
Abstract
Purpose:
Pipkin type IV femoral head (FH) fracture was thought as poor prognosis. There were several surgical approaches and treatments for this difficult fracture. However, there was no one treatment superior to another. We reviewed a serious of patients with Pipkin type IV FH fracture underwent surgery via a modified Gibson approach.
Methods:
We reviewed a consecutive series of nine patients with Pipkin type IV FH fracture under surgery via a modified Gibson approach between 2012 and 2013. The surgical procedure was completely described, and the radiological outcome and the functional outcome were also reviewed.
Results:
The mean follow-up duration was 17 (12–30) months. The mean Merle d’Aubigne score was 16 (8–19). Seven patients had anatomical reductions, and two had imperfect reductions by Matta’s grading. There was no early posttraumatic osteoarthritis during the follow-up period. One patient with early post-traumatic osteonecrosis 3 months after index surgery underwent total hip arthroplasty.
Conclusions:
Through this surgery approach to fix the FH and the acetabulum, the radiological and the functional results were satisfactory. We still need more patients with prospective study to find an optimal surgical approach for Pipkin type IV FH fracture.
Background
Fracture-dislocations of the hip joints are uncommon injuries and are usually the result of high-energy trauma. 1 –3 According to the literature, femoral head (FH) fractures account for 7–16% of all hip fracture-dislocations. 4 –7 Treatment for FH fracture mainly depends on the fracture type. In general, surgical intervention is reserved for a major fragment displacement of more than 2 mm and a non-congruent hip joint. 8,9
In 1957, Garrett Pipkin described a simple and useful classification for FH fractures. Since then, Pipkin’s classification has been commonly used to evaluate FH fractures. Among the four types of fractures in this classification, Pipkin type IV fractures are believed to have poorer prognosis. 3,9 There are several surgical approaches for the treatment of Pipkin type IV FH fractures, including the Watson-Jones approach, Smith-Peterson approach, the Kocher-Lagenbeck approach with a trochanteric flip osteotomy and anterior dislocation of the hip, 10 –12 and the modified Heuter approach. 13 However, no one surgical approach has been ascertained to be superior to the others. In this article, we report an alternative surgical approach to reduce and fix both acetabulum posterior wall (PW) and FH fractures.
Materials and methods
Between July 2012 and June 2013, nine cases of Pipkin type IV FH fractures underwent surgical treatment by a single surgeon (YHY) in Chang Gung Memorial Hospital, a referral hospital and a level 1 trauma center in North Taiwan. All patients were admitted to the hospital either through the emergency department (ED) or by referral from the local hospital after initial resuscitation. The resuscitation protocol followed the Advanced Trauma Life Support guidelines and was completed in the ED.
As soon as the hemodynamic status of the patient stabilized, the image studies were performed at the ED. The X-rays for the chest and pelvis are the standard image study initially. However, during resuscitation stage, whole body computed tomography scan (CT) scan was often performed for clarifying major organ injuries. Regarding to the pelvic and acetabular fractures, a 3D reconstruction CT scan was also executed. Whenever a dislocated hip joint was found, manual closed reduction was performed immediately either at the ED or in the operating room. None of the nine cases in this study required open reduction of the dislocated hip joint.
The indication for the FH fractures was the fractures involving suprafoveal area and incongruent FH after closed reduction of the hip joint. In addition, the indication for the acetabular fracture was the fracture involving PW. All fractures received definitive surgeries with open reduction and internal fixation between 3 and 7 days after injury. After the index surgery, plain radiographs in the pelvic anteroposterior (AP) view and two Judet oblique views were obtained. Each patient was allowed toe-touch ambulation for at least 6 weeks and then full weight bearing ambulation for another 6 weeks. Three months after surgery, the patients could walk freely without assistance.
