
Abstract
Aim:
To identify whether the location of refractory patella tendinopathy (PT) has an effect on treatment modality (radial extracorporeal shock wave therapy (rESWT) or arthroscopic debridement).
Methods:
Between 2012 and 2014, 40 patients with PT underwent a magnetic resonance imaging (MRI) scan. This confirmed the diagnosis as either involving the tendon itself (group A, 20) or with retropatella fat pad extension (group B, 20). All patients underwent rESWT. If there was no improvement patients proceeded with surgery in the form of arthroscopic debridement (by senior authors CW and AG). Outcomes were assessed before and after treatment using the Victorian Institute of Sports Assessment-Patella (VISA-P) score.
Results:
There were 18 males and 2 females in group A and 15 males and 5 females in group B. The mean age was 41.4 years in group A (23–59) and 34.7 in group B (19–52). Seventeen of 20 in group A reported good or excellent outcomes and did not require surgical intervention (remaining three improved after second course of ESWT). All patients in group B failed to improve with rESWT, resulting in arthroscopic debridement and reported good or excellent outcomes. After 6 months, group A mean VISA-P score increased from 50.2 to 65.0 (p = 0.01) and group B from 39.6 to 78.4 (p = <0.001).
Conclusion:
An MRI should be performed to determine the precise location of tendinosis in patients with refractory PT who fail standard conservative management. If the MRI scan shows intratendon changes only, ESWT should be performed and those with extension into the fat pad should proceed to arthroscopic debridement without rESWT.
Introduction
Patella tendinopathy (PT) is a common chronic overuse injury causing pain over the inferior pole of the patella. It particularly affects recreational and elite athletes, with over 40% prevalence among elite basketball and volleyball players. 1 For this reason, it is also known as “jumper’s knee.” 2 Symptoms can be debilitating due to its chronicity, with some athletes prematurely ending their career as a result. 2
The aetiology of PT remains unclear, with repetitive overloading thought to play an important role. 3 It was previously believed that inflammation was central to the pathological process, but histological evidence rejects this. 4 This has led to the more appropriate term “tendinopathy” being used reflecting the degenerative nature of this condition and failed healing response. 5 Recently, it has been shown that the sympathetic nervous system has a direct influence on perivascular innervation of the dorsal paratendinous tissue of the patella tendon in arthroscopically treated patients which correlates with “neovessels,” found on color Doppler. 6
Both ultrasound and magnetic resonance imaging (MRI) have been used in the diagnosis of PT. Ultrasound has been the traditional approach to image tendons and shows an area of hypoechoic signal and increased thickness in the area of clinical tenderness. 7 An MRI has also been shown to identify signal changes within the proximal patella tendon and increased thickness. 8
Many treatment strategies have been suggested for PT but management still remains unclear due to the incomplete understanding of the underlying pathology. Conservative management includes rest, nonsteroidal anti-inflammatory drugs and physiotherapy including stretching and eccentric exercises. 9 The results of conservative management are inconsistent and can often lead to a prolonged clinical course. 10 Novel advancements, which show good outcomes, include extracorporeal shock wave therapy (ESWT), platelet rich plasma (PRP), and sclerosing injections. 11 –13 If conservative treatment fails, patients may proceed with surgical intervention in the form of either open or arthroscopic shaving. Up to 70% of open cases have good or excellent results 14,15 increasing to 92% when no bony work is involved, 15 and arthroscopic techniques have been found to be as effective as open surgery. 16
The ESWT used in medicine dates back to the 1970s for breaking up kidney stones (lithotripsy). In the 1990s, its use for treating chronic tendinopathies began. 17 In contrast to urological treatment (lithotripsy) where ESWT is used to disintegrate renal stones, it is used in musculoskeletal treatments (orthotripsy) to cause interstitial and biological responses resulting in tissue regeneration. 18 Since its introduction into musculoskeletal medicine, randomized controlled trials (RCTs) have shown that ESWT is effective for a variety of different tendinopathies, including rotator cuff, achilles, patella, extensor tendinopathy of the elbow, and in plantar fasciitis. 18 –20 The outcomes from these studies have a success rate of approximately 80%. Although the efficacy can be inconsistent, the National Institute for Health and Care Excellence has provided guidelines regarding its use. 21,22
So far, no studies have directly compared the effect of retropatellar fat pad involvement on treatment in refractory cases of PT. The purpose of this study was to identify whether the involvement of the fat pad has an effect on treatment modality (radial extracorporeal shock wave therapy (rESWT) or arthroscopy and debridement) and outcome.
