
Abstract
Purpose:
Sternoclavicular joint is an amphiarthrodial joint formed by the clavicle and sternal manubrium. This joint becomes chronically unstable in case of a medial clavicle dislocation or fracture, and improper treatment could cause malformation and pain. We aimed to determine the efficacy of a novel sternoclavicular hook plate for treatment of unstable sternoclavicular joint dislocation or fracture.
Methods:
Between June 2011 and December 2013, the sternoclavicular hook plate was used to surgically treat 32 adult patients with unstable sternoclavicular joint dislocation or fracture. Of these, 12 and 5 patients suffered from anterior and posterior dislocation of the sternoclavicular joint, respectively, 10 had medial clavicle fracture, and 5 had fracture dislocation. For anterior fracture dislocation, the standard sternoclavicular hook plate was used, while for the posterior dislocation, screws were added at the distal end of the hook plate, anterior to the sternal manubrium, to prevent postoperative redislocation.
Results:
No intraoperative complications were observed during the procedure. Postoperative X-ray and computed tomography revealed normal anatomical positions of sternoclavicular joints and excellent positions of internal fixation. About 3–6 months after surgery, all patients achieved primary healing without redislocation of the sternoclavicular joint along with satisfactory restoration of anatomical structures of the medial clavicle; nine patients had swelling but no pain around the sternoclavicular joints. Internal fixation was removed in 29 patients 6–12 months postoperatively and no sequelae were observed.
Conclusion:
This novel sternoclavicular hook plate demonstrated excellent efficacy and could provide a reliable therapeutic approach for this kind of trauma.
Introduction
The incidence of sternoclavicular dislocation is low, accounting for less than 5% of shoulder girdle injuries 1 and about 1% of scapulothoracic dislocations, 2 while the incidence of medial clavicle fracture accounts for only 5–6% of the clavicle fractures. 3 However, its incidence rate is increasing with the increase in traffic accidents. Osteoarticular injuries around the sternoclavicular dislocation are mainly caused by high-energy damages and are frequently complicated with multiple traumas, leading to the possibility of a missed diagnosis. Since important tissues such as the mediastinum and trachea are located posteriorly to the sternoclavicular joint, surgical treatment carries a risk of sternoclavicular dislocation; in addition, choosing the optimal therapeutic option is controversial.
Conservative treatments include manipulative reduction and limb immobilization; however, maintaining position after fracture dislocation is difficult, and long-term immobilization could severely affect the quality of life of the patient. Surgical treatments include Kirschner wire fixation, plate fixation, ligament reconstruction around the sternoclavicular joint, and medial clavicle resection; 4 –7 thus far, no standardized surgical pattern or internal fixation device has been developed. Several surgical approaches carry a risk of multiple complications. For example, patients who undergo Kirschner wire fixation may suffer from serious complications such as blood vessel and vital organ injuries following pin breakage or displacement. 8,9 Application of a T-shaped plate that fixates the clavicle and sternal manubrium by screw sacrifices the amphiarthrodial function of the sternoclavicular joint. 10,11
These serious complications and disadvantages of the internal fixation materials have shown the crucial importance of the assessment and appropriate selection of therapeutic approaches for this type of trauma. In this study, we designed and utilized a novel sternoclavicular hook plate to restore and fixate the unstable sternoclavicular joint dislocation; in addition, we retrieved the related literatures and compared our method with other internal fixations, in order to provide a better therapeutic regimen.
Methods
General data
Based on the anatomical characteristics of the human sternoclavicular joint, we designed an anatomical sternoclavicular hook plate and ancillary equipment (patent nos. ZL2003201079412 and ZL201220667654.6); the plate hook was inserted from the posterior upper edge of the sternal manubrium to hook the sternums and the plate body was placed at the anterior edge of the medial clavicle, fixated by the screws (Figure 1). The intraoperative manipulation is convenient and safe and can easily accomplish the reduction of fracture dislocation; one end of the plate is fixated by the screws and the other end is hooked into the sternal manubrium, that is, the plate is dynamically fixated, which can maintain a certain activity function of the sternoclavicular joint. The plate is manufactured by Zhejiang Canwell Medical Co., Ltd. (China). It is divided into two parts: left and right; two models of the hook measuring 21 mm and 24 mm in height are available. There are screw threads at the end of the hook, accompanied by matching nut and washer, which is used for fixation of the posterior dislocation of the sternoclavicular joint.