Patients were assessed at intervals of 1, 3, 6, and 12 months after discharge. Thereafter, annual follow-ups were conducted annually. Functional and radiologic evaluations were performed and documented at each clinic visit. The functional results were recorded using the Merle d’Aubigne and Postel score. 14 Three parameters were used to evaluate the radiological outcomes: the accuracy of the reduction using Matta’s grading system and the osteonecrosis of the femoral head (ONFH) using the Ficat classification. 15
Statistical analysis was conducted using the SPSS statistical software package (version 15.0; SPSS, Chicago, Illinois, USA). Continuous variables were presented as mean values.
Surgical technique
Under general anesthesia, the patient was placed in the lateral decubitus position with the injured hip facing up. The incision field was covered cranially to the posterior iliac crest, anteriorly to the anterior iliac spine, and posteriorly to the gluteal fold. The injured leg was prepared in an aseptic field for manual traction and manipulation during the surgery (Figure 1(a) and (b)).
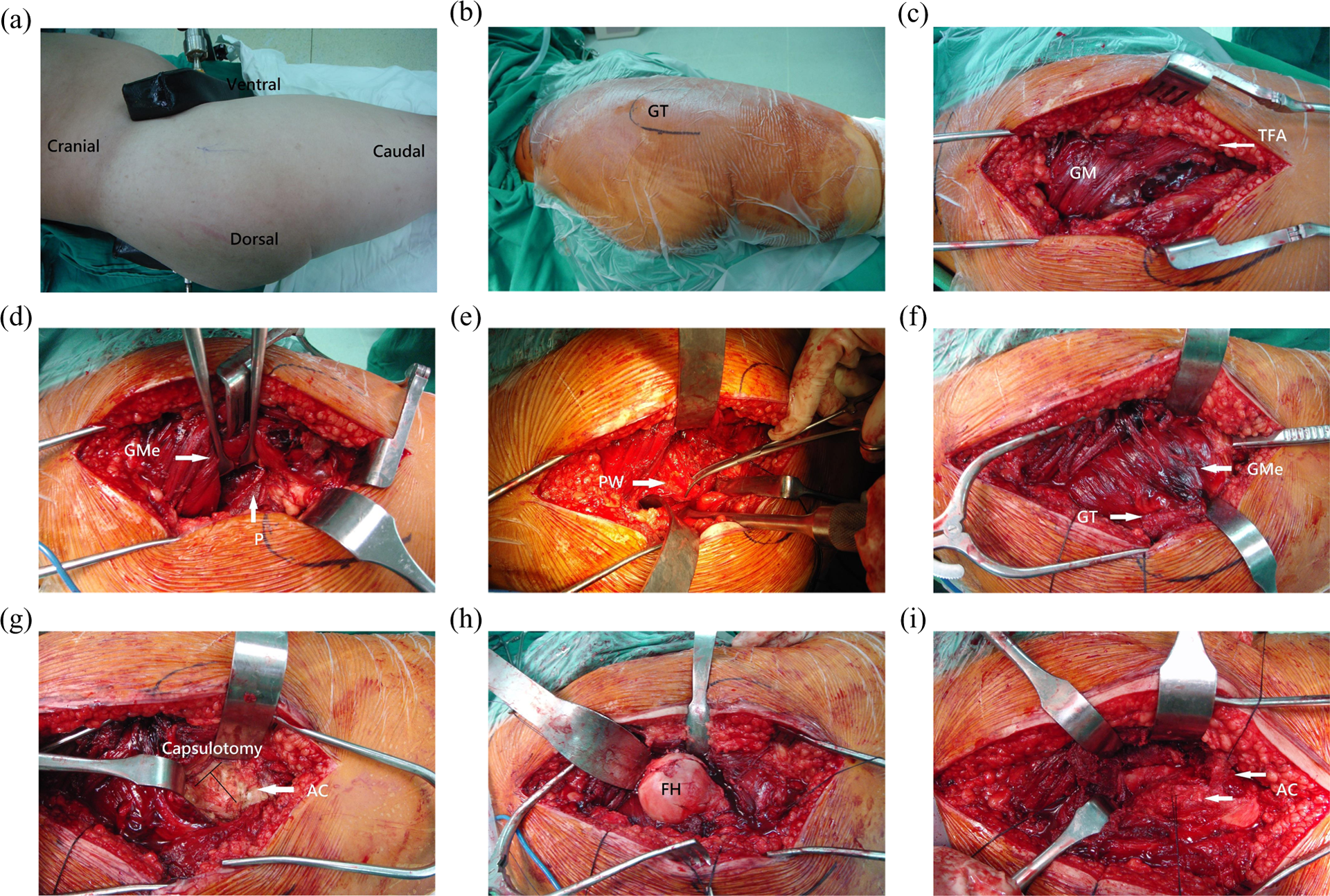
(a) and (b) The patient was in the lateral decubitus position. The GT was identified and marked. (c) After incision of the skin and dissection through the tensor fascia lata, the GM was met. (d) By retracting the GMe anteriorly, the short rotators were visualized. (e) After cutting the short rotators, the pathoanatomy was identified. (f) After reduction and fixation of the PW, the surgical field was changed for the modified Hardinge approach. (g) A T-shaped capsulotomy was performed at the radial portion of the acetabular site. (h) The FH was dislocated anteriorly. (i) After fixation of the FH, the AC was repaired and the hip joint was relocated. AC: anterior capsule; FH: femoral head; GM: gluteus maximus; GMe: gluteus medius; GT: greater trochanter; PW: posterior wall.
Our treatment plan was to first fix the acetabular PW and then fix the FH. We used a modified Gibson skin incision as described by Moed in 2010. 16 The skin was incised, and the subcutaneous tissue and fat were divided sharply. The fascia and tensor fascia lata along with the fascia of gluteus maximus (GM) was then incised sharply to create a deep dissection to the short external rotators for approaching the injured region of the affected hip (Figure 1(c) to (e)). The injured leg was kept in hip-extension and knee-flexion positions during the procedure to release tension on the sciatic nerve. We kept the soft tissue around the injured acetabulum as intact as possible, thereby minimizing the risk of nonunion.
