
Abstract
Purpose:
Tendon harvesting for anterior cruciate ligament (ACL) reconstruction often injure sensory branches of the saphenous nerve (SN). Our purpose was to estimate the prevalence and postoperative course of sensory nerve injuries in bone patellar tendon bone (BPTB) autograft harvesting for ACL reconstruction.
Methods:
Between 2012 and 2014, patients who had primary ACL with BPTB autograft were included (n = 60) and interviewed specifically for sensory loss and its recovery. The surface area of sensory loss was documented. Evaluation also included demographic details, level of activity, and description of postoperative sensation disturbances.
Results:
The mean postoperative follow-up time was 24 ± 14 months. At the last follow-up, 46 (77%) patients reported on postoperative reduced sensation; however, only 35 (58%) remained with sensation loss. The most involved region of reduced sensation was of the infrapatellar branch of the SN. Three patients claimed they regret to have had the surgery specifically because of sensation loss and kneeling difficulties, while all others did not.
Conclusion:
Primary ACL reconstruction using the midline incision for harvesting the middle third of the patellar tendon autograft has a high prevalence of sensory nerve injury with a minor possibility for complete recovery within the first year. However, sensory loss secondary to this injury does not impair normal daily activities in these patients.
Introduction
The standard of care for a ruptured anterior cruciate ligament (ACL) of the knee in active persons with clinical instability is an arthroscopic autograft reconstruction. 1 With approximately 200,000 annual procedures in the United States, 2 the most popular autografts for reconstruction are bone patellar tendon bone (BPTB) or hamstring’s (HS) tendons. 3 The decision to recommend operative treatment for a person with a torn ACL is multifactorial and should also contemplate possible complications. Of these, the morbidity associated with harvesting the graft, such as anterior knee pain after the use of BPTB or reduction in knee flexion strength after the use of HS tendons, needs to be taken into account. 4 The various techniques for graft harvesting in ACL surgery are associated with local loss of sensation to the lower leg due to sensory nerve damage during the procedure, 5 –7 specifically the infrapatellar branch of saphenous nerve (IPBSN) and sartorial branch of saphenous nerve (SN). This type of injury may cause hypoesthesia, dysesthesia, painful neuroma, and reflex sympathetic dystrophy. Furthermore, anterior knee pain and kneeling pain have been directly related to the damage of some of its branches. 8,9 The incidence of IPBSN injury in ACL reconstruction changes according to the surgical technique and has been reported to be as much as 50% with the BPTB autograft technique and 30–59% with the HS’s technique. 10,11 The reports on the prevalence of these injuries are scarce and lack sequential follow-up, while the implications on patient satisfaction are not known. The aim of this study was to estimate the prevalence of sensory nerve injuries in BPTB autograft harvesting for ACL reconstruction and follow-up their postoperative course. The hypothesis was that these injuries are common, improve with time and are considered as minor by the patient.
Materials and methods
Between June 2012 and December 2014, a total of 227 patients had ACL reconstructions in our department that serves as a regional referral center for arthroscopic surgery. The study included patients who have had primary ACL reconstructions utilizing BPTB autografts. This study did not include patients who had multiligament reconstructions, meniscal repair procedures, surgery for synovial disease (e.g. rheumatoid arthritis, pigmented villonodular synovitis), ispilateral previous knee surgery, or worker compensation claim. Of the 63 patients who were eligible for inclusion, 60 had consented to participate and complete the follow-up (58 males, 2 females). The mean age was 26 ± 6 years.
All perioperative evaluations and operations were undertaken and reported by three senior orthopedic surgeons who work together in an academic knee arthroscopy regional referral center. In addition to the regular follow-up meetings at 2 weeks, 6 weeks, 3 months, and 6 months after surgery, the patients were interviewed at a minimum of 12 months after the index operation. The interview included questionnaires regarding sensation loss (Table 1) and current activity level (Tegner activity scale 12 ). The area of sensory loss was described and mapped according to a standard leg drawing. The most noticeable diameter of sensory loss was recorded and categorized as <5 cm, 5–10 cm, >10 cm.
Questionnaire for sensation loss.

