
Abstract
Background:
Frozen shoulder is not an uncommon disorder, and steroid injection into the glenohumeral (GH) joint is one of the most well-known approaches for the frozen shoulder. However, their results have been varied with beneficial effects or no additional advantage. With the understanding about the pathological changes taking place in frozen shoulder and the biomechanics involved, we wanted to evaluate the short- and long-term efficacy of steroid injection by a novel three-site (NTS) injection technique and compare it with the single-site injection (SSI).
Material and methods:
This was a prospective study with 85 patients including all stages and randomized into two groups. SSI group received steroid injection through posterior approach. NTS group received the same dose of steroid in diluted doses at three sites (posterior capsule, subacromial and subcoracoid). Second sitting was repeated after 3 weeks. Both groups had received the same physiotherapy. The patients were evaluated by CONSTANT score at initial, 3 week, 6 week and 6 month.
Results:
NTS group patients had significant pain relief and early improvement in activities of daily living (p < 0.005). Both groups had improvement in shoulder movements but with NTS group, early near-normal scores were attained and sustained after 6 months. About 43% in SSI group could not attain near-normal levels and had relapses.
Conclusion:
The three-site approach to steroid instillation in frozen shoulder is a safe method and provides early recovery and better improvement in shoulder function with less relapses.
Background
Frozen shoulder or the adhesive capsulitis of the shoulder is not an uncommon disorder characterized by a significant reduction of active and passive range of motion of the glenohumeral (GH) joint along with pain. 1 Although self-limiting, it can be extremely painful and debilitating affecting the activities of daily living 2 and there may not be complete resolution of symptoms in a vast number of cases. 3 Various treatment modalities include benign neglect, 4 oral nonsteroidal anti-inflammatory drugs (NSAIDs), 5 oral corticosteroids, 6 GH intraarticular corticosteroid injections, 7 interventional microadhesiolysis 8 and various physical therapies, 9,10 operative interventions like manipulation under anesthesia 11 or supraclavicular blocks, 12 arthroscopic capsular release 13 or hydrodialation 14 and open surgical release. 15 Non-surgical interventions still are the mainstay of treatment and operative reserved for only refractive cases. 16
Regardless of the aetiology, steroid injection into the GH joint together with therapeutic shoulder exercises is one of the most well-known approaches for the frozen shoulder known for their additive effect. 7 However, their results have been varied with beneficial effects 17 or no additional advantages. 18 Some of the known attributable causes of low efficacy are a low accuracy of injection into the GH joint without radiologic guidance, 19 dosage, 20 number of injections 21 and pathological process occurring at different sites. 22 With the understanding about the pathological changes 22,23 taking place in frozen shoulder and the biomechanics 24 involved, the authors wanted to evaluate the short- and long-term efficacy of steroid injection by a novel three-site (NTS) injection technique (posterior capsule, subacromial and subcoracoid) and compare it with the traditional single-site injection (SSI).The hypothesis being that the NTS injection technique would have better outcomes than the other.
Materials and methods
This was a prospective randomized comparative study done between September 2012 and March 2015 comparing the instillation of steroids in primary frozen shoulder through the traditional single site posteriorly and an NTS injection technique. Patients presenting with pain and restricted shoulder movements and fulfilling the Codman criteria were evaluated with X-ray, ultrasound, magnetic resonance imaging of shoulder to rule out secondary causes like rotator cuff tendinosis, biceps tendinitis, calcification tendinosis and so on.
Patients beyond age 68 and below 40, unwillingness and inability to comply shoulder physiotherapy and other invasive procedures, uncontrolled diabetes, deranged thyroid functions, associated shoulder disorders, patients under other serious medical illness, undertaking steroids, and immunosuppression were excluded from the study. Patients were also classified by their clinical staging into freezing, frozen and thawing phases and the randomized by adding subsequent patients into one of the groups (Figure 1).

Consort flow chart of events in the study.
Treatment procedure
Eighty-five patients were included and randomized into two groups, 43 in SSI group and 42 in NTS group. All patients prior to injection were subjected oral NSAIDS, supervised physiotherapy by trained physiotherapist, ultrasonic therapy and home exercises (wall creeping, cart wheel and towel exercises) for period of 4 weeks. Two sittings were given without radiological assistance in both groups separated by a gap of 3 weeks. Short-term improvements noted and re-evaluated after 6 months for long-term sequel.