The injured acetabular PW was reduced with manual traction, a pusher rod, and a point clamp and was temporarily fixed with Kirchner wires. After the PW was satisfactorily reduced, a pre-bent Judet reconstruction plate (DePuy Synthes, Paoli, Pennsylvania, USA) was applied as a neutralization plate.
Then, reduced and fixed the fractured FH. We maintained the hip and knee in the flexion position. We used the modified Hardinge approach, 17 which is primarily used in total hip arthroplasty (THA). In brief, we released the muscle-tendon junction of the gluteus medius (GMe) at the insertion of the greater trochanter (GT; Figure 1(f)). We then cut the gluteus minimus 1-cm medial to the edge of the GMe. A T-shaped capsulotomy was performed to release the anterior capsule (AC). The radial portion of the capsulotomy was performed at the acetabular site to avoid damaging the cervical vessels (Figure 1(g)). The hip joint was then dislocated, and the fractured fragments of the FH were viewed (Figure 1(h)). We used 3.5-mm interfragmental screws to fix and compress the fracture site. The hip was reduced, and the AC, gluteus minimus, and GMe were repaired layer by layer (Figure 1(i)). The wound was closed in layers with the absorbable sutures and suction drains left in the wound.
Results
During the study period, nine patients with Pipkin type IV FH fracture were treated using the modified Gibson approach (Figure 2). The locations of the fracture of the FH were four involving suprafoveal area and five involving infrafoveal area. All acetabular fractures involved PW. The patients consisted of eight males and one female with an age range of 18–40 and a mean age of 27. Of the admitted patients, seven suffered injuries from motorbike accidents, one had a dashboard injury from a car accident, and one had an injury from a fall. As soon as the fracture-dislocation of the hip was identified, the dislocated hip was relocated. The mean operation time for open reduction and internal fixation (ORIF) surgery was 202 (133–323) min, and the mean blood loss intraoperatively was 216 (100–450) ml. There were no perioperative complications. Seven patients had anatomical reductions, and two had imperfect reductions by Matta’s grading. All the patients were followed at the clinic in the mean duration of 17 (12–30) months. The mean Merle d’Aubigne score was 16 (8–19). Three months after the ORIF surgery, one patient showed early post-traumatic ONFH.