Morphology of the plate, nut, and washer.
The study was approved by the ethics committee of Taizhou Hospital of Zhejiang Province. All participants have provided informed consents. Between June 2011 and December 2013, 32 patients were admitted and surgically treated for fracture dislocation at our hospital. Patients whose plain computed tomography (CT) image indicated an anterior or posterior clavicle dislocation that exceeded more than half of the joint surface, those whose physical examination showed obvious focal uneven surface and unusual activities, those in whom stable alignment could not be maintained by manipulative reduction, and those with comminuted lesions or oblique fractures of the medial clavicle were included in the study. There were 24 male and 8 female patients with a mean age of 42 years; 12 patients suffered from anterior dislocation of the sternoclavicular joint, 5 had posterior dislocation of the sternoclavicular joint, 10 had medial clavicle fracture, and 5 had fracture dislocations, 2 of which were old dislocations (more than 3 weeks old). For the anterior fracture dislocation of the sternoclavicular joint, the standard sternoclavicular hook plate was used, and for the posterior dislocation, screws and washers were added anterior to the sternal manubrium in order to prevent postoperative redislocation (Figure 2).

Position where the plate is placed in the human skeleton sample, with nuts and washers used in posterior clavicle dislocation and nuts spared in anterior dislocation.
Surgical procedure
Surgeries were performed under intubation anesthesia or unilateral cervical plexus anesthesia + local anesthesia; an S-shaped incision measuring 8–10 cm was made along the midline of manubrium, via the sternoclavicular joint, and to the anterior edge of the clavicle; the sternal manubrium, sternoclavicular joint, and proximal clavicle were exposed and the long and bent nerve dissector was closely adhered to the sternum to dissect the soft tissues of the posterior sternal manubrium after stripping the upper edge. A specially made drill jig (containing a sleeve to protect the posterior sternum, manufactured by Zhejiang Canwell Medical Co., Ltd., part of the patent) was placed from above the sternal manubrium to drill at the midline of the manubrium and about 1.2 cm from the upper edge; there was a barrier sheet in the drill jig located at the posterior sternal manubrium to prevent the drill from damaging the important tissues of the posterior sternum. The hook end was inserted from the posterior sternum into the bone foramen and the other end was adhered to the anterolateral clavicle to perform the reduction based on the fracture dislocation mechanism. The plate was then fixated to the clavicle by the screws while washers and nuts were added at the threads of the hook end for patients with posterior dislocation (Figure 3).
