
Abstract
Purpose:
Following far advancement of modern medicine and technology, functional disability in a certain type of sequelae of poliomyelitis may be effectively improved.
Methods:
Eight consecutive adult patients with unilateral sequelae of poliomyelitis were treated. These patients had shortened lower extremity of an average of 4.8 cm (range, 4.0–5.5 cm) in the lesion side. Muscle power of the ipsilateral knee was nearly intact (grade 4 or 5) but the ankle extension was completely flaccid. The tibia was osteotomized and lengthened with external fixation. Consequently, all external fixators were converted to plates supplemented with autogenous corticocancellous bone graft and bone graft substitute. Ankle arthrodesis was performed concomitantly.
Results:
Seven patients were followed up for an average of 3.7 years (range, 2.2–5.4 years). All seven lengthened sites healed with an average union time of 3.9 months (range, 3.5–4.5 months) after plating. One ankle infection occurred. Gait function significantly improved by modified Mazur scoring evaluation (p = 0.02). At the latest follow-up, all patients had a minimal or unnoticed limp in level walking.
Conclusion:
The described combined techniques may be an excellent alternate for treating selected patients with sequelae of poliomyelitis. The procedure is not complex but the efficiency is extremely prominent.
Introduction
Following far advancement of human civilization and modern medicine, the incidence of poliomyelitis has greatly decreased. 1 However, complete extinguishment of this disease from the world may still be indefinite. In the author’s country, patients with acute poliomyelitis have rarely appeared but those with sequelae of poliomyelitis of low back pain and a limp may be met at the outpatient department (OPD) sporadically.
Sequelae of poliomyelitis may be multiple and the severity is varied. 2 Clinically, not all sequelae of poliomyelitis are suitable for treatment. Following far advancement of modern medicine and technology, theoretically some anomalies may be treated effectively with current techniques. Especially, for patients who have only unilateral lesions, a limp may introduce pelvic torsion and intractable low back pain. 3 The pathomechanism is imputed to leg length discrepancy (LLD) and loss of muscle power in extensors of the hip, knee, and ankle. 4 If both disorders are effectively treated, significant improvement of daily activity may be anticipated.
Techniques for improving disabilities caused by poliomyelitis are various. Patients may lose extensor power of the knee, ankle, or both in different degrees. 4 Following far advancement of techniques of limb lengthening and ankle arthrodesis, 5,6 patients who can be successfully treated by combined techniques may achieve significant improvement in daily activity. The purpose of this retrospective study was to investigate patients with a certain type of sequelae of poliomyelitis, who were treated with combined techniques. The degrees of improvement were quantitatively evaluated and possible surgical indications were comprehensively established.
Materials and methods
From March 2003 to May 2011, eight consecutive adult patients (>18 years) who had sequelae of poliomyelitis (drop foot but nearly intact knee extension function) were treated by the single author using combined techniques at the author’s institution. Patients aged from 24 years to 56 years (average, 39 years) with a male to female ratio of 2:1. All patients sustained poliomyelitis since their childhood. Except the unilateral lower extremity, no other anatomic sites were involved. All patients walked with a limp but no aids were necessary. Although a heel lift had been used by some patients, low back pain occurred intermittently in all patients. All patients visited the author’s clinics because they gained public messages that gait function might be markedly improved after treatment.
At the OPD, the disease course was carefully pursued. The muscle power and range of motion (ROM) around the hip, knee, and ankle were evaluated manually and using a goniometry. A full-length standing scanogram was routinely taken. The treatment plan was explained thoroughly to patients. Indications for combined techniques included a unilateral lesion, LLD ≥ 4 cm, the main shortening being in the tibia, knee extensor power of grade 4 or 5, 7 and complete loss of ankle dorsiflexion ability. Inclusion criteria for this study were sequelae of poliomyelitis with unilateral lesions, drop foot, nearly normal knee extension function, and LLD ≥ 4 cm. Exclusion criteria were bilateral lower extremity abnormality (no need of correction), significant loss of knee extensor muscle power or associated with foot deformity (32 patients), and main shortening being in the femur (five patients). Patients with main shortening in the femur would be treated with femur lengthening and were excluded. 8 Patients with abnormal ipsilateral knee extensors or foot deformity were excluded to avoid interfering with the evaluation of gait function. In these eight patients, the shortened lower extremity was an average of 4.8 cm (range, 4.0–5.5 cm) in the lesion side. The tibia was shortened of an average of 3.1 cm (range, 2.5–3.5 cm) and the femur of an average of 1.8 cm (range, 1.5–2.0 cm).
