
Abstract
Introduction:
The aim is to analyze the functional outcomes of patients of giant cell tumor (GCT) of distal radius treated with ulnar translocation and wrist arthrodesis.
Methods:
Study included 25 patients of aggressive GCT of distal radius, resected and reconstructed using ulnar translocation and wrist arthrodesis. The ulna-carpal radius fixation was performed with plate and screws. The patients were followed to bony union and minimum follow-up was 1 year.
Result:
Twenty-two patients were of Campanacci grade 3 and three patients were of Campanacci grade2. The mean follow-up was of 23 months (12–36). All patients had an excellent range of pronation and supination. The mean Musculoskeletal Tumor Society score was 24 (range 22–28). Grip strength of affected hand compared to the contra lateral hand was found good in 17 cases and average in 7 cases. The mean bone union time at ulna to radius junction was at 6.5 (5–8) months and ulna to carpal junction at 4.5 (4–6) months. The complications were surgical site infection (one case), recurrence (one case) and failure of union (one case), and ulna graft fracture with implant failure in (two cases).
Conclusion:
Reconstruction of distal end of radius using ulnar translocation and wrist arthrodesis provides excellent functional outcomes with preservation of rotational movement of forearm and hand function. Reconstruction of the distal radius by ulnar translocation without complete detachment from surrounding soft tissues functions like vascularized graft without use of microvascular techniques.
Introduction
Giant cell tumor (GCT) of bone is a benign but locally aggressive tumor and the treatment consists of either curettage or en bloc resection of the lesion with subsequent reconstructions. 1 –4 Distal radius is the third most commonly involved site of skeletal GCTs (10% cases) next to distal femur and proximaltibia. 1,2 The tumor removal and reconstruction of defect in GCT of distal radius is relatively difficult due to epiphyseal–metaphyseal location and presence of radial artery and median nerve in close proximity. 4
Aggressive GCTs poses question to the surgeon about the surgical planning for complete removal of the tumor with reconstruction modality for better preservation of the forearm and hand function. 5 –7 Different surgical modalities have been advocated for the management of GCT of distal radius. 3,4,7 –17
The treatment modality for GCT of the distal end of the radius should suit patient best as per the profession and requirements. Resection of the tumor and reconstruction of the distal radius by ulnar translocation without complete detachment from surrounding soft tissues was first described by Seradge H. 18 Although ulna translocation has its demerits, that is, loss of movements at wrist and weak grip strength. 18 –22 The majority of literature on the treatment of GCT of distal radius subject focuses on the resection of the tumor followed by reconstruction methods, and however, papers analyzing the functional outcomes of this procedure are scanty. 3,4 The aim is to analyze the functional outcomes of patients of GCT of distal radius treated with ulnar translocation and wrist arthrodesis.
Methods
The study included retrospective cases of patients who were operated in our hospital for aggressive GCT as defined by Campanacci of the distal end of radius by resection of tumor and reconstruction with ulna translocation and wrist arthrodesis from 2012 to 2016. According to the Campanacci classification, grade I tumors involve a well-marginated border of a thin cortical rim of mature bone, and the cortex is intact or slightly thinned but not deformed. Grade II tumors involve relatively well-defined margins but no radio-opaque rim. Grade III tumors involve a fuzzy border. The medical records and plain roentgen graphs and MRI were carefully studied (Figure 1). In all the cases, a biopsy specimen was obtained prior to definitive surgery using the core biopsy needle. The bone resected at time of definitive surgery was also sent for histopathological evaluation. Forearm was positioned in prone position and under general anesthesia and tourniquet control, a posterior incision was made. The superficial branch of the radial nerve was identified and protected. The radius was approached through the space between the brachioradialis and the extensor carpi radialis longus. The proximal margin of tumor was marked as per preoperative planning. The whole distal portion of the radius with the tumor was removed. The distal third of ulna was exposed with intact muscle cuff and resected as per the defect created after radius tumor removal. The distal end of ulna was cut transversely with saw. The scaphoid and carpal bone was cut with saw. The resected ulna is then placed into the place previously occupied by the radius and fixed to the proximal fragment of the radius with dynamic compression plate. A dynamic compression plate is bend to two regions, that is, ulnocarpal junction and radius ulna junction. Wrist arthrodesis is performed with forearm in mid-prone position. Prior to final fixation, full pronation and supination is checked. A volar plaster is applied until suture removal splint after closing the wound in layers over a suction drain. This was followed by below elbow cast for 2 months duration. Graded exercise program were guided by the postoperative clinical and radiological status. Serial radiograph is performed monthly to assess bone union (Figure 2). The patients were called for follow-up every 2 month for first year and subsequently every 6 months. The patients were followed to bony union and minimum follow-up was 1 year. The clinical observations were made regarding recurrence of tumour, functional status, and hand grip strength. Radiological criteria of assessment were local recurrence, status of bone union, stability at ulnocarpal junction, and deformity. The patient’s Musculoskeletal Tumor Society (MSTS) score was calculated at every follow-up. Handgrip strength was measured using a grip strength measuring device with a spring action; the strength was graded into good, fair, or poor as per the following criteria.