Case 2: (a) Right hip traumatic fracture-dislocation of a 33-year-old male after a motorbike accident. (b) and (c) X-ray following the surgery.
This patient was a 20-year-old male who, due to a motorbike accident, suffered a left side Pipkin type IV FH fracture (Figure 3(a)) and a left tibia shaft open fracture (Gustilo-Anderson type I). He underwent surgical debridement and internal fixation with an intramedullary nail (Zimmer, Warsaw, Indiana, USA) on the night of the accident. A manual closed reduction with low femoral skeletal traction was performed due to an unstable hip joint.

Case 8: (a) Left hip traumatic fracture-dislocation of a 19-year-old male. (b) Early ONFH after the surgery. (c) 6-month after ORIF surgery with total hip arthroplasty for left hip. ONFH: osteonecrosis of the femoral head; ORIF: open reduction and internal fixation.
Definitive surgery was performed 4 days after the injury. A comminuted fracture of the PW and infrafoveal FH fracture were found. The PW was buttressed with two semitubular plates as spring plates, and the displaced FH fragment was left in situ because the fragment was infrafoveal and there was no limitation of the range of motion of the hip joint.
At the 3-month follow-up, ONFH was noted on X-ray examination (Figure 3(b)). THA (Delta Biolox; Zimmer) on the left hip was then performed 6 months after the injury (Figure 3(c)). After THA, the patient was doing well at the 24-month follow-up.
Discussion
Alexander Gibson described the posterior approach for hip fractures in 1950. 18 Moed modified the Gibson approach using a straight skin incision for better exposure of the anterosuperior acetabulum, preservation of the neurovascular supply to the anterior portion of the GM, and decreased risk of iatrogenic sciatic nerve injury. 19 We used this same incision and approach to fix the acetabular wall and added a modified Hardinge approach to simultaneously fix the FH.
Surgical intervention for Pipkin type IV FH fracture is always necessary. For Pipkin type IV fractures that involve the infrafoveal part of the FH with a congruent hip joint, the acetabular PW fracture undergoes surgery, and the FH is left untreated. For Pipkin type IV fractures that involve the suprafoveal part of the FH or the infrafoveal part with a non-congruent hip joint, surgery is performed on both parts. Because the fractured part of the FH is always located anteromedially, it is difficult to fix the FH using the posterior approach and posterior dislocation of the hip. Therefore, reduction and fixation the FH must be performed through an anterior approach.
Different methods have been proposed for the surgical dislocation of the hip for the FH fracture. One of these procedures is trochanteric flip osteotomy. 10 –12 the greatest advantage of which is the improved exposure for anatomical reduction. However, there are occasional complications following the trochanteric flip osteotomy, such as nonunion, migration of the trochanter, and trochanteric bursitis from the prominent implants. 19 We avoided these morbidities and achieved the same reduction quality and stable fixation using this modified surgical technique.
The incidence of ONFH after surgical dislocation of the hip has always drawn attention. Previous studies documented that anterior surgical dislocation of the hip with a T-shape or Z-shape capsulotomy did not jeopardize the blood supply of the FH. 12,13 We came to the same conclusion in our previous study. 20 In the cadaveric study, the main blood supply of the FH was shown to come from the posterior-superior portion of the medial circumflex femoral artery. 12,21 Therefore, to avoid ONFH, while exposing the PW, it is critical to cut the external rotators 1 cm away from the insertion of the GT, which may decrease the chance of injury to the nutritional vessel.
In summary, we report a surgical approach for management of both FH and acetabular posterior fractures. The main advantage of this surgical approach was to fix both parts of fractures simultaneously in a single incision. Although there was one case that showed early post-traumatic ONFH and then underwent THA, we still believe that this technique is a promising and safe procedure for treating hip dislocations and associated fractures of the FH and acetabular PW. Based on the results, we need to study more patients to make the results conclusive.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.