
Abstract
Tumours and metastases of the spine are extremely stressful for patients, especially for elderly multimorbid patients. The modern cavity/coblation method offers a very good therapeutic alternative for such patients. The goal of this article was to evaluate and present the characteristics, significance, opportunities, issues of the minimum invasive cavity/coblation method as well as the results of the treatment of 302 patients with vertebral tumours and metastases.
Keywords
Introduction
Tumours and metastases in the spine are strong onerous conditions for patients. The treatment of these diseases has advanced considerably in the past centuries. However, many patients with multiple metastases with bone destruction, especially osteolyses and fractures in multiple vertebral bodies or other organs, were limited to traditional therapeutic methods such as chemotherapy and possibly radiation, pain management and so on.
Traditionally recognized methods are cryotherapy, thermotherapy or laser therapy and radiofrequency. When cryotherapy is operated at very low temperatures, it is very labour-intensive, is unable to remove all metastatic tissues completely and is highly likely to damage healthy tissue. 1,2 Thermo-/laser therapy operates at higher temperatures, locally at 500°C, and has considerable damage potential to healthy tissue. 3,4 Radiofrequency, for example, with Rita Starburst magnetic resonance imaging (MRI) device, is operated with radiofrequency current, generates a very high temperature (more than 400°C) to damage tumour cells, is not able to fully destroy tumours/metastases and is also able to damage surrounding healthy tissues, nerves and vessels. 2,5,6
The execution of radically open and lengthy operations for solitary metastases, such as the anterior and posterior fusions with vertebral body replacement, are linked to considerable intraoperative and post-operative risks. Examples of such risks are massive bleeding at a larger access, tumour resection, increased injury risk for blood vessels, nerves as well as wound healing disturbance and considerable infectious risk due to large contamination area and long operation times. Many different interoperative and post-operative complications, such as loosening and fractures of the osteosynthetic material and decompensation of neighbouring spine segments, are very frequent. 7 –10
Furthermore, there are contraindications for larger operative procedures in the spinal area for many patients with a reduced general condition. Especially high-risk patients such as patients with cardiopulmonary limitations make longer operational times and blood loss impossible, in particular when considering the questionable success of large invasive procedures. Above all, in both curative as well as palliative situations, the goals of the operative procedure are as follows: a low traumatization of the soft tissue and bones through a minimal invasive technique, the reduction of blood loss, maintenance of stability of the vertebra and the spinal segment, adjusting the deformation or repositioning the compressions fracture, the decompression and expansion of the spinal canal with possibly complete removal of tumour tissue and prevention of vertebral body fracturing. Of utmost importance is the reduction of pain as well as the improvement of life quality.
The correct indication and choosing the correct therapeutic method are very important for the proper treatment of metastases of the spine. The correct therapy always has to be determined on a case-by-case basis, depending on different criteria and parameters (clinical, radiological, histopathological, etc.). The recognized score systems (such as, but not limited to Tokuhashi score, Karnofsky index and Tomita score) are helpful to determine for each case the type and extent of the method – palliative or radically chirurgical tumour resection and so on. 9,11,12
To optimize and improve the care of patients with multiple metastases and vertebral body destruction, our clinic successfully uses the recent and modern minimal invasive coblation/cavity method. So far, coblation has only been used in a relatively small number of cases, in particular in the United States, Japan and France. In Germany, this method has been used for the spine in very few clinics, occasionally also for arthroscopy and in otorhinolaryngology. 13,14 Not only does the removal of tumour tissue result in a cavity for cement, but all tumour cells are also destroyed and evaporated. Through the application of the plasma field, molecular bridges in the tumour are broken up, and the molecules start denaturation that leads to their transition to gas. 2,15 –17 The advantages are remarkable: through the creation of room, as well as the simultaneous coagulation and removal of the tumour using cold energy (locally around 42°C), the bone cement can be added without pressure. The risks of extravasation and tumour spread are decreased considerably. Other risks, especially blood loss and complications, are decreased and the operative times are considerably shorter. 18,19
The cavity/coblation method has significant advantages and differences to other long-established operational methods – vertebroplasty and kyphoplasty. In vertebroplasty, the cement usually leaks around the tumour and the tumour is not substantially made smaller. 20 In balloon kyphoplasty, 21 –23 the balloons create only a cave and the tumour cells are only pushed to the side, which increases the risk of tumour spread to blood vessels. Even in the radiofrequency kyphoplasty, 24 –27 the tumour is not removed and only deported by the bone cement to the side, where there is also the risk of tumour spread through the blood vessels. In both methods, there occurs no removal of the tumour tissue. 22,23,26 –28 In coblation, the controlled ablation is done with a prebent plasma probe. The tumour tissue is dissolved without thermal effect at very low temperatures through plasma field energy.
The purpose of this article and clinical trial was above all to examine and expand the value and the possibilities and limits of applying the percutaneous coblation/cavity method via plasma field followed by vertebro-/kyphoplasty to the spine. The second and very important task was to improve the therapy of tumours and metastasis of the spine through the combination of cavity/coblation with other procedures such as chemotherapy, radiation, additional dorsal minimal invasive percutaneous stabilization and straightening through the fixture of internal, open minimally invasive decompression. Included in this task is the improvement and optimization of the appropriate therapy scheme for specific clinical cases/disease patterns that are controlled by long-term results. Also here was developed and optimized the treatment strategy and treatment algorithm for optimizing the diagnosis, the treatment and control of operative and post-operative treatment. The short- and long-term results of these optimized therapies were planned, documented and evaluated in regular intervals.