Surgical technique
In the first stage of surgery
Under the generalized anesthesia with endotracheal intubation or spinal anesthesia, the patient was placed at the operating table in the supine position. A pneumatic tourniquet was used routinely.
A mid-third fibulotomy was performed first. After a mid-third tibial shaft osteotomy was performed with a power saw, a lengthening external fixator (Ilizarov or TraumaFix external fixator; Paonan Biotech Co., Taipei, Taiwan) was applied. The wound was closed with nonabsorbable sutures.
The patient was advised to use crutches and followed up at the OPD. Lengthening of the tibia was implemented by the patient with 1.0–1.5 mm per day at home. Passive ankle dorsiflexion was encouraged as tolerated. The pin tract site was cared with 70% alcohol solution once per day. After the desired length was achieved, the patient was re-admitted.
In the second stage of surgery
Under the generalized anesthesia with endotracheal intubation, the patient was placed at the operating table in the lateral decubitus position. Corticocancellous bone graft was procured from the ipsilateral posterior iliac crest as much as possible. Then, the patient was changed to a supine position and the external fixator was removed. A pneumatic tourniquet was applied.
The lengthened site in the tibia was opened directly. Generally, the tissues in this area were unhealthy and fragile. The local area was completely debrided. With the assistance of a spinal spreader, the gap was distracted up to the desired length. A dynamic compression plate (Synthes, Bettlach, Switzerland) was inserted on the lateral aspect of the tibia with four cortical screws on each fragment. Corticocancellous bone graft with or without bone graft substitute (Wiltrom, Hsinchu, Taiwan) was packed in the gap. Four vials of vancomycin powder were placed in the local area to prevent infection. The wound was closed with nonabsorbable sutures.
The ankle fusion was performed with a directly anterior approach on the ankle joint. The articular surfaces of the tibial plafond and talus were resected with a power saw. The ankle alignment was adjusted. Right angle, mild external rotation, and mild valgus of the foot were preferred. 5,9 The gap was filled with cancellous bone graft and the ankle was stabilized with two staples (Richards, Memphis, Tennessee, USA). A short leg splint was applied. Three patients needed to perform Achilles tendon lengthening concomitantly. It was done with an oblique incision of the Achilles tendon and sutured after the ankle fusion was completed.
Postoperatively, early ambulation with protected weight bearing was permitted. Knee ROM exercise was encouraged. Patients were followed up at the OPD in 4–6-week intervals. Clinical and radiological bony healing processes were recorded. Crutches were discontinued after bony healing was achieved. After the bone healed, the patient was advised to follow up each year and whenever necessary.
Bony union was defined as clinically there was no pain and tenderness, and radiographically solid callus had connected both fragments. 10 Nonunion was defined as the local area was still not healed after 1-year treatment or requirement of a second operation to achieve bony union. 11
Gait function was evaluated with the functional mobility scale (FMS) and modified Mazur scoring system. 12,13 The two scoring systems were used individually because of varied requirement for poliomyelitis patients. The FMS focused on the ability of walking in different distances (5, 50, and 500 m). It was deeply dominated by the disease severity. The modified Mazur scoring system (excluding pain and ROM; 40 points of total scores in nine items) was used to evaluate the worth of concomitant ankle fusion. It included limp (six points), downhills (three points), downstairs (three points), ability to rise on toes (five points), running (five points), distance (six points), uphills (three points), upstairs (three points), and support (six points). More than 90% of total scores (≥36 points) was considered as an excellent grade and 80–89% of total scores as a good grade (≥32 points). A fair grade was 70–79% of total scores (≥28 points), and a poor grade was less than 70% of total scores (<28 points). A satisfactory outcome included an excellent or good grade.
Statistical comparison was performed using the Wilcoxon signed rank test (SPSS Version 11.0; SPSS Inc., Chicago, Illinois, USA). A p value <0.05 was considered statistically significant.