Plain radiographs showing lytic expansile lesion in distal radius.

Bone union seen at both osteotomy sites.
Results
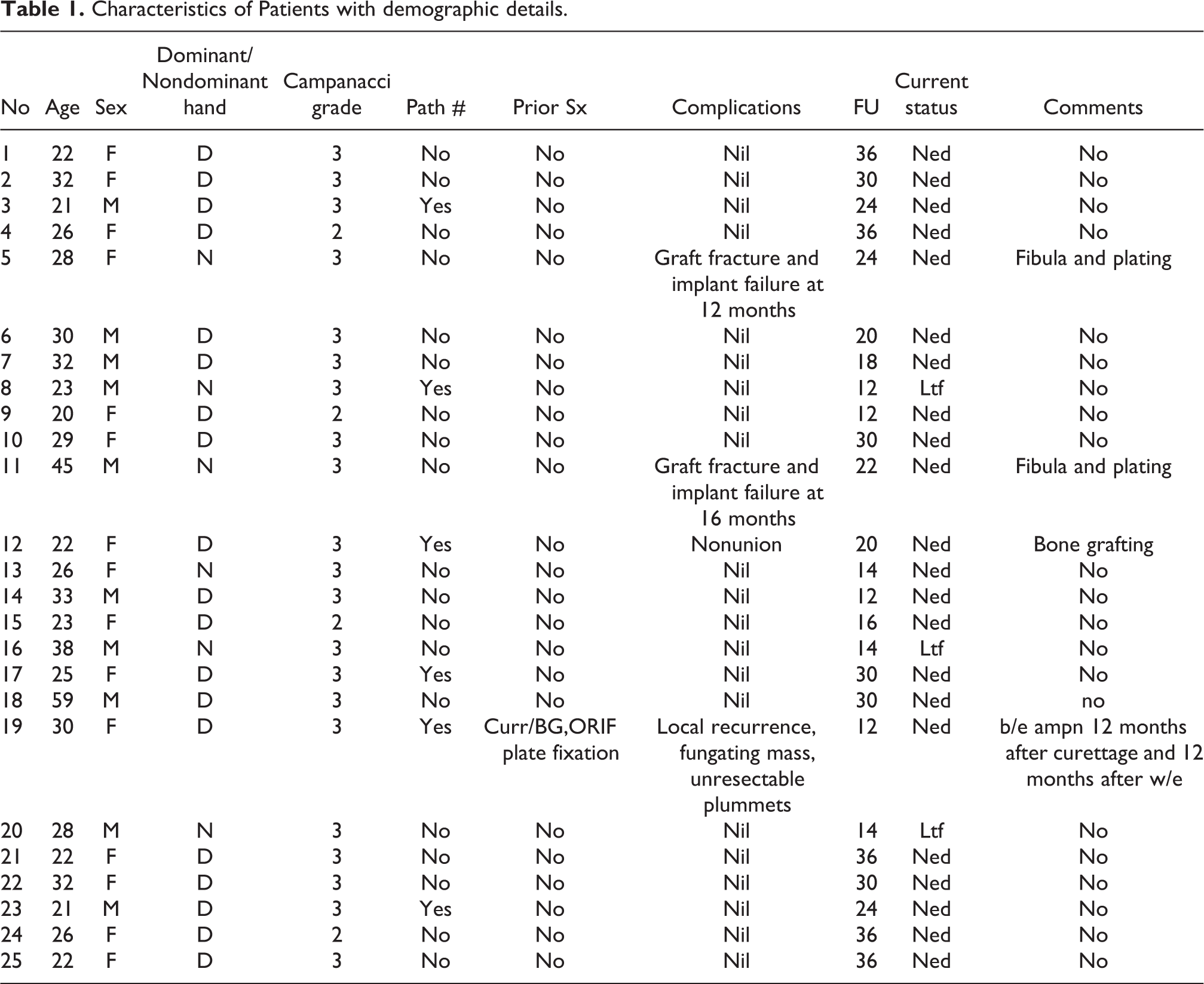
Of the 25 patients analyzed, there were 10 males and 15 females with 19 dominant and 6 nondominant sided involvement of distal radius. The mean age of patients was 29 years (21–59 years). Twenty-two patients were of Campanacci grade 3 and three patients were of Campanacci grade2 (Table 1). One of the cases had pathological fractures and none of the cases had metastatic disease at presentation. The mean follow-up was of 23 months (12–36).
