
Abstract
Introduction:
Percutaneous fixation of intra-articular calcaneal fractures is traditionally assisted only by intraoperative fluoroscopy. Previous studies have demonstrated that the additional use of subtalar arthroscopy in anatomical reduction of the posterior calcaneal facet of the subtalar joint for less complex calcaneal fractures yielded positive results up to 2-year follow-up. This study aims to investigate long-term outcomes of these patients using similar evaluation parameters. We hypothesized that this novel technique with dual-imaging can provide sustainable, long-term benefits with good functional outcomes and significant restoration of the Bohler’s angle.
Methods:
We performed a retrospective study of 15 Sanders II, AO-OTA 83-C2 intra-articular calcaneal fractures in 14 patients who underwent subtalar arthroscopy and fluoroscopy guided percutaneous fracture fixation with a minimum follow-up of 5 years. Outcome measures were assessed using the ankle and hindfoot NPRS, AOFAS ankle–hindfoot score, and SF-36 Physical Function subscale preoperatively and at 3 months, 6 months, 1 year, 2 years and 5–8 years postoperatively. The Bohler’s angle was measured preoperatively, immediately postoperatively and at 5–8 years postoperatively.
Results:
We report excellent functional outcomes in all scores as well as continued improvements in the majority of patients across all time points with minimal subsidence of the corrected Bohler’s angle over our study time frame.
Conclusion:
Subtalar arthroscopy with intraoperative fluoroscopy in anatomical reduction of the posterior calcaneal facet of the subtalar joint is most useful in Sanders type II, AO-OTA 83-C2 fractures with excellent functional outcomes and good preservation of the corrected Bohler’s angle on long-term follow-up.
Introduction
Calcaneal fractures are often the result of traumatic axial loading, such as falling from heights. Three-quarters of these fractures are intra-articular and are associated with less favourable outcomes, especially in the presence of risk factors for wound complications, for example, diabetes, smoking, peripheral vascular disease and open fractures. 1
Anatomic reduction and restoration of joint congruity in the posterior subtalar joint are thought to be the most important indicators of prognosis. 2 –6 Large contact shifts can result from incongruity as low as 1–2 mm leading to alterations in the load bearing mechanics of the joint and predisposing to subtalar osteoarthritis. Pain and the consequent compromise in functional outcomes may ultimately necessitate secondary subtalar fusion. Although open reduction internal fixation with the traditional L-shaped lateral incision offer excellent fracture visualization and facilitates direct reduction in some areas, this is not without limitations and significant drawbacks in the management of calcaneal fractures. Attendant soft-tissue complications such as wound edge necrosis with an extended lateral incision have been shown to occur up to 11% of cases and infection rates up to 7%. 7
Recent advances in minimally invasive surgical techniques, such as limited-incision sinus tarsi ORIF, percutaneous fixation and arthroscopic-assisted fracture reduction, have shown promising outcomes in patients with soft-tissue compromise, multiple comorbidities and displaced intra-articular fractures with minimal comminution. 8 There is, however, limited data on the long-term benefits of these procedures.
In our earlier prospective study of 22 consecutive patients with Sanders II, AO-OTA 83-C2 intra-articular calcaneal fractures who underwent fixation with intraoperative fluoroscopy and subtalar arthroscopy in 2010, we demonstrated significant correction of Bohler’s tuberosity joint angle with minimal subsidence at 2 years and significant improvements in mean ankle and hindfoot Visual Analog Scale (VAS) pain score, American Orthopedic Foot and Ankle Society (AOFAS) ankle–hindfoot score and Short Form-36 (SF-36) Physical Function scores up to 2 years. 9 The objective of this retrospective study is to evaluate long-term outcomes of the use of dual-modality imaging using similar evaluation parameters.
Materials and methods
Subtalar arthroscopic and fluoroscopic guided percutaneous fixation of 15 Sanders II intra-articular calcaneal fractures were performed in 14 patients (13 male, 1 female) between April 2007 and June 2010. The mean patient age was 51.4 years (range 39.3–66.9 years). Mean duration of follow-up was 79.2 months (range 64–100 months).
All our patients had Sanders type II, AO-OTA 83-C2 fractures. This is due to the selection criteria of our technique. We have previously excluded Sanders type III and IV, AO-OTA 83-C3 and C4 calcaneal fractures on the premise that these fracture patterns were more appropriately addressed with open reduction internal fixation.
Outcome measures
Similar evaluation parameters for residual pain and function were used in the assessment of long-term outcomes of these patients as our previous study. These include: (1) the ankle and hindfoot NPRS, (2) the SF-36 Physical Function (SFPF) subscale and (3) the AOFAS ankle–hindfoot score.