Method of injection
In the SSI group, a single injection of 40 mg of methyl prednisolone acetate mixed with 2 ml of 2% lignocaine was prepared and instilled through the posterior approach (2 cm below and lateral to angle of acromion directed towards coracoid).
In NTS group, the same solution was further diluted with 8 ml normal saline and instilled at three sites. Posterior site injection was given 2 cm below and lateral to angle of acromion directed towards coracoid. During the steroid injection the arm was gradually abducted for instillation of steroids into axillary recess.
Subacromial site was attained by running the 16G IV needle above spine directed towards acromioclavicular joint through supraspinatus muscle and gradually internal rotating during instillation.
Subcoracoid site was obtained by running the needle on subscapularis surface 0.5–1 cm inferior and lateral to coracoid passing towards the lateral third of coracoid, arm externally rotated during instillation of steroid.
The initial baseline and subsequent outcome measures during follow-up at 3, 6 weeks and 6 month were done using CONSTANT score technique (pain, activities of daily living, flexion, extension, internal and external rotation, and strength).
Statistical analysis
Categorical variables were presented in number and percentage (%) and continuous variables were presented as mean ± SD and median. Normality of data was tested by Kolmogorov–Smirnov test. If the normality was rejected, then non-parametric test was used. Statistical tests were applied as follows.
Quantitative variables were compared using paired t-test/Wilcoxon ranked sum test (for non-parametric data) across follow-ups within group and independent T-test/Mann–Whitney test (for non-parametric data) between the two groups. Qualitative variables were compared using χ2 test/Fisher’s exact test. A p value of <0.05 was considered statistically significant. The data was entered in MS EXCEL spreadsheet and analysis was done using Statistical Package for Social Sciences (SPSS) version 21.0.
Demographic data