Ultimately, this presentation is going to show the specifics of the method, the surgical technique, problematic, results as well as the effectiveness of the method, determining the limits of indication and the modernization of the method, based on the clinical study of 302 patients with 987 treated vertebral bodies with tumours and metastases at the spine.
Patients/material and methods
This study concerned male and female patients affected by spinal tumours – large symptomatically hemangiomas and spinal metastases with destructions/osteolysis as well as fractures with dangers of instability (proven through X-ray, computed tomography (CT)/MRI, F-18 full-body fluorodeoxyglucose positron emission tomography (F-18-FDG–PET), whole-body bone scintigraphy) and with a pain syndrome.
Preoperatively every patient underwent the following diagnostic, including tumour staging: clinical (including pain intensity documentation by the visual analogous scale (VAS)), radiological (X-ray in two layers, CT, MRI (obligatory), whole-body scintigraphy or F-18-FDG-PET, etc.) and histopathological (if possible preoperatively, especially at the known primary tumour otherwise intraoperatively for every patient), where the diagnosis of the tumour or metastases of the spine was saved both clinically and radiologically as well as histologically for every patient.
There is a pro- and retrospective clinical study, in which case some additional important innovations were introduced to the well-known ‘classic’ cavity/coblation method: additional performing of the kyphoplasty for fracture reduction, extraction or removal of the tumour remains from the vertebral body immediately after cavity/coblation under pressure, immediate local radiotherapy or irradiation, timely implementation of physiotherapy. Also here was developed and optimized the treatment strategy and treatment algorithm for optimizing the diagnosis, the treatment and control of operative and post-operative therapy. The short- and long-term results of these optimized therapies were planned, documented and evaluated in regular intervals.
The cavity/coblation method is approved for the treatment in Germany, United States and in several other countries. All patients were informed in accordance with standard length about the treatment methodology, treatment strategies, study course or therapy control intervals, data protection, possible complications and so on.
Description of cavity/coblation method
The Cavity Spine Wand/Probe (Figure 1) creates a free space in the vertebral body – cavity with the destruction of the tumour tissue through the creation of the plasma field (coblation-controlled ablation) at low temperature (approximately 42°C), through plasma-emitted high-frequency energy. Through the removal of tumour tissue, not only is a cavity created for filling with cement but also complete destruction/evaporation of the tumour cells can be achieved. The tumour cells are destroyed/evaporated as a result of the application of the plasma field to molecular bridges, which breaks up tumour tissue, leading to the denaturation of the molecule and consequently to a sublimation of the molecule to a gaseous state. The resulting benefits are considerable: through the creation of room and the simultaneous coagulation and removal of the tumour (local, approximately 42°C, cold energy), the cement can be inserted without pressure. The risks of extravasation, as well as tumour spread, are considerably minimized. Further operational risks, above all blood loss, complications and surgical times, are considerably reduced. 1,17,18,29 –31

Cavity unit: Cavity access trocar with attached Cavity Spine Wand/Probe and infusion line with the electrolyte NaCl. The bent tip of the Cavity Spine Wand leaves the tumour ablation perform in several directions. Cavity SpineWand has activated multiple active electrodes in order to create the plasma field, the ablation only happens in the forward motion, electrolyte solutions and slats such as NaCl are required to create the plasma field, the sonde is bent forward to create more room. NaCl: sodium chloride.
We have combined the method with balloon kyphoplasty 21,22,23 with custom-made extremely thin trocars to allow for fracture reposition and kyphosis reduction with the polymethylmethacrylate (PMMA)-bone cement application for vertebral stabilization and for filling the defect. The plasma probe is prebent and can be rotated, meaning the ablation was done in multiple directions under permanent control using X-ray in two projections during the surgery.
Operative technique cavity/coblation
The operation is performed in prone position. The entrance to one or multiple concerned vertebral bodies is created percutaneously trans- or extrapedicularly. An X-ray control, taken in two levels, is constantly performed during the entire operation.
Step 1: Inserting the custom cannula with a thread to get a better and a more stabilized grip. Extracting of biopsy material for microbiology and histopathology through a specialized biopsy cannula (Figure 2).
Step 2: Work with the Cavity Spine Wand in many directions, removal of the tumour with minimal blood loss because the blood vessels coagulate through plasma energy, creating a space devoid of tumour

Cavity tumour: OP-step 1: Inserting the special thin entry cannula/trocars with the thread (in order to have a better and more stable grip: transpedicularly or extra pedicularly).

Cavity tumour: OP-step 2: Working with the Cavity Spine Wand, removal of tumour, creating free room. Inserting the cement (prior to that the rests of the tumour and the NaCl solution is vacuumed through pressure through the cannula). The clinical trials show the effectiveness of the Cavity SpineWand: 2.5–3.5 qcm of tumour can be removed – cavity.

Cavity tumour: operation (OP)-step 3: The fracture reposition occurs, if necessary, prior to the balloon kyphoplasty. Then the stabilization of the vertebral body is carried by the PMMA-bone cement. PMMA: polymethylmethacrylate.