The NPRS pain score assesses pain from a scale of 0 (no pain) to 10 (worst possible pain). The SFPF subscale assesses physical function on a scale of 0 (extremely poor function) to 100 (excellent function). The AOFAS ankle–hindfoot score assesses pain (40 points), function (50 points) and alignment (10 points). A total score of 0 indicates a poor result whereas a score of 100 indicates an excellent result.
Assessment was performed and compared against previous scores documented at the following time points: before surgery, 3 months, 6 months, 1 year and 2 years postoperatively. Preoperative assessment was performed at the bedside, whereas postoperative evaluation was conducted at a dedicated Orthopaedic Diagnostic Center by a blinded physical therapist at the appropriate time points.
Radiographic analysis was performed using plain radiographs with lateral, Harris-Beath axial and Broden’s views. Bohler’s tuberosity joint angle was measured thrice by two blinded observers on lateral radiographs using software tools (Image management System Version 5.1) to two decimal places and averaged. The final figure was then corrected to one decimal place for reporting purposes. These were measured on radiographs preoperatively, immediately postoperatively and on long-term follow-up, as shown in Figure 1.

Examples of (a) preoperative; (b) immediate postoperative; and (c) long-term follow-up (5–8 years postoperative) lateral radiographs.
Statistical analysis
The data was compiled and analyzed using SPSS version 21 (SPSS Inc., Chicago, Illinois, USA). Continuous data was expressed as mean values and standard deviations. Analysis of variance with Bonferroni adjustment was used in the statistical analysis of both Bohler’s tuberosity joint angle and subjective outcome measures (NPRS, AOFAS and SF-36) across different time points. A significant result was taken as p < 0.05.
Results
There was significant correction of Bohler’s tuberosity joint angle from 3.5 ± 7.5° preoperatively to 18.7 ± 10.1° postoperatively (p < 0.001), with mean correction of 13.8 ± 9.8°. The Bohler’s tuberosity joint angle on long-term follow-up (mean 79.2 months, range 64–100 months) was 17.6 ± 10.2°. Compared to postoperative values, there is a subsidence of 1.2 ± 1.6° which was not statistically significant (p > 0.999). The Bohler’s tuberosity joint angles at the various time points are as shown in Figure 2.

Bohler’s angle.
Comparison between patient-reported outcome measures at the different time points can be found in Figure 3. Compared with preoperative values, there was significant improvement in the 3-month NPRS (from 8.6 ± 2.3 to 4.0 ± 3.1), AOFAS (from 11.2 ± 17.9 to 54.5 ± 23.4) and SFPF score (from 11.7 ± 22.2 to 50.0 ± 27.8). At 6 months, the NPRS, AOFAS and SFPF scores were 2.8 ± 3.0, 68.6 ± 26.4 and 68.0 ± 26.2, respectively. At 1 year, the NPRS, AOFAS and SFPF scores were 1.9 ± 2.9, 79.9 ± 25.0 and 80.0 ± 20.3, respectively. At 2 years, the NPRS, AOFAS and SFPF scores were 1.2 ± 1.8, 86.8 ± 11.9 and 91.8 ± 8.9, respectively. On long-term follow-up (mean 79.2 months, range 64–100 months), the NPRS, AOFAS and SFPF scores were 0.9 ± 1.8, 90.3 ± 12.2 and 92.7 ± 7.3, respectively. These indices showed continued improvement over the entire follow-up period.

Subjective outcome measures.
Of the 14 patients, 12 had unilateral calcaneal fractures and 2 had bilateral calcaneal fractures (Table 1). Fifteen of the 16 calcaneal fractures were amenable to percutaneous fixation guided by our dual-modality imaging.
Summary of patients’ demographics, injuries sustained and follow-up time frame.