Materials and methods
This single center retrospective study included patients with PT who presented to the senior authors (CW and AG) was performed at the University Hospital of Wales (UHW), between 2012 and 2014.
Patients were eligible for inclusion if they had a history of pain in the patella tendon, symptoms lasting more than 3 months (that had not settled with standard conservative treatment), aged between 18 and 60, had palpation tenderness of the patella tendon and had an MRI scan confirming the location and diagnosis of PT. All participants had to provide informed consent to be entered into the trial.
Exclusion criteria for the study included acute knee/patella injury, chronic joint disease, contraindication to ESWT (pregnancy, malignancy, and coagulopathy), previous knee surgery, or steroid injection in the previous 3 months.
All patients (40) underwent an MRI scan at UHW using a 1.5T MRI scanner (Echospeed, GE healthcare, Minnesota, USA). The MRI scan confirmed the diagnosis as either involving the tendon itself (group A, 20) or the retropatella fat pad (group B, 20; Figure 1). All patients underwent rESWT after failed conservative management. If there was no improvement in their symptoms, arthroscopic debridement was performed (by senior authors CW and AG).
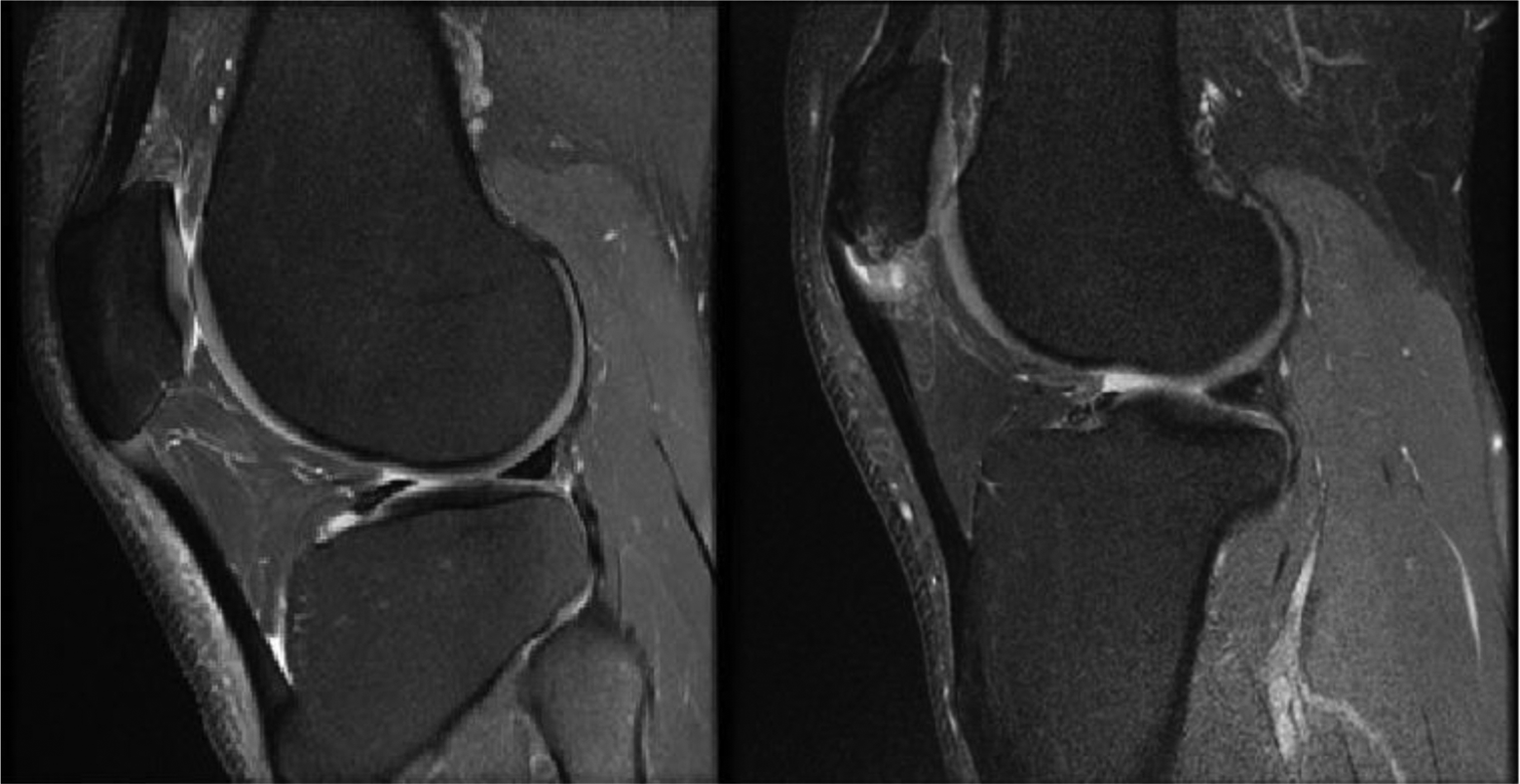
PD: proton density sagittal MRI. Left: group A—intrasubstance involvement. Right: group B—extending into the retropatella fat. MRI: magnetic resonance imaging.
Surgical technique
In all procedures, a 4.0-mm 30° high definition arthroscope, a 4.5-mm straight shaver blade, and a 90° bipolar ablation probe were used. The patients were positioned supine with a tourniquet. First, an arthroscopic inspection of the knee was performed via standard medial and lateral portals to rule out any other joint pathology. Initially, the most proximal part of Hoffa’s fat pad was debrided, both to remove an anticipated painful structure and to visualize the most posterior fibers of the proximal tendon.
Rehabilitation protocol
The knee was immobilized in extension in a functional brace for 3 weeks. Motion was gradually and partially restored until the fourth postoperative week. Full weight bearing was permitted after the third postoperative week.