Characteristics of Patients with demographic details.
There was one case of recurrent GCT initially treated with extended curettage with recurrence detected at 12 months after ulnar translocation. The mean resected length of the radius was 8.6 (range 7–10) cm. Early radiological union at host–graft junction was achieved at 12–14 weeks (mean 12.5 weeks) and solid incorporation with callus formation was seen in 28–32 weeks (mean 29) in all the cases (Figure 4). The mean bone union time at ulna to radius junction was at 6.5 (5–8) months and ulna to carpal junction at 4.5 (4–6) months. All patients had an excellent range of pronation and supination (Figures 3 and 4). The mean MSTS score was 24 (range 22–28). Grip strength of affected hand compared to the contralateral hand was found good in 17 cases and average in 7 cases (Table 2).

Clinical photograph showing forearm pronation with fingers in flexion.

Clinical photograph showing forearm supination with fingers in extension (black arrow on unaffected limb).
Functional outcomes and MSTS score.
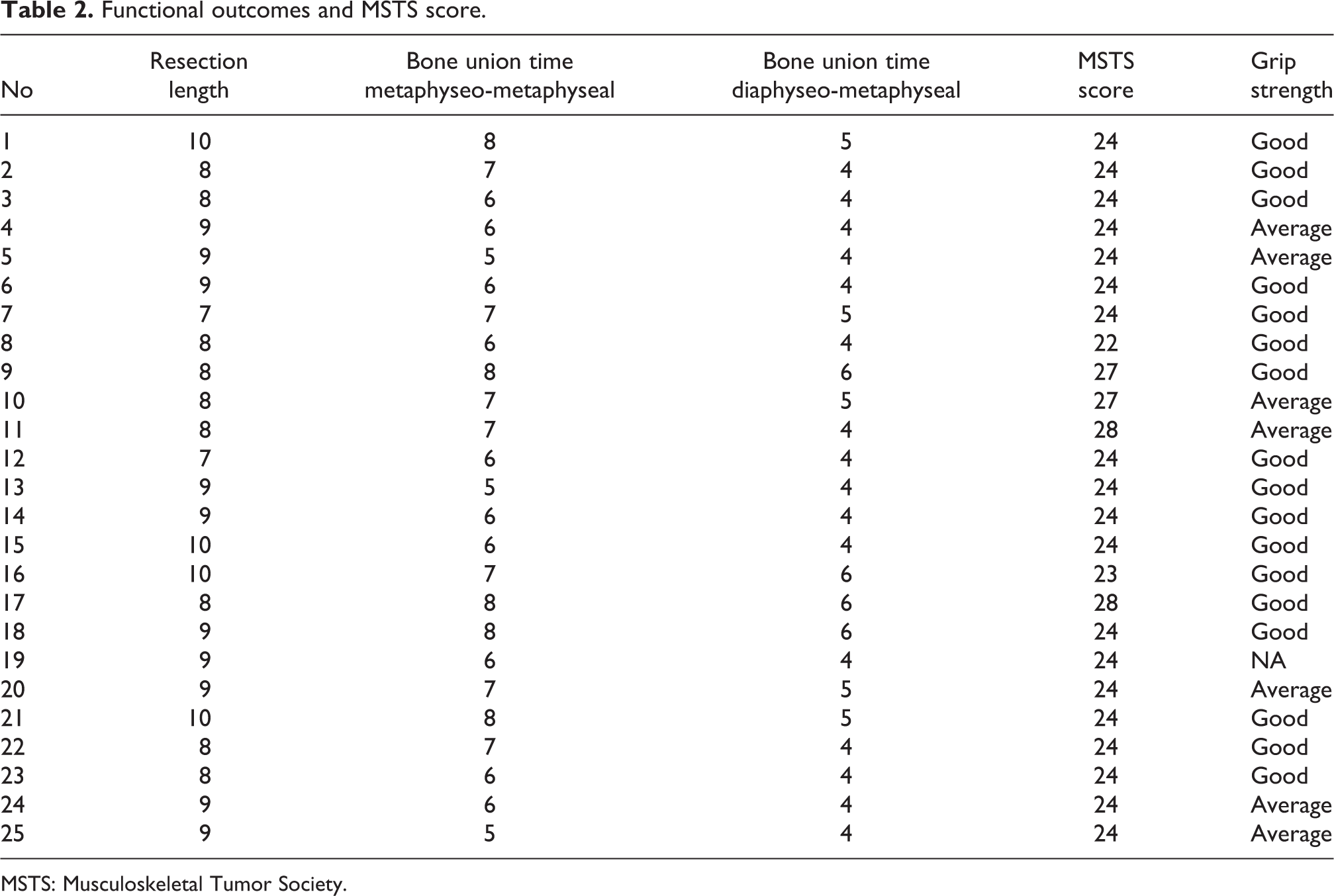
MSTS: Musculoskeletal Tumor Society.