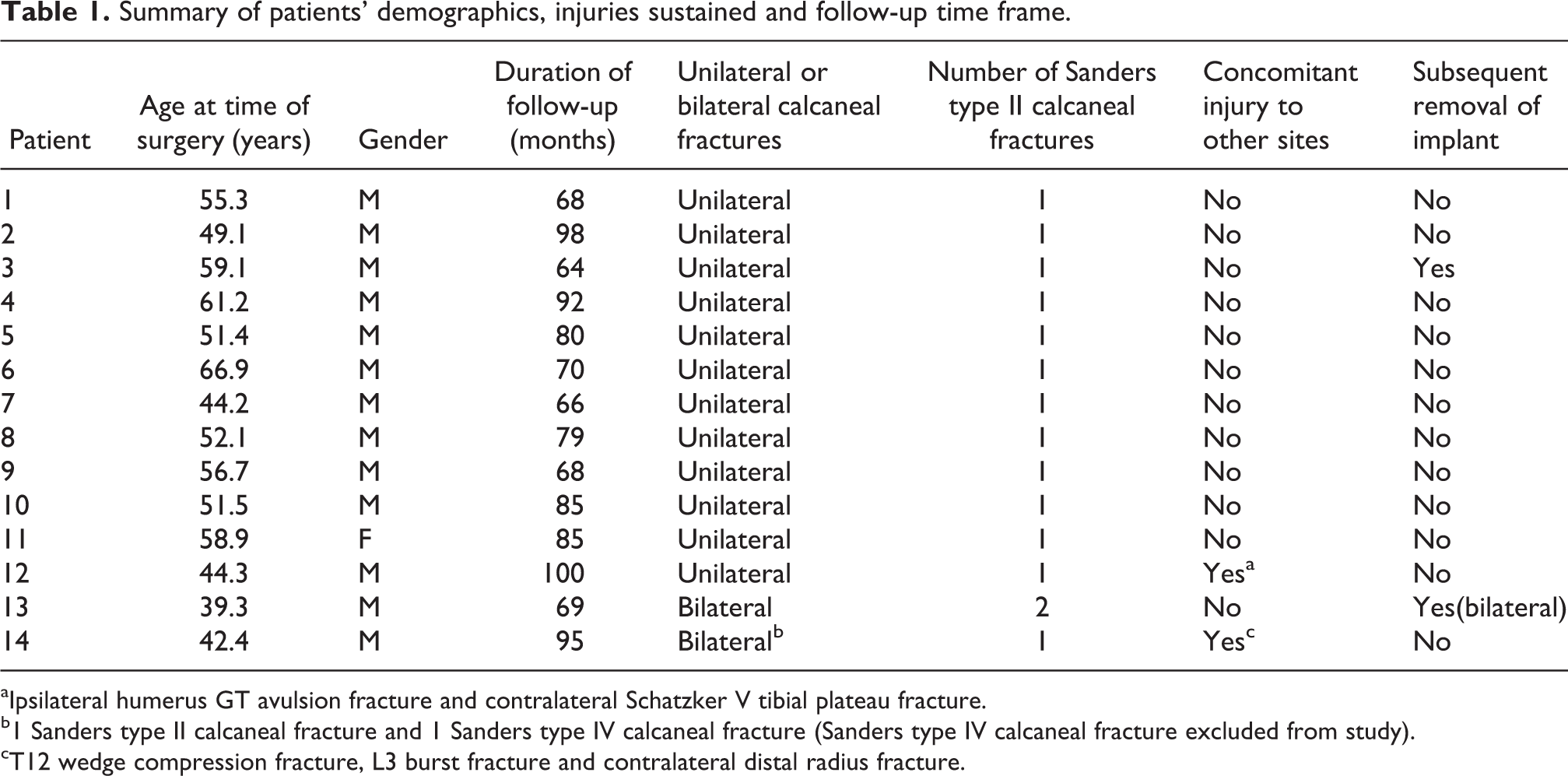
aIpsilateral humerus GT avulsion fracture and contralateral Schatzker V tibial plateau fracture.
b1 Sanders type II calcaneal fracture and 1 Sanders type IV calcaneal fracture (Sanders type IV calcaneal fracture excluded from study).
cT12 wedge compression fracture, L3 burst fracture and contralateral distal radius fracture.
Of the 12 patients with unilateral calcaneal fractures, 1 had concomitant trauma to other sites including an avulsion fracture of the greater tubercle on the ipsilateral humerus and a Schatzker V tibial plateau fracture on the contralateral side.
Of the two patients with bilateral calcaneal fractures, one patient had only one side that was amenable to percutaneous fixation guided by our dual-modality imaging. This patient also had concomitant trauma to other sites including T12 wedge compression fracture, L3 burst fracture and a contralateral distal radius fracture. His other calcaneal fracture was Sanders type IV, which was excluded from our study. The other patient had bilateral Sanders type II calcaneal fractures.
All other patients had isolated calcaneal fractures without concomitant injuries to other sites.
There were no conversions to open surgery in any of the reported cases. Three of the 15 cases in our study required removal of the metalwork. Of the three, two were secondary to discomfort due to screw prominence and one was due to patient’s preference. The patient with bilateral Sanders II calcaneal fractures had the metalwork removed in both calcanei, although only one was symptomatic. There were no other complications.