Note: At the low temperature of 42°C, usually no injury and necrosis of the bone tissue occur in the vertebral body. In this case only, the tumour tissue is removed. Even with the application of the bone cement, before it is hard to imagine the local temperatures above 70°C, which does not hurt the bone tissue developed, but vice versa – improves the composition between the bone cement and the bone tissue. In laser ablation, for example, yet developed much higher local temperatures – over 500–600°C, which of course is the injury/danger for the surrounding structures much larger. The plasma field can theoretically occur intraoperatively as injuries to nerves, blood vessels and internal organs. In order to avoid this, the X-ray control in two planes, frontal and sagittal of the probe position, is continuously carried out during the entire operation. In our study, however, no such violations are passed. Step 3: Insertion of the bone cement through pressure of the vacuum after the remainder of the tumour and the sodium chloride (NaCl) 0.9% solution have been removed through the cannula. Kyphoplasty allows for the expansion of room in the vertebral body as well as fracture reposition in case of fracturing (Figure 5).

The coblation effect: the Cavity Spine Wand moves and works only in forward direction. With a plasma field, induced tumour cells are decomposed into gaseous components.
Explanation
In the same surgical session, only one or two or more vertebrae can be effectively treated by cavity/coblation. For cavity/coblation, the NaCl 0.9% solution (physiological solution) was always used as the electrolyte. After the removal of the tumour tissue by coblation, the remains of the NaCl 0.9% solution with tumour residues were removed and sucked away from the vertebral body. After this was performed the baloon kyphoplasty using the PMMA -bone cement, which is always used in kyphoplasty.
Post-operative therapy controls
Post-operative results were controlled clinically and radiologically at regular time intervals (after 2, 14 days, after 3, 6, 12, 24, 36, 48 and 60 months), including questionnaires concerning the intensity of pain after VAS, the inhibition or improvement of life quality, the survival rate and so on. Particular attention was paid to tumour staging in order to exclude a local relapse or further metastasis.
Results
Treated patients and metastases species
Within 6 years (01.03.08–01.05.14). 302 patients (188 females and 114 males, age range of 31–92 years old, average age of 65.4 years) or 987 vertebral bodies with tumours or metastases were treated (Table 1).
Treated tumours and metastases of the spine during the clinical study.

Table 2 shows the distribution of patients with tumours/metastases with osteolysis/bone destruction and with/without pathological vertebral fractures. During one operative session either only one or two and several (up to 8) affected vertebrae were treated by the cavity/coblation in different patients.
Vertebrae/segments that were treated by cavity/coblation in one surgical session.

Operated vertebrae
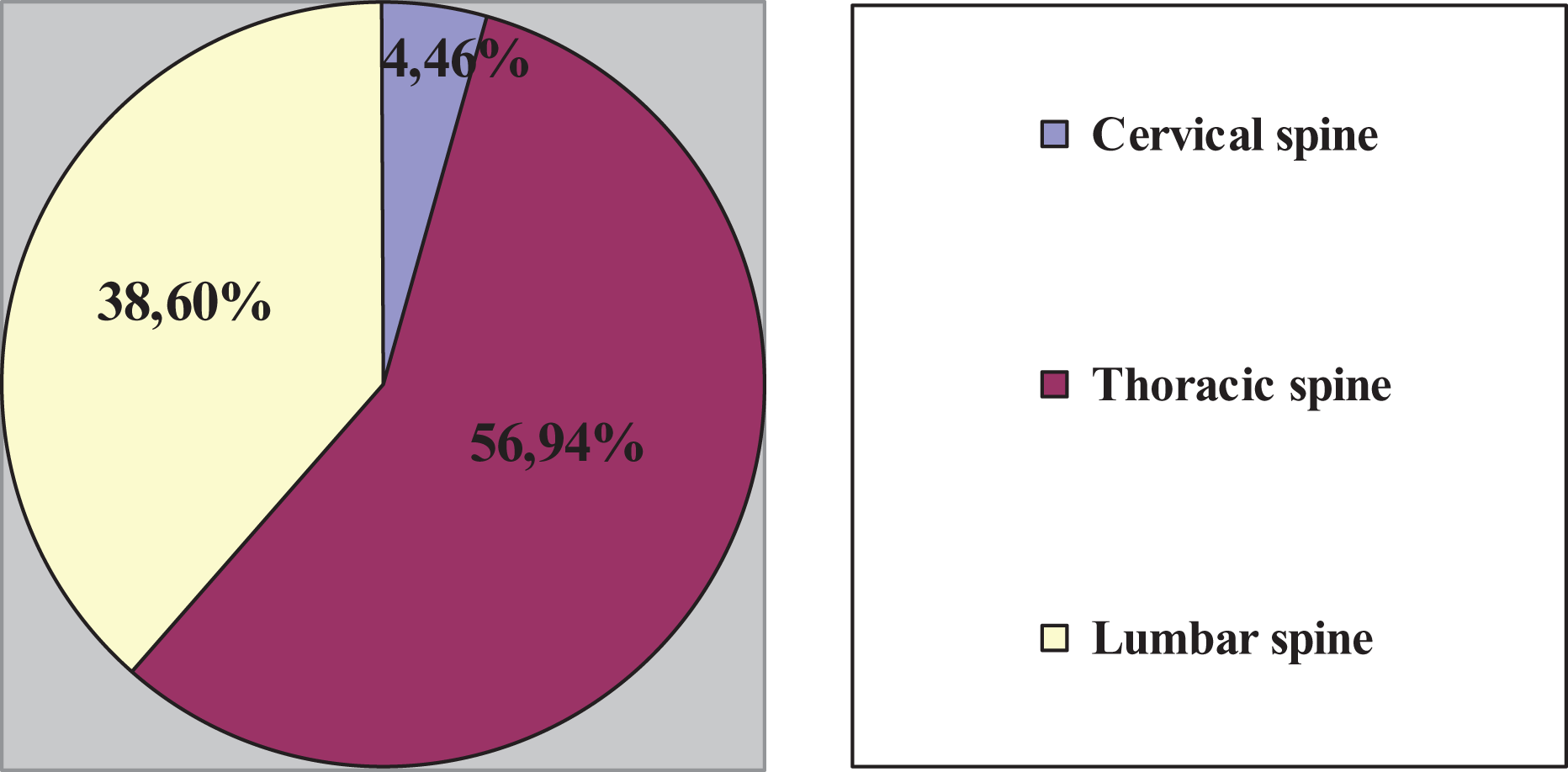
Total 44 vertebral bodies or 4.46% of all spine tumours/metastases were treated at the cervical spine, 562 vertebral bodies or 56.94% at the thoracic spine (Figure 6) and 381 vertebral bodies or 38.60% at the lumbar spine (Figures 7 and 8). Twelve patients were treated three times (at different vertebral bodies), 25 patients – two times (at different vertebral bodies) and 216 patients – one time at single or multiple vertebral bodies.