All patients were scored before ESWT/arthroscopic debridement and again at 6 months afterwards using the Victorian Institute of Sports Assessment-Patella (VISA-P) score. Results will be analyzed using SPSS version 20 (SPSS, Chicago, Illinois, USA). The pre- and posttreatment VISA-P score will be assessed using the t-test. A value of <0.05 is considered statistically significant.
Results
The mean age was 41.4 years in group A (23–59) and 34.7 in group B (19–52). Seventeen of 20 in group A and all patients in group B reported good or excellent improvement. After 6 months, group A VISA-P mean core increased from 50.2 to 65.0 (p = 0.01) and group B from 70.1 to 90.7 (p = <0.001; Figure 2).

Breakdown of results for groups A (left: ESWT, p = 0.01) and B (right: arthroscopy and debridement, p = 0.001) pre- and posttreatment. ESWT: extracorporeal shock wave therapy.
Discussion
The patella tendon is particularly vulnerable to injury and difficult to manage successfully. 23 Many treatment strategies have been suggested but management still remains unclear due to the incomplete understanding of the underlying pathology. If standard conservative measures fail, alternative novel techniques may be used.
Hoksrud and Bahr used ultrasound guided sclerosing injections in 33 patients with PT. 12 They reported statistically significant improvement in VISA scores 12 months afterwards. However, these effects didn’t persist and when interviewed by telephone at 44 months, a third of patients (12/29) had undergone arthroscopy. 12
Filardo et al. have used PRP for refractory PT. 13 In this study, they compared PRP with regular physiotherapy and found that both groups were found to have statistically significant improvements in pain and movement at 6 months. There was no comparison group in their study, and as a result, it is not clear as to the real contribution PRP has in PT. The ideal number of PRP injections required is not yet established, and the rationale for its use still remains unclear.
ESCT is the most published of the novel treatments with regard to PT with numerous papers investigating the efficacy of ESWT (RCTs, case series, and case control studies). 24,25 These studies concluded that ESWT seems to be a safe and effective treatment for PT, with approximately 74.7% of patients reporting an improvement in pain and knee function. 25 Unfortunately, all these studies have used different protocols, making it very difficult to perform a meta-analysis allowing a standardized treatment protocol for PT. One of the few consistent findings with ESWT is that they all had a minimum of three sessions.