Out of 102 patients, 85 were included in the study and randomized to one of the groups. In the SSI group, there were 43 patients (Male = 12, Female = 31) with a mean age of (56.4 ± 4.32) years (range, 48–64) and mean duration of symptoms 15.2 months and more non-dominant side involvement 69.7%. There were three diabetic patients and two hypothyroid patients. Three patients did not turn up for follow-up.
In the NTS group, 42 patients (M = 17, F = 25) with age range between 42 and 67 years (mean = 56.24 ± 5.42) and mean duration of 14.82 months with similar non-dominant side involvement 53%. There were four diabetics and two hypothyroid patients and two patients did not turn up for follow-up. From the p values in Table 1, it is clear that there was no statistical significance in the demographic parameters of patients (age, sex, duration of symptoms, side involvement, and stage of the disease and co-morbidities) included in the study.
Demographic tables.
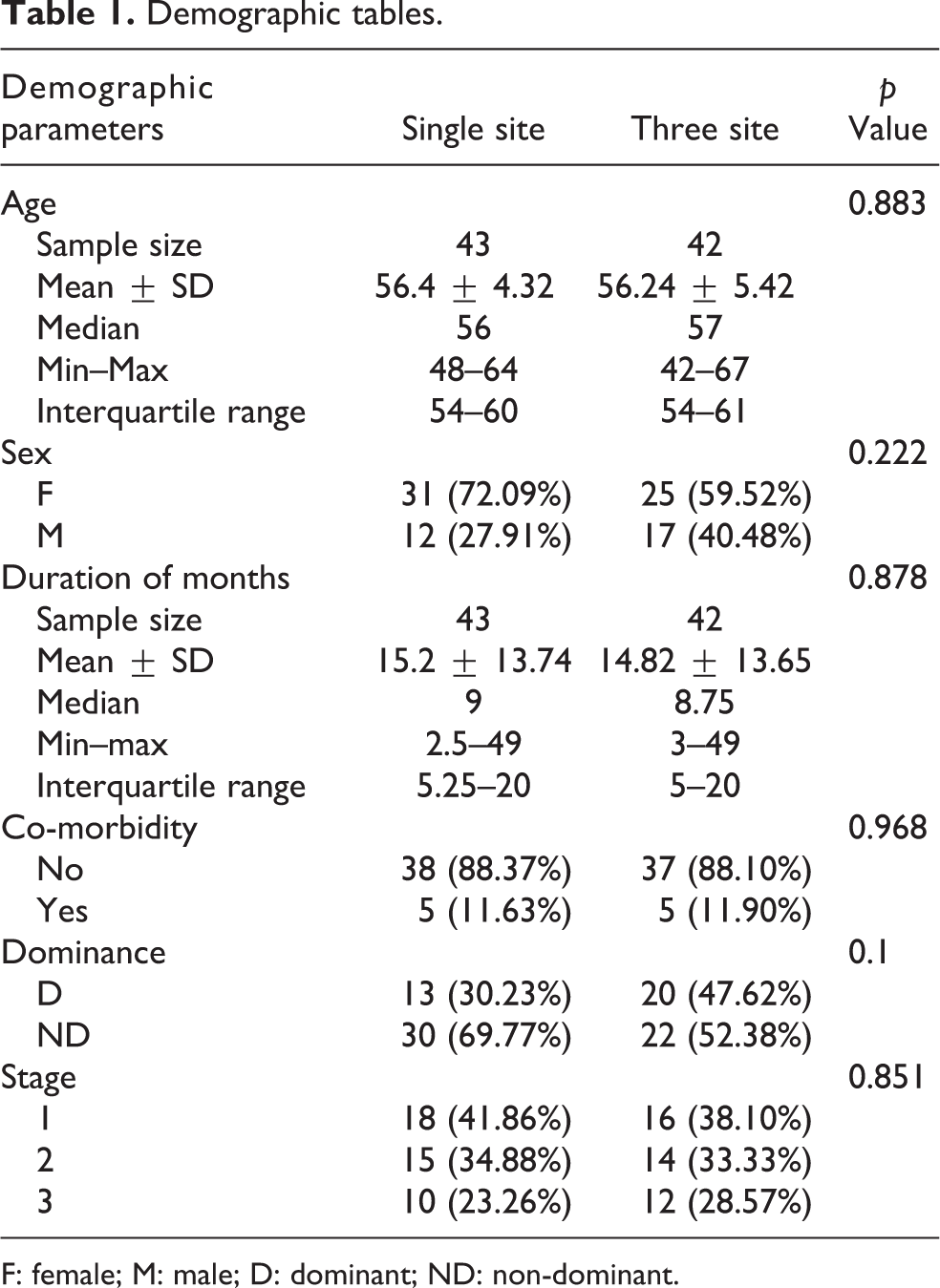
F: female; M: male; D: dominant; ND: non-dominant.
Results
There was no significant difference in the baseline values of the components of CONSTANT scores. The pain scores had significantly improved at successive visits in both the groups; however, the improvement in pain scores was much earlier and higher with the three-site injection group (p < 0.0005). Also, it is clear that few patients in the SSI group had discomfort at the 6-month follow-up (Figure 2).

Line diagram comparing the pain trend in both groups.
The activities of daily living (ADL) seemed to improve significantly from the baseline values with subsequent sittings in the NTS group. In the SSI group, significant improvements occurred only after the second sittings (Figure 3). The involvement and improvement of flexion was comparable with both the groups at all visits.

Comparison of the activities of daily living between the two groups.
The severity of abduction and external rotation involvement reveals the nature of the disease. Though the scores improved with subsequent visits, the improvement was only less than that expected in the SSI group (p < 0.0005). The NTS group had notably increased range of abduction and external rotation reaching almost near normal at 6 weeks and follow-up (Figures 4 and 5).

Subsequent improvement in the scores of range of movements in patients who received methyl prednisolone acetate through posterior approach.