Results
Seven patients were followed up for an average of 3.7 years (range, 2.2–5.4 years). One patient was lost despite the greatest efforts to contact him.
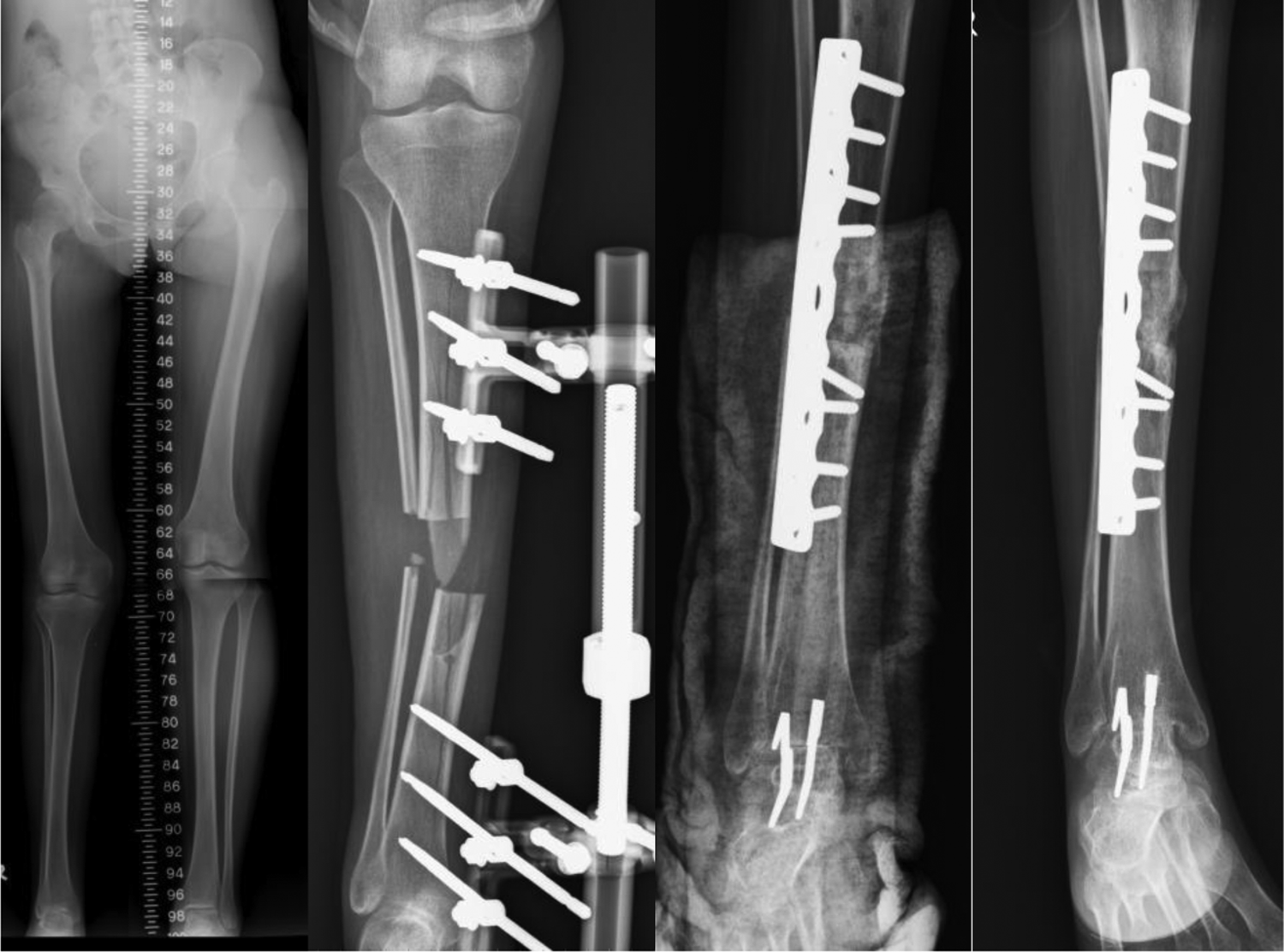
External fixation in seven patients was applied for an average of 5.9 weeks (range, 5–6 weeks). All lengthened sites healed with a union rate of 100% and an average union time of 3.9 months (range, 3.5–4.5 months) after plating (Figures 1 and 2; Table 1). Except one ankle, six ankles fused within 4 months. This special case was due to deep infection (case 6, fusion at 7 months, Figure 3).