Clinical case 1, Pat. F., male, 52 years old, large hemangioma Th5 with microfracturing and massive pain syndrome, therapy resistant. Free from pain after the operation cavity/coblation with vertebroplasty.

Total number and spread of the vertebral bodies to be treated in the spine segments.
Percentage of the treated vertebral body in comparison to the spread in the spine segments.
It was taken the following distribution of patients into treatment groups according to the surgical procedures: Group 1: For 212 (70.2%) of all patients – only cavity/coblation with vertebroplasty/balloon kyphoplasty, percutaneously (Figure 6) was performed. Group 2: For 28 (9.27%) of all patients – the cavity/coblation with additional microsurgical decompression and hemi-laminectomy, respectively (in mini-open technique), tumourectomy and primary stabilization by the balloon kyphoplasty, all cases in the thoracic spine area. Group 3: For 62 (20.53%) of all patients, the cavity/coblation with additional dorsal percutaneous instrumentation with internal fixture over several segments (3 up to 8) was performed, to allow for stabilization and possibly straightening/correcting (especially for fractures with kyphosis and stenosis), done after the decompression and laminectomy, to avoid the sintering and further secondary deformations).
In the two And three Treatment cases/groups, the cavity/coblation was combined with microsurgical decompression and tumour removal. The blood loss through the previous coblation with coagulation and removal of tumour tissue was considerably less than for just the decompression and tumour removal (without cavity) (Table 3). Minimal invasive surgery was performed percutaneously using the dorsal instrumentation and very precisely using the X-ray-imager. It was controlled two times, respectively, using 3D navigation to place the screws precisely, which is especially important in cases of metastasis in the neighbouring vertebral bodies.
Comparison of the therapy methods of tumour metastases of the spine in the study: cavity alone, cavity with decompression, cavity with decompression and dorsal stabilization and with conventional open tumour surgery including vertebral body replacement and dorsal stabilization (based on the literature and our own clinical experience).

Using cursive will be the number of all clinical cases and all operations separately presented.
The results were controlled both clinically and radiologically 2, 14 days, 3, 6, 12, 24, 36, 48 and 60 months after the operation. Post-operatively no sintering or fixture-loosening/dislocation appeared. In all three groups, the results, especially for the local tumour relapse and the survival rate, were dependent exclusively on the number of metastases and extent of their spread and not on the operative method (e.g. additional percutaneous instrumentation).
Pain syndom rediction after the operation
The pain was reduced dramatically and resulted in high patient satisfaction and rapid life quality improvement of all patients. Preoperative pain related to the spinal tumours/metastases was determined through the VAS, differentiated for back pain as well as pain in the arms and legs in the case of spinal canal stenosis. Post-operatively, the pain was on average 6–8 VAS points lower, going from 7–10 point preoperatively to 0–3 point post-operatively.
Biopsy
All patients had samples (biopsies) taken intraoperatively from the affected/treated vertebral body, in order to be able to perform microbiological (MiBi, for exclusion of infections/spondylitis) and histopathological (histology, determination of tumour/metastasis type/source and primary tumour determination, tumour grading respectively) tests.
In 71 (23.5%) cases, diagnostics and operation were able to discover, define precisely and treat previously undiscovered primary tumours and metastases.
All patients were able to be mobilized rapidly after the operation, the blood loss was minimal and further treatment was usually initiated immediately.
The risk of hemangiomas of one or more segments with massive bleeding tendencies and risk of cement embolism was particularly decreased after the ablation and the coagulation of the tumour vessels through the plasma field.
Also for the treatment of plasmocytomas, in particular of large osteolysis and fractures, cavity/coblation followed by kyphoplasty showed very good results.
Complications
In 40 (by 40 vertebral bodies from 987 patients – only in 4.1%) cases, where large vertebral damage was present, small cement leakage laterally or in the intervertebral disc space was detected without clinical relevance.
Two hundred thirty-two patients (139 women and 93 men) have died as a result of tumour manifestations of the metastasis in the internal organs.
No local or generalized infection and no neurological deficits after surgery were recorded. We had observed no secondary kyphosis/deformity in our clinical study.