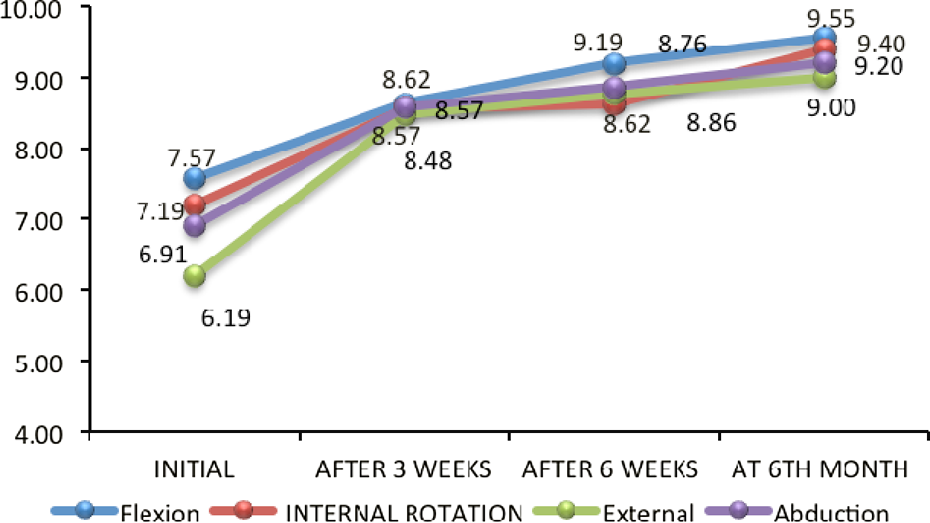
Linear diagram of the patients in the novel three-site injection group demonstrating the significant early improvement and near-normal range of movements attained by the end of 6 weeks and maintained till follow-up.
From Figures 6 and 7, it is clear that the CONSTANT scores improved significantly in both the groups. But the patients in the NTS group had faster rate of improvement and also attained near-normal scores. Four patients in the NTS group experienced tingling sensation around the arm which recovered in 3 days’ time. Apart from this, there were no major complications experienced in the study.

Strength trend in both the groups following steroid instillation suggesting a greater strength pattern in the three-site group.

Comparing the total CONSTANT scores in both the groups. Scores higher in the three-site group than the single-site group.
Discussion
The central pathology in frozen shoulder is inflammation of the capsule and the structures around it followed by fibrosis with type III collagen and absence of myofibroblasts, basically a Dupuytren-like disease. 25 There occurs contracture of the rotator cuff interval and coracohumeral ligament, 24 subacromial scars, loss of subscapular recess, fibrosis of capsuloligaments complex and a reduced GH joint volume. 26
Depalma 24 had explained the biomechanics in frozen shoulder by correlating contracture of the capsular ligament and specific pattern of GH movement restriction joint. Coraco humeral ligament (CHL) involvement restricts external rotation in neutral. Contracture of middle gleno humeral ligament (MGHL) and anterior inferior glenohumeral ligament (AIGHL) restricts external rotation in mid-elevation and external rotation in abduction, respectively. Whereas inferior capsule involvement causes restriction of abduction in neutral rotation and PIC causes internal rotation restriction. Oh et al. 27 also demonstrated that a single triamcinolone injection in the GH joint was no superior to the subacromial injections, indicating the multiple pathological sites of the disorder.
In this study, patients evaluated after a single sitting with the three-injection technique had significantly more range of abduction, external and internal rotation by about 40°, 25° and 20°, respectively, with only two resistances noted. Though there were improvements in abduction and external rotation, about 30% of patients in the single-site group had persistence of restricted movements even after 6 months with six resistance and three relapses, thus supporting the fact that instillation of steroids at target-specific sites of pathology in frozen shoulder had good outcomes.
Four of our patients had paraesthesia around the arm, probably the involvement of the musculocutaneous nerve. Maintaining the line of injection in the lateral third of coracoid prevents this complication. Because of this technique, the nerve is 20 mm away from injection site. 28
We also learned that patients in the NTS group were able to undergo physiotherapy comfortably and respond better indicated by the significant improvement in the activities of daily living. To our knowledge, this is one of the studies to demonstrate that steroid instillation in diluted doses at subcoracoid, subacromial and posterior capsule has better results than the traditional single posterior injection. Limitations of this study were (1) limited sample size, (2) less duration of follow-up (3) pain-specific outcome measures other than CONSTANT scores were not used, and (4) it is important to note that this study did not make use of a control group and the participants.
We concluded from this study that steroid instillation with this NTS techniques is safe, reliable and has early and near total functional outcomes with less relapses.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.