Case 2: A 28-year-old woman sustained poliomyelitis with shortening of right lower extremity of 5 cm (femur, 2.0 cm; tibia, 3.0 cm). The tibia was lengthened of 4.0 cm and ankle arthrodesis was performed. A good gait function with an unnoticed limp was achieved for 4.8-year follow-up.

Case 3: A 52-year-old man sustained poliomyelitis with shortening of left lower extremity of 5.5 cm (femur, 2.0 cm; tibia, 3.5 cm). The tibia was lengthened of 4.0 cm and ankle arthrodesis was performed. A good gait function with an unnoticed limp was achieved for 3.7-year follow-up.

Case 6: A 31-year-old man sustained poliomyelitis with shortening of right lower extremity of 4.5 cm (femur, 1.5 cm; tibia, 3.0 cm). The tibia was lengthened of 3.5 cm and ankle arthrodesis was performed. Unfortunately, ankle infection occurred at 3 months and staples were removed after debridement. The ankle fused 4 months later. A good gait function with a minimal limp was achieved for 2.9-year follow-up.
Clinical data of patients with sequelae of poliomyelitis treated using combined techniques.

EF: external fixation; F: female; LLD: leg length discrepancy; M: male.
There were no nonunion and malunion (angular or rotational deformity >5°; shortening >2 cm). One patient (case 6) had deep infection in the ankle at 3 months. The staples were removed after debridement and vancomycin powder was placed locally. An ankle-foot orthosis was wear for 4 months and the ankle fused uneventfully (Figure 3; Table 2). The final LLD of seven cases was an average of 1.1 cm (range, 1.0–1.5 cm) as measured by full-length standing scanograms (Table 1).
Clinical data of patients with sequelae of poliomyelitis treated using combined techniques.

FMS: functional mobility scale (total, 6 points); mMazur: modified Mazur scoring system (total, 40 points).
Gait function improved at the latest follow-up (27.6 versus 34.1; p = 0.02) as evaluated by the modified Mazur scoring system (Table 2). All achieved a satisfactory outcome. There was no change in the FMS. Before treatment, all patients had a limp. At the latest follow-up, all patients had a minimal or unnoticed limp in level walking.
Discussion
Not all sequelae of poliomyelitis need treatment and can be treated effectively. 3 The outcome after treatment may still be unsatisfactory or even more deteriorated. In this study, only those patients who could be treated with current well-established techniques (limb lengthening and ankle arthrodesis) were selected and all achieved a great success in 3.7-year follow-up.
Patients with poliomyelitis may have very different motor function impairment. 3,4 Very commonly, patients lose extension power in the hip, knee, and ankle. Almost all patients have associated with significant LLD (>2 cm). 4 The combined anomalies may introduce progressive pelvic torsion and intractable low back pain. 3,4 Complete treatment of these disorders is difficult. However, for patients with significant LLD and nearly intact knee motor function, treatment of LLD and ankle disorders may achieve maximal efficiency. The author referred to various patients in his clinics and finally classified them into three categories: type 1, loss of knee extension function but preservation of ankle dorsiflexion function; type 2, loss of ankle dorsiflexion function but preservation of knee extension function; type 3, loss of both knee and ankle extension function. In author’s clinics, the incidence of these three types of patients was approximately 2:1:2. In the current study, treatment of unilateral type 2 anomalies had achieved the highest satisfactory rate.
In normal individuals, more than 2 cm of LLD will introduce a limp. 14,15 A heel lift is suggested for 2–4 cm of LLD. More than 4 cm of LLD is advised to surgical correction because of inconsistent level of the knee joint. However, in patients associated with drop foot, a heel lift on the orthosis may be too clumsy to wear. To improve the gait, lengthening of the limb may be more practical. In this study, all patients had an LLD of less than 2 cm (average, 1.1 cm; range, 1.0–1.5 cm) after tibial lengthening, and no heel lift was needed.