Surgery was done under general anesthesia with the patient in a supine position. A leg holder and tourniquet were placed around the thigh of the affected leg. The harvest of the tendon was done using a midline longitudinal skin incision from the inferior pole of the patella to the tibial tuberosity. The subcutaneous tissue and the underlying bursa were then gently released with scissors. The central one-third of the patellar tendon was harvested together with bony plugs of the patella and tibial tuberosity, utilizing a double blade knife, electrical saw, and osteotome. The remaining gap was closed by suturing the edges of the patellar tendon. Arthroscopic ACL reconstruction was then performed. Standard anterolateral and anteromedial knee portals were used through the open incision of the tendon harvest. An additional medial suprapatellar portal was used for the purpose of water inflow during surgery and for inserting a drain at the end. The BPTB autograft was fixed by femoral and tibial interference screws (BioComposite; Arthrex Inc., Naples, Florida, USA).
All patients were discharged from the hospital 1 day after the surgery. A continuous passive motion device was used from day 2 to the first 2–3 weeks. Patients were allowed to bear weight as tolerated with a knee immobilizer and crutches for the first 2 weeks. A standard gradual rehabilitation protocol was followed for 6 months after surgery. Descriptive statistics were used for the purpose of prevalence calculations. Results were expressed by mean and standard deviation for parametric variables and by median and range for nonparametric variables.
Results
The mean postoperative follow-up time was 24 ± 14 months. At the last follow-up, 46 (77%) patients reported on postoperative reduced sensation; however, 11 of these patients experienced full recovery within an average of 8 months. Overall, 35 (58%) of the patients in the current study remained with sensation loss (29 incomplete and 6 complete). The most involved region of sensation loss (42 of 46 patients) was lateral to the midline incision with an area diameter of 5–10 cm, while four patients had a small (less than 5 cm) area of sensation loss at the midline incision scar. At the last follow-up, the median postoperative Tegner activity scale was 4 (range 0–9) points, which was the same as the preinjury level. Three patients claimed they regret to have had the surgery specifically because of sensation loss and kneeling difficulties, while all others answered it did not affect their daily function and in retrospect it would not have changed their decision for having surgery.
Discussion
The results of the current study show that the IPBSN was damaged by the direct longitudinal midline approach to patellar tendon graft harvesting during ACL reconstruction in most of the patients. Nevertheless, the loss of sensation was perceived by patients as a minor complication and had no influence on their daily function.
The IPBSN is a small nerve that supplies cutaneous sensation to the lower limb (Figure 1). The nerve itself is purely sensory, with no motor component, and it supplies the anterolateral aspect of the leg. 13 The prevalence of IPBSN injury secondary to ACL surgery varies among different studies depending on the type of incision and graft. 14 –16 Injuries to the SN and its branches are well reported with HS graft harvest 17 but remained underreported for traditional central third patellar tendon harvesting.
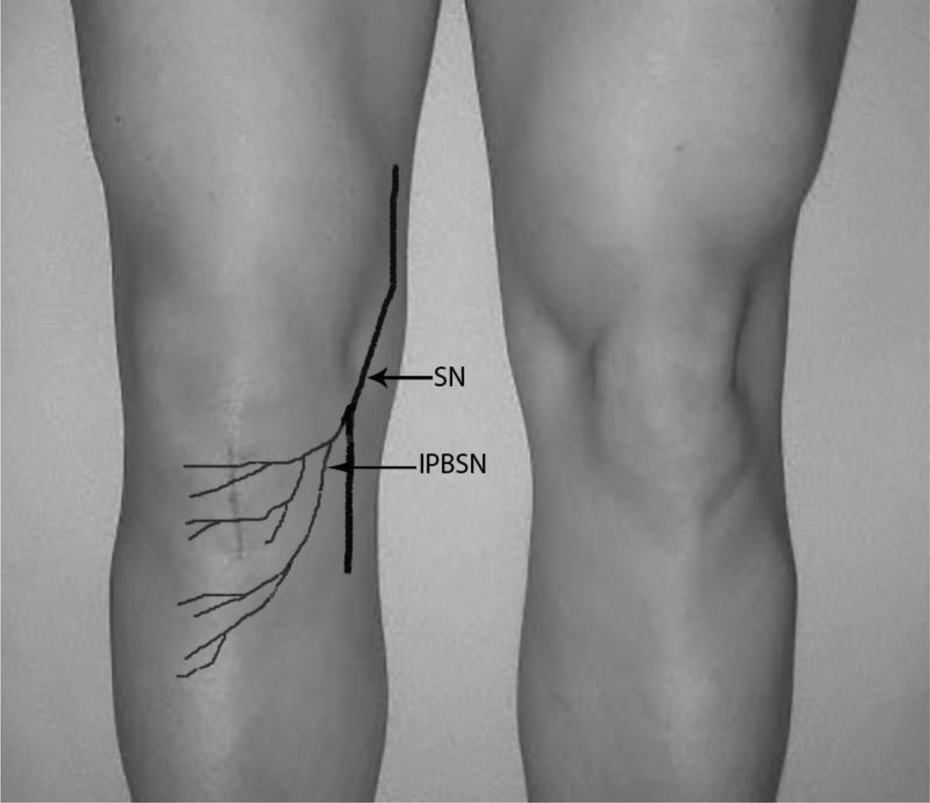
A drawing of the SN and the IPBSN on a right knee after patellar tendon harvest. Nerve injury may be minimized by identifying nerve branches or using horizontal incisions. SN: saphenous nerve; IPBSN: infrapatellar branch of the saphenous nerve.