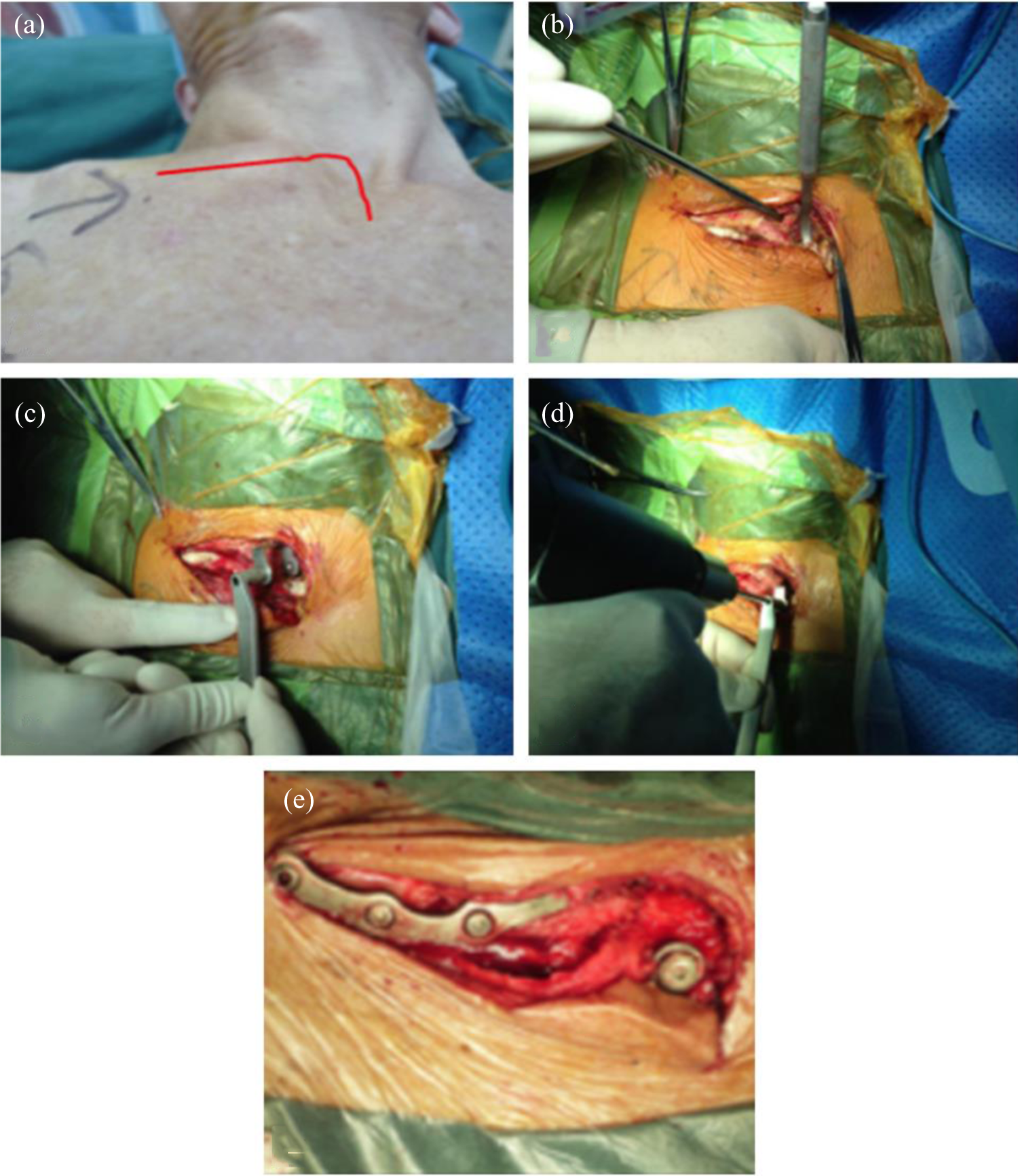
(a) Anterior dislocation of the right sternoclavicular joint with a 7-shaped incision; (b) soft tissue of the upper edge of the sternal manubrium is stripped by a dissector; (c) a specially made drill jig is inserted from above the sternal manubrium; (d) there is a barrier sheet at the posterior drill jig, which avoids damages to the important tissues located at the posterior sternal manubrium during the drilling; and (e) washers and nuts should be used during a posterior dislocation of the sternoclavicular joint to prevent postoperative redislocation.
Postoperative management
A drainage rubber was placed into the incision and the layered suture was performed. Immediately after the surgery, patients were asked to start functional exercises of the affected limb, such as pendulum-like movements, active and passive flexion, and uplifting movements; patients could resume their daily activities and work 3 months postoperatively. The sternoclavicular hook plate could typically be removed 6–12 months postoperatively when the fracture line disappeared and healed.
