
Abstract
Introduction:
The purpose of this study was to evaluate the effectiveness of arthroscopic skills training.
Methods:
A routine diagnostic arthroscopic exercise using a porcine knee was performed. A checklist of 10 tasks was used in the training and the time taken to complete the checklist was evaluated, and the Arthroscopic Surgery Skill Evaluation Tool (ASSET) score was used to score the training and evaluate the practice session. A total of 14 residents attended this training, including five first- and second-year residents, five third- and fourth-year residents, and four orthopedic fellows. The ASSET score and time taken to complete the task checklist were evaluated, and the first and third practice sessions were scored to evaluate the effectiveness of the training.
Results:
The mean ASSET score improved from 21.8 in the first practice session to 24.9 in the third session (p < 0.001); the time taken to complete the task checklist decreased from 242 s in the first practice session to 207.5 s in the third session (p < 0.001). The ASSET score and the time taken to complete the task improved in all groups between the first and third practice sessions. The degree of improvement in the ASSET score and the time taken to complete the task checklist between the first and third practice sessions in each group were not statistically different among the groups (p = 0.857, p = 0.263, respectively).
Conclusion:
Porcine knees provide good material for residents and young orthopedic surgeons for teaching and training of arthroscopic surgical techniques.
Introduction
Arthroscopic techniques in orthopedic surgery are commonly used in clinical practice today, and orthopedic surgeons need to develop the necessary technical skills. However, delivering training in using arthroscopic techniques during residency can be difficult because of various reasons, such as limited opportunities to practice arthroscopy, paucity of suitable cases in the hospital, and unavailability of training tools. Techniques can be learned by observing procedures performed by experienced surgeons, reading books and journals, attending courses, or by practicing on cadaver models and simulators. Each method has its own advantages and disadvantages. 1 –4 Learning by observing procedures being performed by experienced surgeons or by attending courses provides the opportunity to experience actual management of pathologic lesions; however, not every orthopedic surgeon gets such a chance. A cadaveric knee is identical to the knee of a real patient; however, its large-scale availability is questionable. A simulator is less expensive than cadaveric models; however, whether training on a simulator would improve actual surgical performance is uncertain.
The porcine knee is another option. It is inexpensive, easily obtainable, and has the advantage of being anatomically similar to the human knee. In our institution, arthroscopic training is imparted using a porcine knee model. The purpose of this study was to evaluate the effectiveness of this training.
Materials and methods
Ten knees were obtained from healthy pigs that were older than 8 months and weighed more than 90 kg. Specimens were disarticulated from the hip and ankle joints. The mean length of the legs was 36.6 ± 0.8 cm. There was no gross deformity in any of the legs. The proximal femur was clamped in a holder for the knee to be flexed and extended. A 4-mm, 30° arthroscope was used in the study (Figure 1). A total of 14 residents participated in this training. They were five first- and second-year residents (the junior resident group), five third- and fourth-year residents (the senior resident group), and four orthopedic fellows (the fellow group). Each participant performed a set of 10 tasks three times. This checklist of 10 tasks was devised by Koehler et al. for evaluating diagnostic knee arthroscopy skills on cadaveric models (Table 1). 5 The time taken to complete the checklist was evaluated, and the Arthroscopic Surgery Skill Evaluation Tool (ASSET) score reported by Koehler et al. was used to score the training and evaluate the practice session (Table 2). 5

Use of porcine knee in arthroscopy. The proximal femur is fixed in a holder with the knee free to flex and extend.
Checklist of tasks to be performed for assessing skills in diagnostic arthroscopy of the knee.

ACL: anterior cruciate ligament; PCL posterior cruciate ligament.
The ASSET global rating scale.