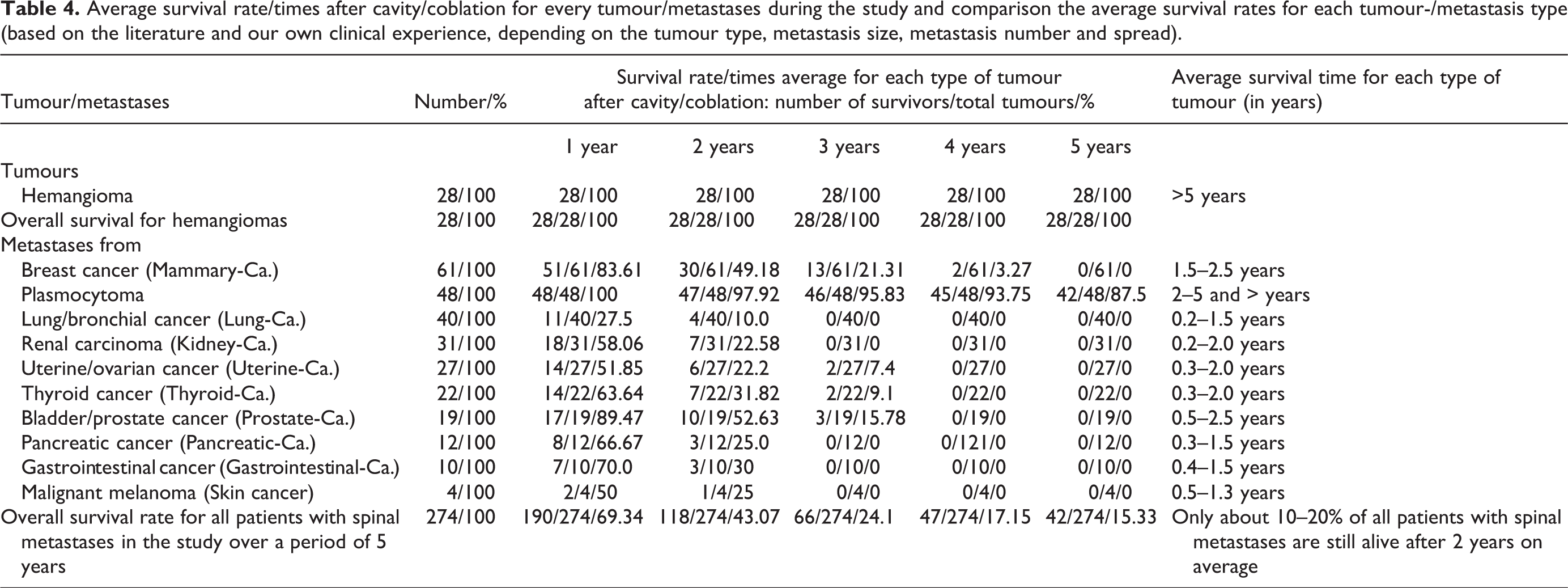
Nevertheless, the length of survival was increased independently of the type of tumour through the application of cavity/coblation with radiation and chemotherapy. The pain syndrome was significantly decreased and the quality of life was significantly better compared to the average results of palliative therapy without metastases-/tumour resection through cavity/coblation. 6 –9 Table 4 shows the result of survival rates and survival time after cavity/coblation for all hemangiomas and all metastases types in the study and the comparison of the average survival rates for each tumour-/metastasis type (according to the literature, depending on the tumour type, metastasis size, metastasis number and spread).
Average survival rate/times after cavity/coblation for every tumour/metastases during the study and comparison the average survival rates for each tumour-/metastasis type (based on the literature and our own clinical experience, depending on the tumour type, metastasis size, metastasis number and spread).
Local recurrence control post-operatively
Especially important was the control of the local findings to prevent the tumour recurrence at the treated vertebral bodies. In Table 5, the data concerning the therapy controls or rather the metastases-/local relapse controls are displayed.
Post-operative results for all tumours/metastases for local control/recurrence exclusion after cavity/coblation followed by local radiation therapy (maximum radiation dose 30–40 Gy) and chemotherapy of metastases.a

CT: computed tomography; MRI: magnetic resonance imaging; F-18-FDG-PET: F-18 full-body fluorodeoxyglucose positron emission tomography; –: no survival rate/no surviving patients with the respective tumour/metastases at this time.
aExamination methods are as follows: X-ray, CT, MRI, if needed (especially after instrumentations with existing implants with F-18-FDG-PET) or a whole-body skeletal scintigraphy.
Table 5 shows local relapse, which occurred in 13 of 61 cases or 21.3% of metastases of mammary carcinoma, in 2 of 48 cases or 4.2% of metastases of plasmocytoma, in 3 of 40 cases or 7.5% of metastases of lung carcinoma, in 7 of 31 cases or 22.6% of metastases of renal carcinoma, in 2 of 27 cases or 7.41% of metastases of uterine-/ovarian cancer, in 5 of 22 cases or 22.7% of metastases of thyroid cancer, in 3 of 19 cases or 15.8% of metastases of bladder-/prostate cancer and in 2 of 12 cases or 16.7% of metastases of pancreatic cancer. Altogether it concerns 37 of 274 cases with metastases or only 13.5% (another 28 were patients with hemangiomas – here are no local recurrences) of local relapse in 1 or 2 areas/vertebral bodies of extensive metastases of very aggressive, lowly differentiate tumours that only appeared 1 or 2 years after. The first 3 and 6 months usually passed without any local relapse. The local relapses were treated by locally aimed radiation therapy as well as chemotherapy.