Evaluation indices
The clinical efficacy of this procedure was assessed using the Rockwood scale 6 months postoperatively. 10 According to this scale, 3 points indicated no pain, 2 points indicated mild pain, 1 point indicated moderate pain, and 0 point indicated severe pain. With regard to the range of movement, 3 points indicated normal movement, 2 points indicated mildly restricted (<25%) movement, 1 point indicated moderately restricted (25–50%) movement, and 0 point indicated severely restricted (>50%) movement. With regard to muscle strength, 3 points indicated normal strength, 2 points indicated mildly reduced (<25%) strength, 1 point indicated moderately reduced (25–50%) strength, and 0 point indicated severely reduced (>50%) strength. With regard to the limitation in daily activities, 3 points indicated no limitation, 2 points indicated mild limitation, 1 point indicated moderate limitation, and 0 point indicated severe limitation. With regard to the subjective outcome, 3 points indicated an excellent outcome, 2 points indicated a good outcome, 1 point indicated a fair outcome, and 0 point indicated a poor outcome. A total score of 13–15 points indicated an excellent outcome, 10–12 points indicated a good outcome, 7–9 points indicated a fair outcome, and <7 points indicated a poor outcome.
Results
No intraoperative complications such as neurological, vascular, or tracheal damages were observed in any patient. Postoperative X-ray and CT reexaminations showed normal anatomical position of the sternoclavicular joint and excellent position of the internal fixation in patients with dislocation fracture (Figures 4 and 5). All 32 patients were followed up, with a mean duration of follow-up of 10 (range, 6–24) months. Primary healing was achieved 3–6 months postoperatively in all the patients, without re-dislocation of the sternoclavicular joint, and anatomical structures of the medial clavicle were restored with satisfactory functions; nine patients had swelling but no other symptoms such as pain around the