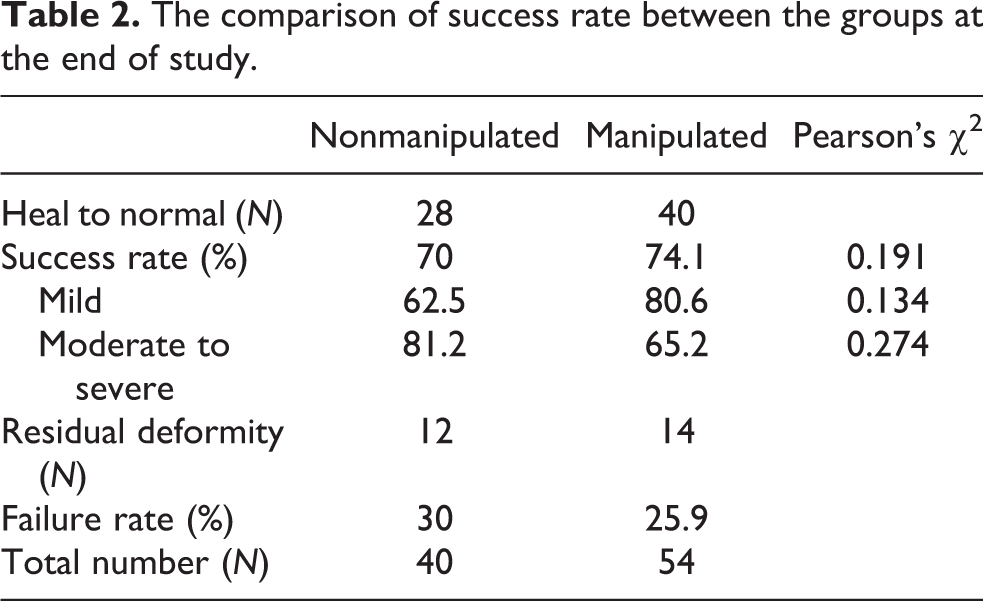
Kaplan–Meier analysis was used to compare time to success between the groups (Figure 5). The overall success rate in observation group was 15% at 1 month, 55% at 3 months, and 70% at 6 months whereas the success rate in manipulation group was 35% at 1 month, 67% at 3 months, and 74% at 6 months. The success rate of mild deformities in stretching group was higher than observation group (80.6% vs. 62.5%, Pearson’s χ 2 0.134). The success rate of stretching group was lower in moderate-to-severe deformities (65.2% vs. 81.2%, Pearson’s χ 2 0.274). Our hypothesis, “stretching program would be higher success rate in moderate-to-severe metatarsus adductus,” was found not true based on the outcome that it has lower success rate. The data showed that although there was a difference in success rate between the two groups, it was not a significant difference between these two groups.
Discussion
MA has been increasingly observed among clinicians. Some MA deformities improve spontaneously, whereas others worsen. A 1985 study found that intoeing gait developed in patients with uncorrected MA. 12 Older children and adults with uncorrected MA rarely complain of pain and occasionally have metatarsus primus varus deformities and bunions. Although MA is not a disabling deformity in adults, correction of this disorder is advisable in infants. 2 Many physicians believe that MA-related deformities will self-correct over time without treatment, 16 whereas other physicians advocate passive stretching of the foot by the parents. 3 Bohne reported that flexible MA responded well to shoe modification, adjusted sleeping position, and passive stretching of the forefoot. 6 However, there was no control group and levels of flexibility were not established in that study. It is, therefore, possible that the results of that study may have been influenced by self-resolving cases within those receiving treatment. Two authors proposed that incorrectly performed stretching of the foot in MA, whether conducted by parents or health professionals, can cause the heel to sit in a valgus position. 2,3 This posture change may lead to the development of flat feet (pes planus) and/or skewfoot. Although there is no research data to support this statement, some authors in cohort studies advocate instruction of stretching technique. 2,7,9 No study has been conducted that proves the impact of stretching in MA. The absence of a control group decreased the strength of the author’s argument. Given the small number of studies that have been conducted in the efficacy of stretching in pediatric MA, the present study was undertaken to prospectively randomize and compare the results of stretching in pediatric MA with an observation-only study group.
Ponseti and Becker do not advocate stretching by parents, because they found that stretching in patients with complex deformities are usually poorly performed by family members. 2 In the present study, mild deformity MA usually yielded faster recovery with manipulation by family. Stretching by well-trained parents has potential effect in cases of mild deformity MA. From a report by Ponseti and Becker, moderate-to-severe MA deformity appeared to worsen in the stretching group, as compared to the observation group. 2 Although the results of this study showed no significant difference in overall success rate between groups, it was shown that manipulation seemed to worsen in moderate-to-severe cases of MA in newborns. Therefore, we recommended observation only in MA and advised parents to avoid positions that may prolong or worsen MA-related deformity. Treatment of more severe forms of MA with more complex deformity must be based on a clear understanding of normal foot kinetics and their alterations in MA.
Parents should be mindful of sitting and sleeping postures that force the foot into a prolonged adduction position, because this could prolong the deformity. 11 Children often sleep in a prone position, with some babies having their buttocks elevated, the hips and knees in complete flexion, and the feet often adducted and tucked in underneath the buttocks. Because these sleeping positions tend to worsen MA deformity and prolong its presence, we routinely advise parents to observe for and attempt to correct these habits.
The primary limitation of this study centers on the use of clinical examination for patient evaluation. Clinical examination is highly subjective and radiologic evaluation would have provided potentially more accurate and objective assessment. However, radiographic assessment would have exposed our patients to unnecessary radiation and would not have visualized noncalcified bone in newborns.
Conclusions
Parental stretching in infants with mild degree of MA yielded faster recovery compared to the observation-only/nonstretching group. Although up to an 80% success rate was observed in the stretching group, the difference in overall success rates between groups was not statistically significant. In moderate-to-severe deformity, our results showed a lower success rate in the stretching group; but, again, the difference between groups was not significant. In conclusion, the authors recommend all MA feet should be observed for 6 months, then casting if deformity persisted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.