Surgical technique
Images and surgical technique described in this section are adapted from our original article by Woon et al. 9
Patients are positioned in the lateral decubitus position on the uninjured side. The suggested positioning of the image intensifier, arthroscopy equipment and personnel is shown in Figure 4 to facilitate the use of fluoroscopy and arthroscopy in our technique. The operative extremity is draped free with a tourniquet applied to the proximal thigh and the uninjured extremity is flexed at the knee.
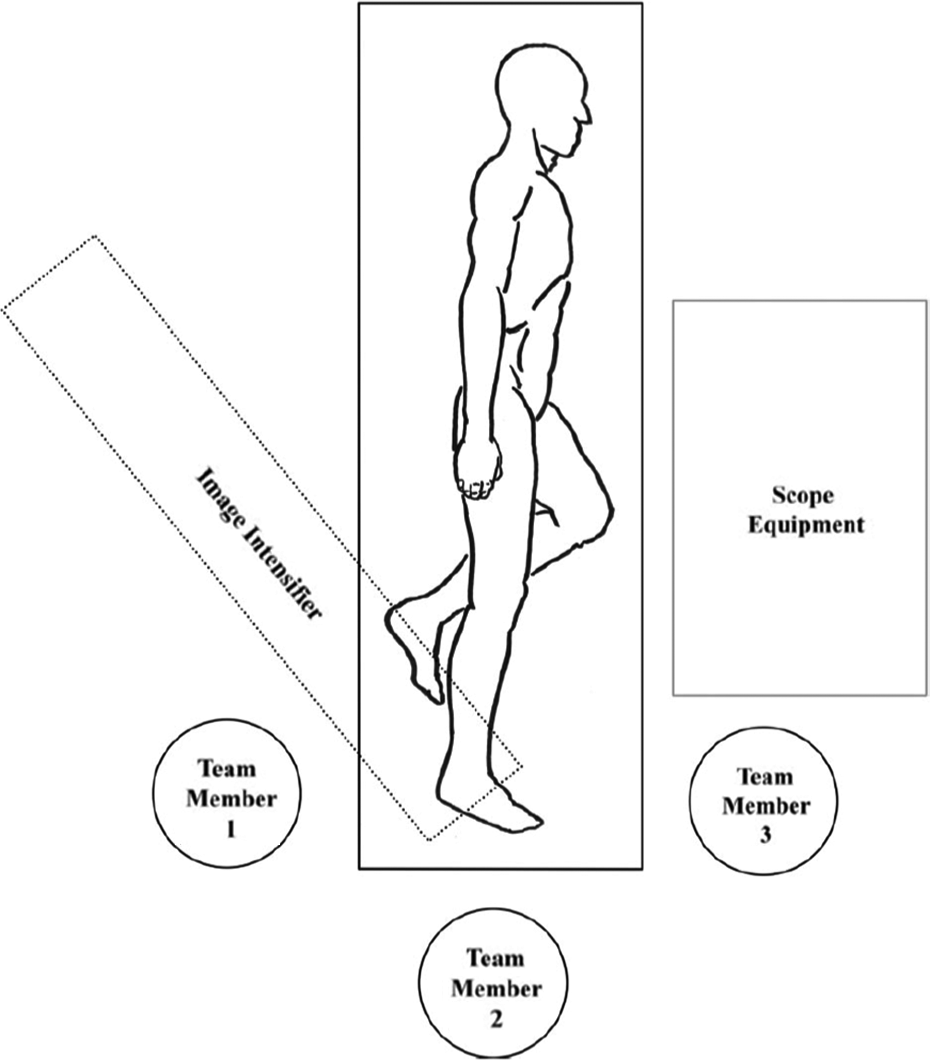
Suggested positioning of hardware and personnel.
The introduction of a wrist arthroscope (2.4 mm, 0°, Stryker) through anterolateral and midlateral portals, as shown in Figure 5, allows optimal visualization of the posterior facet without the need for release of the interosseous ligaments.

Placement of anterolateral and midlateral portals, percutaneous insertion of Schanz screw into tuberosity.
Examination of the posterior facet for incongruities is performed after joint irrigation, fracture haematoma debridement and removal of loose osteochondral fragments arthroscopically under direct vision. Manipulation and elevation of the superolateral depressed fragment is then performed with either Kirschner wires (K-wires) or using a periosteal elevator inserted into the fracture site through a stab incision over the lateral calcaneum. The reduction and correction of incongruities such as step-offs or gaps are confirmed both fluoroscopically and arthroscopically (Figure 6) with the acceptance of up to 1-mm residual step-offs and gaps without associated step-offs.

Arthroscopic visualization of articular step-off (a) before reduction and (b) after reduction.