sternoclavicular joints. Internal fixation was removed in 29 patients 6–12 months postoperatively and no sequelae were observed. The follow-up of three patients was delayed because of noncompliance and was conducted 1.5–2 years postoperatively. Physical examination at follow-up revealed a protruded bulging deformity at the upper sternal manubrium, while CT reexamination showed obvious callus proliferation around the sternal border; bone foramen at the hook end was enlarged, with bone resorption (Figure 6). However, their sternoclavicular joint was well matched and the pain was not significant; all three patients were aged above 55 years and worked as farmers. According to the Rockwood scale, 24 patients were excellent and 8 patients were good.

X-ray and CT image of a 24-year-old male patient suffering from posterior dislocation of the right sternoclavicular joint preoperatively, which was restored to normal 2 years postoperatively.
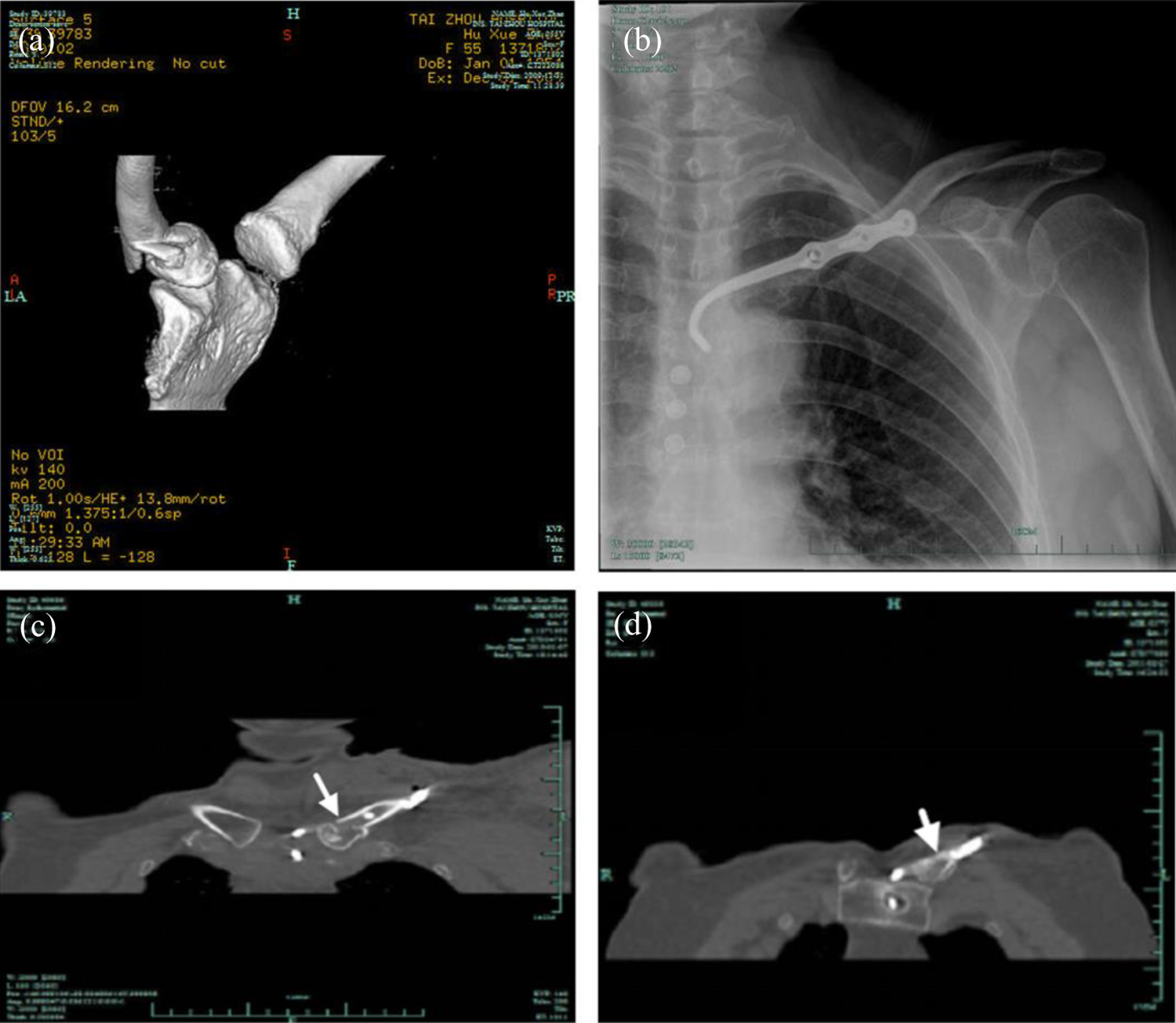
(a) Preoperative CT image of a fracture of the left medial clavicle in a 56-year-old female patient; (b) postoperative X-ray shows a tendency of clavicle anterior displacement; no washer or nut is used in the anterior hook plate; (c) postoperative CT image shows excellent fracture alignment; and (d) CT performed 1 year postoperatively before internal fixation removal shows fracture union.

(a) Preoperative CT image of posterior dislocation of the right sternoclavicular joint in a 24-year-old male patient and (b) 2 years postoperatively, bone resorption and proliferation appear around the hook at the sternal foramen but no nut and washer loosening occur at the anterior hook (white arrow) and the sternoclavicular joint is excellently aligned.
Discussion
Sternoclavicular joint dislocation is a rare injury, which includes anterior and posterior dislocation. Anterior dislocation is more commonly observed while patients with posterior dislocation are at a greater risk. Fracture of the medial clavicle accounts for only 5–6% of all clavicle fractures.