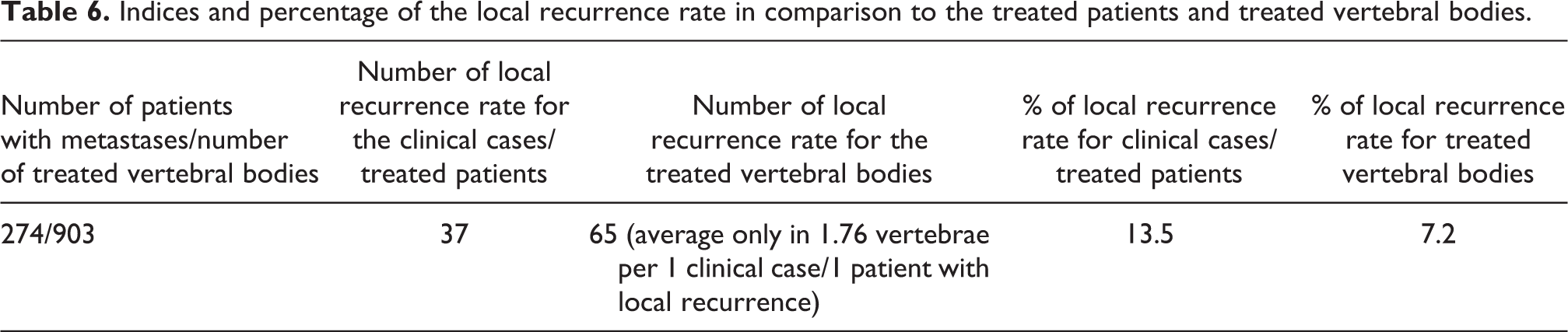
In Table 6 are presented the indices and percentage of the local recurrence rate in comparison to the treated patients (274 with metastases) and treated vertebral bodies (903 with metastases): only in 69 of 903 (or only in 7.64%) treated vertebral bodies – average only in 1.76 vertebral body per 1 patient with local recurrence. Local recurrences were successfully treated in all cases by the targeted local radiation therapy and chemotherapy.
Indices and percentage of the local recurrence rate in comparison to the treated patients and treated vertebral bodies.
Discussion and conclusion
When treating patients with tumours and metastases of the spine, it is vitally important not only to find the primary tumour and treat it but also to find and treat all possible metastases both loco-regionally as well as distant metastases. In many cases of radically extensive operative therapy, a metal fixture of titanium is used which, due to its size, creates many large artefacts that negatively impact the image quality of the CT and especially of the MRI. The implants of steel are furthermore a contraindication for the execution of the most important diagnostic tool for the local tumour search: the MRI and with the local relapse diagnostic. 6 –9,32 Here, and in many other cases, the F-18-FDG-GK-PET offers a successful replacement for patients with metastases of the spine, which was also used effectively in our study for the primary tumour staging, as well as for the relapse control (Figure 9). For the treatment of tumours/metastases of the spine, F-18-FDG-PET additionally offers a very valuable examination method to detect and localize metastases at the spine, in the skeletal system, as well as the lymph nodes, lungs brain, liver and other organs and tissues.

Clinical case 2. Pat. H., male, 56 years old, metastases with osteolyse from pancreas cancer, at the beginning only in the C7, preoperatively: F-18-FDG-whole-body-PET, MRI, CT. PET: positron emission tomography; MRI: magnetic resonance imaging; CT: computed tomography.
Other known traditional treatment methods show considerable disadvantages or side effects. Cryotherapy, for example, performed at very low temperatures, is very labour intensive, a complete metastases removal is predominantly impossible and there is a substantial risk of damaging healthy tissue. 1,2 Laser therapy occurs at higher temperatures locally with 500–600°C. Among other dangers, it risks damaging healthy tissue. 2,4 The radiohighfrequency method, 2,3,5,6,9 for example, with the Rita Starburst MRI device, works with radiohighfrequency and also generates a high temperature (more than 400°C) to destroy tumour cells. However, a complete destruction of the tumour/metastases is barely possible and healthy tissues including vessels and nerves are at risk. For several years, the known method of kyphoplasty in combination with the intraoperative radiotherapy is according to the first results and publications, promising but is very complicated, expensive and can be performed only in large centers with special equipment for radiotherapy. 33,38
The percutaneous cavity/coblation method offers patients with tumours/metastases of the spine of higher operative risk, a relatively safe, minimally invasive and minimally traumatic procedure, which is confirmed by short-term as well as long-term results. Through the percutaneous minimal invasive access, the operative risk, in particular, blood loss, as well as surgical times were reduced. Other important qualities are the rapid post-operative pain reduction and stability. 2,3,6,10,16 –18 Parallel to the vertebral metastases also metastases in other skeletal parts can be successfully treated by the cavity/coblation method (Figures 10 –12).

Clinical case 2. Pat. H., male, 56 years old, new metastases with osteolyse from pancreas cancer in C4 (C7 after surgery – here no tumour recurrence in 3 months post-operatively), in the TH10, L1, L5, left femoral head (in the PET), preoperatively: F-18-FDG-PET (whole-bodyPET), MRI, CT. PET: positron emission tomography; MRI: magnetic resonance imaging; CT: computed tomography.