The complications were surgical site infection (one case), recurrence (one case) and failure of union (one case), and ulna graft fracture with implant failure in (two cases). Case no. 7 developed infection was treated by thorough debridement and appropriate antibiotics and infection subsided in one month’s time. Case no. 19 was a recurrent GCT treated earlier with curettage and bone grafting and developed local recurrence at 18 months after surgery. This patient developed soft tissue and any bony recurrence and unresectable pulmonary metastasis was treated with below elbow amputation in view of fungating mass with complete encasement of neurovascular structures. Case no. 12 had nonunion at radius ulna junction and was treated with bone grafting and the osteotomy site united in 3 months duration. Two patients (Case no. 5 and 11) had fall at 12 months and 16 months which lead to fracture of ulna graft and implant failure. Both cases were treated with fibula graft and locking plate fixation and bone grafting.
Discussion
GCT of distal radius affects young patients with relatively normal life expectancy so it’s tough for management and rehabilitation. Local recurrence and loss of joint function are challenging task to control in GCT surgery. Curettage and filling of void with bone graft or bone graft helps to achieve wrist function but is having very high chances of local recurrence (30–50%). 1 –7 The use of a free nonvascular proximal fibular graft to replace the resected distal radius was described by Mays et al. 9 This method requires prolonged immobilization and is having multiple complications of delayed union, nonunion, and graft resorption, loss of function, stress fracture, deformity, and failure of internal fixation. Wide resection is suggested for most grade 3 and few grade 2 GCT of distal radius. 1 –6 Very few studies on ulnar translocation with assessment of functional outcomes have been published in medical literature. 18 –22 In current study, wide resection and reconstruction with translocation of ulna and wrist arthrodesis was performed. The ulnar translocation provides multiple advantages over use of free vascular and nonvascular fibula and allograft. 18,21 The requirement of microvascular training and risk of vascular damage with its complications are avoided. The facility of bone bank with allograft procurement is not available at multiple centers. Also, there is high risk of infection and graft rejection following use of allograft.
The literature on use of distal radius replacement with artificial prosthesis is not convincing for replication due to its complications. 14 The donor site morbidity in form of separate scar at fibula osteotomy, risk of nerve injury and damage to lateral collateral ligament, and iatrogenic implantation is avoided. 9 This procedure helps to provide forearm pronation and supination with preservation of hand function. The surgical timing for ulnar translocation is relatively shorter as compared to vascular and nonvascular fibula transfer. The vascularity of the ulna graft is maintained due to adequate muscular cuff and it aids in bone union. Translocation of ulna doesn’t provide cosmetically acceptable appearance due to narrowing of wrist and distal forearm giving an hourglass appearance to the limb.
The complication in current series was comparable with the other published literature on ulnar translocation. The common complication of ulnar translocation without wrist arthrodesis is wrist subluxation. 23,24 Saini et al. showed that wrist subluxation which occurred almost in every case and was managed with removable wrist splint worn during night and as needed due to pain during the day time. 23 The wrist instability is avoided due wrist arthrodesis and provides a stable wrist joint.
In current study nonunion was observed in one patient which was treated with bone grafting. Delayed union or nonunion has also been frequently reported. Role of primary bone grafting is debatable due to lack of robust literature on this topic.
The limitation of this study is small sample size and retrospective nature and no comparison group was used. So a multicenter study with a comparison group would be recommended for future studies.
Conclusion
Ulna translocation works like a local vascularized bone graft and carries the advantage of not requiring the facilities of microvascular surgery and allograft. Reconstruction of distal end of radius using ulnar translocation and wrist arthrodesis provides excellent functional outcomes with preservation of rotational movement of forearm and hand function.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.