There are two different types of ESWT—focused and radial. Focused ESWT can be generated by electrohydraulic, electromagnetic, or piezoelectric mechanisms. 26 In all of these three cases, the shock wave is generated in water and focused into a tube before being transmitted into tissues. Radial ESWT waves are formed by accelerating a projectile through a tube before hitting an applicator which is in contact with the skin. As a result of the difference in wave generation between the two types, radial shock waves have a more superficial effect as the maximum focus energy is at the skin compared to focus shock wave which has a focus located deeper within the tissue. Despite these differences, there has been found to be no difference clinical results between the two different types. 27
It still remains unclear exactly how shock wave treatment works. Several theories have been proposed although there is no universally accepted model. One theory suggests that shock waves damage cell membranes preventing nociceptors transmitting pain signals.
28
Others include as follows: Shock waves stimulate nociceptors to send high frequency impulses which are suppressed by a gate control mechanism.
29
Shock waves produce free radicals which change the chemical milieu resulting in release of pain suppressing substances.
29
Shock waves produce hyperstimulation analgesia which acts on the brainstem exert inhibitory control over neural transmission through the dorsal horn.
29
Interpretation of the results of RCTs that have been performed should be with caution as the quality is variable. 30 Only one previous arthroscopic surgical study investigated the removal of neovessels on the dorsal side of the proximal patella tendon on patients’ outcome. 31 At follow-up at 6 months, they found good clinical results with satisfied patients back to previous sporting activity level with reduced pain. 31 However, no approved formal scoring system was used in this study, which relied on the visual analogue scale for pain to measure the improvement of symptoms. All of the published studies have looked into the effect of ESWT regardless of location of where PT is on imaging results.
Open shaving has shown good or excellent results in up to 70% of cases 14,15 increasing to 92% when no bony work is involved. 15 There has been shown no difference between arthroscopic versus open surgery 16 but patients prefer arthroscopic surgery due to the lower morbidity and smaller scars.
Our results showed similar outcomes to those previously published. Group A had good outcomes in 80% using ESWT, which is similar to that found in the literature. 24,31 Three patients had only a small improvement in their VISA scores and as a result brought down the mean score in this group. They required a second course of treatment which improved their symptoms. All patients in group B initially failed rESWT treatment requiring arthroscopic debridement. Postsurgery they all had a good or excellent outcome, with all patients returning to their original preinjury sporting activities. These results would agree with Willberg et al. that arthroscopic shaving of the dorsal aspect of the proximal tendon significantly improves patient’s outcomes in specific cases. 31
In our department, all patients presenting with refractory PT undergo an MRI scan to determine the location and to identify any retropatella fat pad involvement. Patients with intrasubstance involvement proceed with ESWT and those with fat pad involvement proceed straight for arthroscopic debridement without experiencing ESWT. We do not have any other form of novel treatment in our department, as we have achieved good to excellent outcomes in the past by dealing with PT using ESWT, and sclerotherapy and PRP treatments are relatively new and need authenticating. 32
It was difficult to have a control group in this study, as it would have been impossible and unethical to subject them to a further round of classical conservative therapy.
The length of follow-up for this study is relatively short, and the short-term effects may not continue in the long term. However, it would be highly unlikely that high functioning athletes would be willing to receive placebo for a sufficient time.
Other weak points of this study are represented by the lack of randomization and the small numbers of patients treated. Nonetheless this study shows interesting results that could be elaborated in the future in larger randomized studies.
Our results suggest that the location of PT results in good outcomes when treatment is focused. However, as this is only a small pilot study, we would recommend further research to investigate this.
We observed a significant improvement in all scores evaluated in both groups over the 6 months follow-up. The majority of patients had a good recovery, returned to previous sporting level, and were satisfied with their outcome.
Conclusion
Patients with refractory PT should undergo an MRI to determine the location and involvement of the fat pad. If the MRI scan shows intratendon changes, ESWT should be performed resulting in good outcomes. Those patients showing fat pad involvement have good outcomes with arthroscopic debridement without rESWT.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.