ASSET: Arthroscopic Surgery Skill Evaluation Tool.
The ASSET score and the time taken to complete the task checklist were evaluated by an arthroscopic fellowship-trained orthopedic surgeon who was blinded to the participant group and practice round. The difference between the scores in the first and third practice sessions was used to evaluate the effectiveness of the training.
The Wilcoxon signed rank test was used to compare the values in the first and third practice sessions. The Kruskal–Wallis test was used to compare the values for each group in the third practice session, as well as the degree of improvement between the first and third sessions in each group. We used IBM SPSS Statistics version 19.0 (Armonk, New York, USA) for the statistical analysis; p < 0.05 was considered significant.
Results
The mean ASSET score of the 14 participants improved from 21.8 in the first practice session to 24.9 in the third session (p < 0.001), and the time taken to complete the task checklist decreased from 242 s in the first practice session to 207.5 s in the third session (p < 0.001).
The ASSET score improved in all groups between the first and third practice sessions. The score improved from 13.0 to 16.0 in the junior resident group (p = 0.041), from 23.2 to 26.6 in the senior resident group (p = 0.039), and from 31.0 to 34.0 in the fellow group (p = 0.102; Figure 2(a)).

(a) The ASSET score improved in all three groups. The score improved from 13.0 to 16.0 in the junior resident group, from 23.2 to 26.6 in the senior resident group, and from 31.0 to 34.0 in the fellow group. *p < 0.05. (b) The time taken to complete the tasks improved in all three groups. The time decreased from 294.0 to 256.0 s in the junior resident group, from 227.0 to 189.8 s in the senior resident group, and from 195.8 to 169.0 s in the fellow group. *p < 0.05. ASSET: Arthroscopic Surgery Skill Evaluation Tool.
The time taken to complete the task checklist also improved between the first and third practice sessions. The time decreased from 294 s to 256 s in the junior resident group (p = 0.043), from 227 s to 189.8 s in the senior resident group (p = 0.043), and from 195.8 s to 169.0 s in the fellow group (p = 0.068; Figure 2(b)).
The improvement in the ASSET score and the time taken to complete the task checklist was statistically significant in the junior and senior resident groups, but not in the fellow group. The degree of improvement in the ASSET score and the time taken to complete the task checklist between the first and third practice sessions in each group were not statistically different among the groups (p = 0.857, p = 0.263, respectively).
Discussion
In this study, the mean ASSET score and the time taken to complete the task checklist improved between the first and third practice sessions in all participant groups, indicating that training using porcine knees can improve arthroscopy skills. The improvements in score and time were not statistically significant in the fellow group, whereas they were significant in the junior and senior resident groups. It appears that the training is more effective in those with less experience.
Practice on the human body would be the best option for imparting training in using arthroscopic techniques; however, this is limited by local laws, religion, cost, and the lack of body donation in some countries. There are also limited opportunities to participate in actual arthroscopic operations.
Many authors have used animal models of the knee, such as those of pigs, cows, lambs, dogs, and horses. 3 The porcine knee is particularly useful for training purposes because of its similarity to the human knee. 6 The anatomy of the porcine knee is similar to that of the human knee, both grossly and radiographically (Figure 3); the arthroscopic features are also similar (Figure 4). Besides, porcine knees are easily obtained and are not expensive. 2
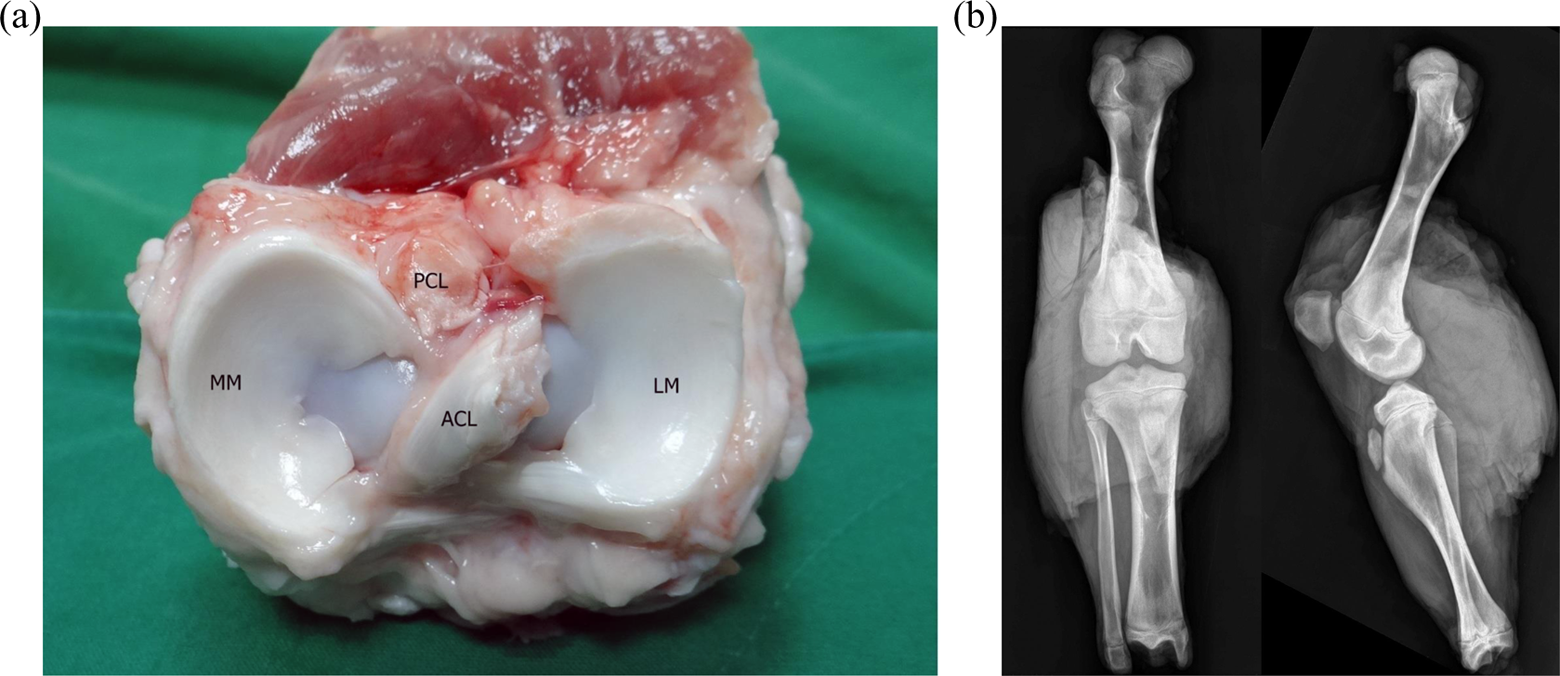
(a) Gross anatomy of a porcine knee. LM: lateral meniscus; MM: medial meniscus; ACL: anterior cruciate ligament; PCL: posterior cruciate ligament. (b) AP and lateral radiographs of a porcine knee. AP: anteroposterior.