Sternoclavicular dislocation is correlated with its specific anatomical structure: The proximal segment of the clavicle bulges, while the clavicular notch of the sternal manubrium is small and shallow; thus, sternoclavicular stability is mainly maintained by the complex and firm ligaments around the joints. There are many important intramediastinal thoracic structures, including the esophagus, trachea, intrathoracic great vessels, and the recurrent laryngeal nerve, located posteriorly to the sternoclavicular joint, which is also the anatomical basis of susceptibility to injuries in posterior sternoclavicular dislocation and during sternoclavicular joint surgeries. 12
Thus far, there has been no widely recognized gold standard for the treatment of sternoclavicular dislocation and displaced fracture of the medial clavicle. Although it has been reported that closed reduction can be the final therapeutic regimen for 38% of patients with such lesions, 13 conservative treatment shows poor efficacy in patients with sternoclavicular joint dislocation; these patients develop progressive pain of the sternoclavicular joint, limiting the movement of the affected shoulder girdle and decreasing their quality of life. 4 While there are other reported surgical treatments including Kirschner wire or plate fixation, medial clavicle resection, costoclavicular ligament reconstruction, 3-point anchor suture, and sternoclavicular joint reconstruction with the palmaris longus or allograft tendon, 4 –7 in all these surgeries, either the amphiarthrodial function of the sternoclavicular joint is sacrificed to achieve firm fixation, or postoperative complications such as internal fixation displacement, reduction loss, and infections are usually observed because of the complex surgical manipulation. Thus far, there has been no well-recognized internal fixation equipment suitable for all sternoclavicular dislocation and medial clavicle fractures.
Since 2002, we have designed the anatomical sternoclavicular hook plate and developed sets of dedicated surgical tools based on three-dimensional CT images and fresh cadaveric models and obtained excellent efficacy in the long-term clinical application. Some advantages of this plate are as follows: (1) the plate is in line with the anatomy of the sternoclavicular joint; (2) the operation is easy and safe; (3) the dynamic fixation of the plate enables micromotion of the sternoclavicular joint within a certain range, consequently minimizing the possibility of internal fixation breakage or displacement; and (4) it can be applied to patients with anterior/posterior dislocation of the sternoclavicular joint or medial clavicle fracture and old sternoclavicular dislocation. Because posterior dislocation of the sternoclavicular joint is extremely unstable and risky and owing to the lack of a suitable implant fixation method, our hook plate is especially advantageous for the treatment of patients with sternoclavicular joint dislocation.
During the operative procedure, attention should be paid to the following aspects: (1) a long and bent nerve dissector should be adopted to dissect the soft tissues of the posterior sternal manubrium after stripping the upper edge so as to prevent damages to the posterior veins and lymphatic vessels; (2) important tissues such as the mediastinum and pleura are located posteriorly to the proximal sternum and clavicle and can be easily injured during the drilling; however, our specially made drill jig can avoid excessive drilling and damages to the important tissues; and (3) based on the injury mechanisms, a nut fixation is unnecessary at the hook end of the plate if there is a tendency of anterior displacement of the medial clavicle, while a nut fixation to fixate the hook end (viz. the anterior sternal manubrium) to prevent the posterior displacement is necessary if there is a tendency of posterior displacement of the medial clavicle.
In the present study, three patients delayed their follow-up visits and visited 1.5–2 years postoperatively presenting of a focal bulge. CT examinations revealed a bony proliferation around the hook area of the lower sternum edge; however, no internal fixation breakage was observed and the sternoclavicular joint appeared normal, indicating that the structural design of the novel sternoclavicular hook plate was reasonable. However, since micromotion of the sternoclavicular joint exists during upper limb movements and the hook moves along with the sternal manubrium, the sternoclavicular hook plate should be cautiously applied for patients with severe osteoporosis; stimulating discomforts at the implant hook end may occur during delayed fixation removal. Therefore, we recommend prompt implant removal (about 6 months postoperatively, after assessing the bone and joint union) in elderly patients, in order to avoid complications caused by implant failures.
Conclusions
This novel sternoclavicular hook plate shows excellent efficacy for the treatment of unstable sternoclavicular joint dislocations. This implant fixation is solid, reliable, safe, and easy to operate, providing a reliable therapeutic method for this type of trauma. However, since fracture dislocation of the sternoclavicular joint is a rare lesion and the sample size of the current study is small, further multicenter studies with large sample sizes are warranted to support our findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.