Clinical case 2. Pat. H, male, 56 years old, metastases with osteolyse from pancreas cancer in the TH10, L1, L5, left femoral head, preoperatively MRI, CT. MRI: magnetic resonance imaging; CT: computed tomography.
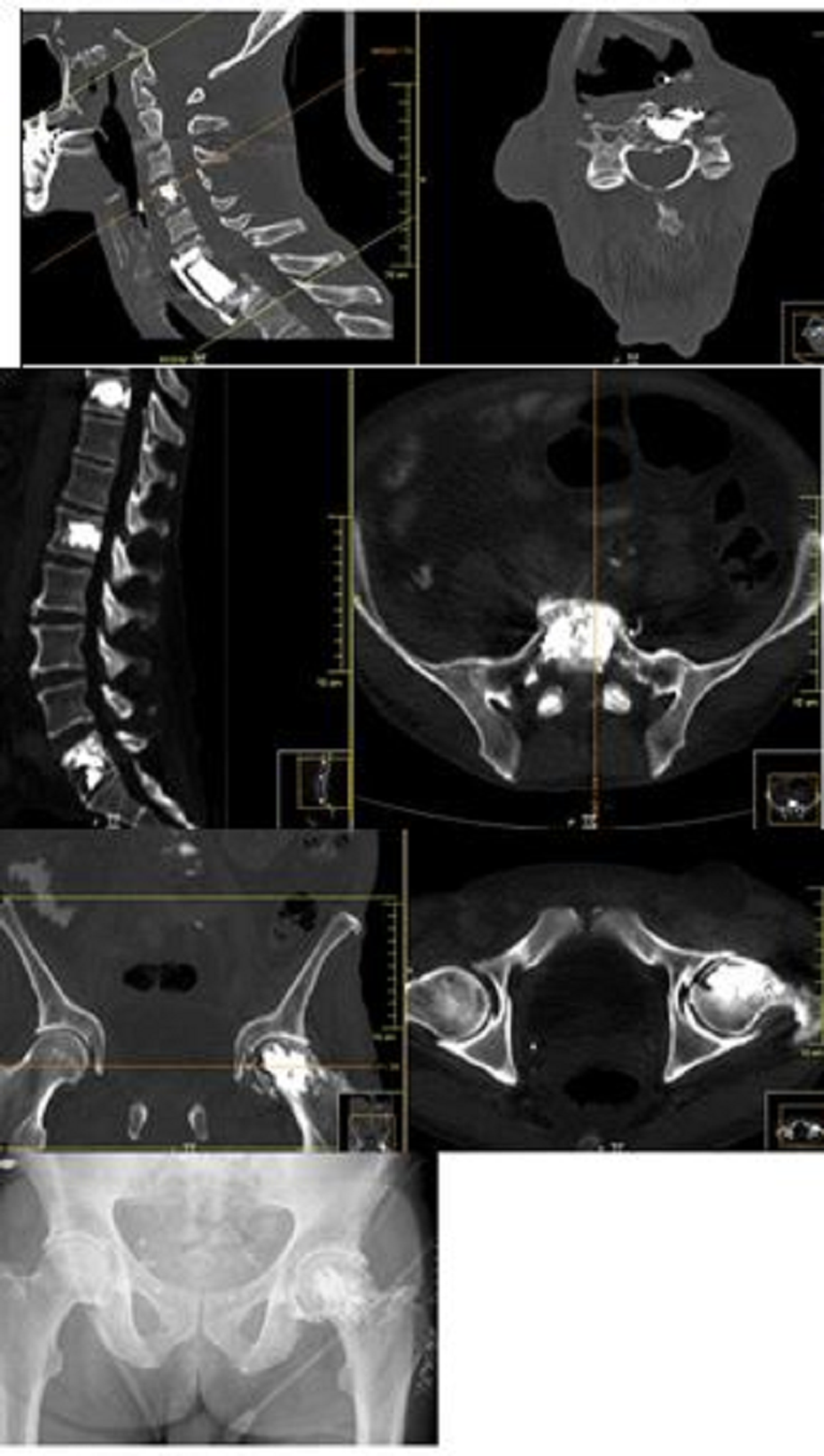
Clinical case 2, Pat. H, male, 56 years Old, 9 months post-operatively after the tumorectomy of the C7 with C7 vertebral body cage replacement and internal fixation with screws and plate from ventral C6-Th1, 6 months after the cavity in C4, Th10, L1, L5 and left hip head. Post-operatively: chemotherapy and local radiation therapy, significant reduction of pain syndrome, restoring stability. CT control after 6 months post-operatively: no local relapse. CT: computed tomography.
So far, clinical studies on cavity/coblation have been carried out and published especially in the United States, Japan and France with relatively small sample size, whereby multiple authors have confirmed the effectiveness of the method. 13 –19
In this study, the already known ‘classic’ cavity/coblation method has been modernized and completed:
1
–3,6,16
–19
Through the combination of cavity/coblation with balloon kyphoplasty
21
–23
with special super thin balloons/trocar, fracture repositioning and kyphosis correction in one or multiple segments, also at the thoracic and at the cervical spine, remain possible. After the destruction of the tumour or after the cavity/coblation, the remains of the tumour are removed through pressurized vacuum that decreases the relapse danger considerably. The cavity/coblation method in the sample patient group was combined post-operatively with local radiation as well as chemotherapy. Particularly important is an obligatory treatment (surgery, radiation, chemotherapy) of the primary tumour and of all metastases. Since cavity does not create large wounds (even when multiple segments are being targeted), the radiation could begin practically immediately or few days after the operation. In comparison, extensive operations create large wounds that allow radiation and chemotherapy only after many weeks due to the high risk of wound healing disturbance.