Arthroscopic anatomy of a porcine knee. (a) Patellofemoral joint. P: patella; F: femoral groove. (b) Medial compartment. MM: medial meniscus; F: femur; T: tibial plateau. (c) Lateral compartment. LM: lateral meniscus; F: femur; T: tibial plateau. (d) Intercondylar notch. ACL: anterior cruciate ligament; PCL: posterior cruciate ligament.
Many scoring tools are used to assess operator performance in surgery. Insel et al. used the Basic Arthroscopic Knee Skill Scoring System for assessing surgeon performance in arthroscopic partial meniscectomy in cadaveric knees. 7 Hoyle et al. 8 created the Global Rating Scale for Shoulder Arthroscopy to assess video recordings of diagnostic shoulder arthroscopy. Koehler et al. reported that the ASSET appeared to be a useful, valid, and reliable method for assessing surgeon performance in diagnostic knee arthroscopy in cadaver specimens. 5 The ASSET was utilized to assess performance in diagnostic knee arthroscopy in porcine knees. As expected, the more experienced surgeons had higher scores; however, after three practice sessions, the scores of all the participants improved.
This study has several limitations. First, only one assessor rated the score, and the number of participants and practice sessions were small. It is also not yet possible to know whether the training using porcine knees will improve actual operating room performance. Consequently, further research is needed to compare training imparted through the use of porcine and cadaver knees.
Conclusion
Porcine knees provide good material for training residents and young orthopedic surgeons in using arthroscopic techniques, and this may aid in developing surgical skills.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.