LLD in patients with poliomyelitis is normally due to combined shortening of the femur and tibia. However, it is unnecessary to lengthen both bones concomitantly. Usually, one bone is more severe and lengthening of this bone is sufficient. In patients with type 2 motor dysfunction in poliomyelitis, the LLD is normally not severe. In this study of eight patients, the shortened lower extremity was an average of 4.8 cm (range, 4.0–5.5 cm). The tibia was shortened of an average of 3.1 cm (range, 2.5–3.5 cm) and the femur of an average of 1.8 cm (range, 1.5–2.0 cm). Therefore, over-lengthening of the tibia to compensate with the femur shortening was performed. The result was very successful.
Techniques for ankle arthrodesis have been continuously developed and a high success rate has been reported. 5 The orientation of ankle fusion has been recommended, and cancellous bone grafting to improve a fusion rate is suggested. In the current study, the ideal principle was followed and a successful fusion was achieved in all patients (even with one infection). Drop foot in poliomyelitis patients generally cannot be treated with anterior transfer of the posterior tibial tendon. For poliomyelitis patients, flexors in the ankle and foot are also weak. The tendon is useless after transfer. 7 When a tendon is rerouted to a new pathway, its muscle power will decrease at least one grade. 16 Osteotomy with gradual lengthening is normally very uncomfortable. In addition, the soft tissue tension is huge during gradual lengthening, which may compromise the fixation stability in ankle fusion. Therefore, osteotomy with gradual lengthening and ankle fusion should not be performed concomitantly.
The patient with ankle deep infection (case 6) is grossly healthy, and preoperative laboratory data are within normal limit. The postoperative course is smooth until 3 months. The infection source is obscure and hematogenous spread may be most possible.
Converting external fixation to plating requires a spinal spreader to maintain the length and adjust the alignment. The local tension is huge and submuscular plating is less possible. For preventing deep infection from the pin tract, local antibiotics of vancomycin are placed. 14 Most wound infection is caused by Staphylococcus aureus (S.A.) as reported in the literature and the author’s institution. Various ratios of S.A. are methicillin sensitive or resistive. However, nearly all S.A. are vancomycin sensitive. Local placement of vancomycin powder during plating is more reasonable.
In the literature, various outcomes in the treatment of sequelae of poliomyelitis with tibial lengthening were reported. Huang treated 35 patients using single Ilizarov technique for tibial lengthening. The complication rate was 68.6% and a satisfactory rate was 82.9%. Using the Ilizarov over intramedullary nailing technique in 12 patients, a 33.3% complication rate occurred but a 100% satisfactory rate was achieved. 17 Song et al. reported 14 patients treated with the Ilizarov over intramedullary nailing technique. Foot deformity was corrected concomitantly using Ilizarov frame with or without local fusion. The satisfactory rate was 57.1%. 18 Emara and Khames treated 32 patients (21 without and 11 with associated knee or foot deformity) using the simple Ilizarov technique. No significant improvement of gait function was found. 19 However, in the current study, all seven patients could achieve nearly normal gait function in level walking. The main difference might be that all seven patients were selected and their knee extension function was nearly intact. However, in previous studies, all patients without selection were treated and knee function might deeply affect outcomes. Once the LLD was corrected in the current series, the gait was completely similar to those patients after ankle arthrodesis. As long as the ankle arthrosis is well maintained, a long-term satisfactory outcome is predictable. 5,13,20 In the current study, all external fixators were converted to plates and not locked intramedullary nails. It was because all tibial diameters were too small to use intramedullary nails.
Some limitations in the current study may not be disregarded. (1) The sample size is small (seven patients) and time of follow-up is short (average, 3.7 years). After all, patients with poliomyelitis are very rare now. The long-term outcomes may be similar to those patients with different causes for ankle arthrodesis. (2) Gait function needs evaluation with a modified scoring system. In previous reports, the severity of all patients was not separated, and the comparison with the current study was unfair. (3) All patients in the current study had no ankle pain before and after treatment. Therefore, pain score in gait functional evaluation was removed. The total scores become smaller and a satisfactory outcome must be redefined.
In conclusion, the described combined techniques may be an excellent alternate for treating selected patients with a certain type of sequelae of poliomyelitis. The procedure was not complex but the efficiency is extremely prominent.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.