6
–9,31,32
The low intraoperative temperatures (only approximately 42°C, with plasma-cold energy) mean the healthy structures/organs/bones are not damaged, which considerably improves the reparatory process in lesion areas. Cavity/coblation was combined in our clinical study in cases of spinal stenosis with the microsurgical decompression that resulted in minimized blood loss.
An interdisciplinary setting or cooperation of spinal surgery with other disciplines, with radiotherapy, oncology, radiology and pathology, is of utmost importance. It is not uncommon that, for the affected patients, the primary tumour is unknown and through diagnostics, according to oncological-chirurgical guidelines at multiple localizations, a biopsy has to be carried out in order to start a targeted, suitable tumour therapy. 6 –9,32
Problematic/particularities
The treatment of tumours and metastases of the spine is a challenge. Of utmost importance is the interdisciplinary collaboration. Depending on bone stability, compression of the neural structures, radiosensitivity of the tumour tissue, the pain symptomatic and, last but not least, the overall prognosis, an individually adjusted therapy of the spine metastases has to be planned. 6 –9,11,12,32
The proper indication and choice of the appropriate treatment method are crucial for the treatment of the metastases of the spine. The right therapy has to be always determined on a case-by-case basis, depending on certain criteria and parameters (clinical, radiological, histopathological, etc.). The known score systems (Tokuhashi score, Karnofsky index, Tomita score, etc.) are helpful in deciding which method and to what extent (palliative or rather radical chirurgical tumour resection, etc.) is best suited for every individual case. Since it is a palliative method in a variety of patients, for example, for multimorbid patients, especially with multilocular tumour manifestations/metastases in the skeleton units or vertebral body, while likely to seek a comprehensive surgical complete resection, often a therapeutic approach is required for solitary metastases. These different score systems, which are used to determine the treatment prognosis and survival prognosis, have limited diagnostic significance and can only be used as pointers. 7 –9,11,12,32
In many cases, it is not possible to remove the tumour tissue completely, which explains why directly after operation a post-operative radiation has to be carried out. An exclusively local radiation (in general, maximum total dose of 30–40 Gy) without previous operative removal of the tumour tissue does not completely remove the tumour, in particular for large osteolysis in several vertebrae with a circumference of more than 2–3 cm. The local radiation dose has to be increased considerably, which can cause damage to the skin, subcutaneous tissue, muscle tissue as well as blood vessels and nerves. 9,34 –37 For multimorbid oncological patients with poor prognosis, in particular with large osteolysis or pathological fractures in the spinal area and with a massive drug-resistant pain syndrome of the spine, for whom until recently no adequate therapy (especially surgical) was available and who, due to practical immobility, died rapidly of various comorbidities (pneumonia, embolism, heart- and circulatory failure, depression), cavity/coblation offers an opportunity to attain a certain degree of mobility including capacity und ability to walk. This, as well as the resultant reduced pain symptoms, improves the quality of life noticeably. What is most important – now can these critically ill patients spend those remaining time – the last days, weeks and months active, pain-free and fully mobile home with their families and not in the hospital.
Like any other method coblation/cavity has its limits and indication restrictions. Those are, in particular, large extensive metastases with destruction of one or multiple vertebral bodies. For optimum metastases treatment, it is necessary that within the vertebral body with a tumour metastasis, all six or at least four vertebral walls for the optimum support of the bone cement still exist.
Additionally, the method has a steep learning curve. The extent of the operation and the indication have to be checked necessarily and adjusted very precisely and accurately for every patient and every case. Also important is a precise surgical technique, where the primary goal is a highly precise metastases removal.
The cavity/coblation method for the treatment of multiple metastases to the spine combined with kyphoplasty, chemotherapy and local radiation therapy immediately after surgery is a safe minimally invasive procedure, which has been with us evidenced by the short- and long-term results. The effectiveness of the cavity method is confirmed by the numerous clinical studies and examples from other colleagues. The surgical risks of blood loss and surgical times are significantly lower and shorter, and the complications rates are minimal. It is always important to consider an extensive diagnostic inclusive tumour staging, proper indication and prognosis determination as well as precise surgical technique. In our opinion, the method shows much promise for the future.
Practical conclusions for the treatment of the spine metastases
When treating patients with metastases of the spine, the following things have to be always considered: Extensive preoperative diagnostic – clinically, radiologically including tumour staging, if possible also histological. The extent of the operation and indication has to be planned, checked and submitted very precisely for each patient individually. Tight collaboration between the orthopaedists/spine surgeons with other specialists: with radiologists/nuclear physicians, radiotherapist, oncologists, histopathologists, pain therapists, physiotherapists and so on. A precise operative technique where the goal is a complete tumour tissue removal and stability. Immediate post-operative execution of local radiation and chemotherapy, the primary tumour and other metastases always have to be treated as well. Regular checkups – clinically and radiologically (to exclude local relapse, loosening, fractures, evaluation of state, satisfaction, life quality, pain reduction, etc.). Very important – proper indications, patient choice, sober prognosis assessment.
The cavity/coblation is a particularly gentle minimally invasive surgical method without or with only minimal traumatization of the soft tissues and bone/vertebrae. No local or generalized infection, no neurological deficits, no secondary kyphosis/deformity after surgery were recorded in our clinical study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.