Tsuda et al. 18 followed 75 patients after ACL reconstruction with a BPTB harvested using a two-transverse-incision technique. In their manuscript, they reported a previous cohort with the traditional longitudinal incision technique in which 93% of the patients experienced hypoesthesia or anesthesia over the area of the IPBSN; however, this percentage was lowered to 17% with the two-transverse-incision technique.
Recently, Gaudot et al. 19 have compared between mini-invasive double incision and traditional midline incision technique for BPTB harvesting. The mean follow-up was 32.7 months. The double-incision approach significantly reduced the midterm incidence of anterior knee pain and the occurrence of sensory disorders after ACL reconstruction. Hypoesthesia was found in 17 (90%) out of 19 patients in the single incision group.
Portland et al. 6 compared retrospectively between 42 patients who had a horizontal incision and 34 patients who had a vertical incision to harvest the central third patellar tendon as graft with a minimum of 2-year follow-up. Similar to the current study, 20 patients (59%) with a vertical incision had evidence of damage to the IPBSN as opposed to 18 patients (43%) with a horizontal incision.
In two studies involving 90 20 and 604 11 patients, respectively, Kartus et al. have reported that the inability to kneel and knee-walk after arthroscopic ACL reconstruction using patellar tendon autografts harvested through a vertical incision was correlated with the area of disturbed or lost anterior knee sensitivity. The clinical importance of damage to the IPBSN is amplified by the fact that the recent studies on arthroplasty 21 and tibial nailing 22 have shown that patient satisfaction is inversely correlated with the presence of injury to the IPBSN.
From cadaveric dissections, 23,24 it is clear that the damage to the infrapatellar nerve branches is unavoidable when a midline approach is used to harvest a patellar tendon graft. The location of these branches is highly variable; however, they consistently terminate over the patellar tendon (Figure 2). It is most likely that only some of the branches get damaged during the midline surgical approach. 25 This would explain the fewer incidences of patients complaining sensation loss over the anterolateral aspect of the knee, after this surgical approach.

IPBSN during patellar tendon harvesting. IPBSN: infrapatellar branch of the saphenous nerve. (Figure 2 is with permission from Oliveira JP, Fonseca F, Noronha JC. Anterior knee pain and sensitivity after anterior cruciate ligament: its impact on sports. OA Orthopaedics 2013 Aug 01;1(2):13.)
This study investigated the prevalence, recovery, and implications of sensation loss after BPTB harvesting, which is currently underreported in the literature; however, it has several limitations. This was a retrospective follow-up done in a single rather than multicenter study with only three surgeons involved. The results of their surgical technique and complications may not reflect the results in other centers. Physicians should inform candidates for ACL reconstruction with BPTB (midline incision) beforehand that there is a substantial risk for sensation loss but can also reassure them that it will probably not affect their function. If surgeons wish to minimize iatrogenic damage to the IPBSN, the direction of incisions should be parallel to the direction of the nerve when technically possible. We believe that our conclusions can help surgeons in their decision-making and informing patients on the expected nerve injury and its recovery.
In conclusion, ACL reconstruction using the midline incision for harvesting the middle third of the patellar tendon autograft has a high prevalence of IPBSN injury with a minor possibility for complete recovery within the first year. However, sensory loss secondary to this injury does not impair normal daily activities in these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.