The superolateral and sustentacular articular fragments are held temporarily using K-wires prior to the insertion of two cannulated or lag screws from lateral to medial just below the subchondral bone for stabilization of the fragments (Figure 7). Care must be taken to avoid the peroneal tendons. Large tenaculi or sharp bone reduction forceps can be applied to achieve compression before screw placement. Reduction of this ‘articular block’ to the tuberosity fragment is then achieved by manipulating a Schanz screw inserted percutaneously into the tuberosity via the Westhues manoeuvre (Figure 5). Varus or valgus deformity is also corrected at this time.

Examples of (a and b) preoperative and postoperative lateral, (c and d) axial and (e and f) Broden’s radiographs.
Fixation with fully and/or partially threaded cancellous screws is performed once satisfactory reduction is achieved (Figure 7). These screws are inserted with the aim to maintain calcaneum length and act as an internal scaffold to prevent collapse. They are inserted from the tuberosity to the calcaneocuboid joint and from the tuberosity to just beneath the posterior facet, respectively. Additional screws are inserted as deemed necessary to stabilize larger fragments.
All patients were placed in a short-leg cast postoperatively. Removal of the cast and stitches is performed at 2 weeks postoperatively.
The supervised rehabilitation program involves non-weight bearing crutch ambulation from 3 weeks to 6 weeks postoperatively, partial-weight bearing (20 kg) from 7 weeks to 12 weeks postoperatively and full-weight bearing after 12 weeks.
Discussion
A review of the literature suggests that the role of subtalar arthroscopy in the management of intra-articular calcaneal fractures is still evolving. Our proposed technique with the use of subtalar arthroscopy and fluoroscopy in percutaneous fixation of intra-articular calcaneal fractures confers advantages from both imaging modalities and allows correlation between radiographic and arthroscopic appearances.
Arthroscopy allows excellent visualization of cartilage and joint surface with real time, close-up visualization of the disrupted subtalar joint. Small intra-articular steps and joint penetration by screws that can be overlooked on low-resolution fluoroscopy/plain radiographs can now be avoided. 1,10 In addition, avulsed fracture fragments lodged in the medial portion of the subtalar joint that are otherwise difficult to reach with the traditional lateral approaches can be removed arthroscopically.
Fluoroscopy addresses the limitations of treatment with arthroscopy alone by assisting in the detection of bony mismatch, determination of screw length, position and proximity to the joint surface, restoration of radiographic indices and evaluation of calcaneocuboid joint incongruities which can go unnoticed with arthroscopy inserted through standard portals. 10
Our study involved subtalar arthroscopy and fluoroscopy in percutaneous fixation of intra-articular calcaneal fractures in Sanders II, AO-OTA 83-C2 calcaneal fractures. In our previous study, we demonstrated good correction of Bohler’s angle and good functional improvements based on VAS, AOFAS and SFPF scores up to 2 years with minimal subsidence of Bohler’s angle over the same time frame. Our current study with long-term follow-up at 5–8 years echoed previous study results. Patients continue to show good functional outcomes based on similar evaluation parameters with the majority showing continued improvements after 2 years. There is again minimal subsidence of the corrected Bohler’s angle when compared to immediate postoperative radiographs over a follow-up time frame of minimum 5 years. The loss of Bohler’s angle is likely the result of bone loss and gradual bony resorption over load bearing surfaces. It is unknown whether this difference is of any clinical significance.
We believe that our technique should only be reserved for simple fracture patterns. As highlighted in our previous article, this is due to the technical difficulty involved in both reduction and maintenance of reduction in more complex fracture patterns. We believe that, in practiced hands, our minimally invasive technique of using dual-modality imaging with percutaneous fixation, is reproducible, can restore congruence to the posterior calcaneal facet in Sanders type II, AO-OTA 83-C2 fractures and is associated with improved long-term outcomes.
Study limitations
The main limitation in our study is the cohort size. Given the novel technique that was employed, the total number of patients who underwent the procedure was small. Of these patients, a significant proportion lost to follow up involved foreign workers who returned to their homeland after their contract expired. Others lost to follow up included patients who are uncontactable as a result of a change in contact details (e.g. phone number and addresses) given the long-term follow-up time frame. Of those that were contactable and declined to return for follow-up, the common reason given was that they have been asymptomatic for years and doing well, hence was not keen to return. One patient died secondary to her other comorbidities.
Conclusion
The combination of subtalar arthroscopy and intraoperative fluoroscopy in anatomical reduction of the posterior calcaneal facet of the subtalar joint in practiced hands is most useful in Sanders type II, AO-OTA 83-C2 fractures. Long-term follow-up at 5 years demonstrates good preservation of function as evidenced by NPRS, AOFAS ankle–hindfoot score and SFPF score.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.