
Abstract
Background:
Surgical dislocation of the hip remains an important alternative in hip preservation surgery, especially when a dynamic access to the hip is needed and arthroscopy is not a suitable option. We describe a novel technique for operative dislocation of the hip without trochanteric osteotomy and the clinical results of our patients.
Methods:
Surgical dislocation of the hip without trochanteric osteotomy was done through a modified lateral approach in all of the cases. A review of demographic, clinical, and radiological data was done in all of the patients operated with this technique between 2010 and 2015. Complications, walking aids, weight-bearing status, and modified Harris Hip Score (mHHS) were also recorded.
Results:
Six surgical dislocations of the hip were carried out. Indications were tumor resection in five and bulletectomy in one hip. There were two women (four hips) and two men. Mean age was 19 ± 3.8 years. Median follow-up was 2.5 years (range 2–4.5 years). Median mHHS was 92 (90–96). There were no intraoperative nor postoperative complications.
Conclusions:
Surgical dislocation of the hip without trochanteric osteotomy through a modified lateral approach appears to be a safe, simpler, and effective alternative.
Introduction
While hip arthroscopy has become the most frequently used technique to asses most of intra-articular pathologies, surgical dislocation of the hip remains an important alternative, especially for scenarios that require a complete and dynamic access to the hip where arthroscopy is not a suitable option. Since Ganz et al. first described the technique and their results, there has been an increasing number of indications for surgical hip dislocation. The most cited indications are Legg-Calvé-Perthes disease, 1,2 slip capital femoral epiphysis, 3,4 and femoroacetabular impingement (FAI). 5,6 Traumatic pathology, 7 –9 bone or intra-articular tumors like pigmented villonodular synovitis, 10 or synovial chondromathosis 11 are less frequent indications.
Surgical dislocation may be performed using anterior, lateral, or posterior approach to the hip. Ganz et al. described the trochanteric flip approach consisting in an anterior dislocation via posterior approach and trochanteric osteotomy. They reported good outcomes with no avascular necrosis (AVN); nevertheless, the trochanteric flip fixation failed in three patients and 37% presented of heterotopic ossifications. 12
Sink et al. reported trochanteric nonunion in 1.8%, with no cases of AVN in 334 surgically dislocated hips in a short-term follow-up of at least 5.8 months. 13 Other potential complication for osteotomy and fixation could be lateral pain, bursitis, and need for hardware removal. Beaule et al. reported the need for screw removal in 9 of 34 cases treated with surgical hip dislocation. 14
Anterior approaches like Hueter and Smith Petersen have been used as an alternative to surgical hip dislocation when combined with an arthroscopic management of the FAI. Promoters propose the advantage of not requiring dislocating the hip, but with the downside of missing the full exposure of the acetabulum. 15,16
Patient demographics.

AVN: avascular necrosis.
To the best of the authors’ knowledge, there is no description of the surgical dislocation of the hip without flip osteotomy of the major trochanter, through a modified lateral approach. The rationale of intending this modification despite the good outcomes reported in the literature is simplifying the procedure, with the hypothesis that outcomes will be comparable.
Our objective is to describe the technique for the surgical dislocation of the hip without a trochanteric osteotomy in a modified direct lateral approach and the clinical results of our patients at midterm follow-up.
Patients and methods
Surgical technique
With the patient in lateral decubitus position, the surgical wound is drawn 1 cm anterior to the major trochanter center, parallel to the femoral diaphysis (Figure 1). In line dissection to the fascia lata tensor, adherences of the fascia must be liberated with finger dissection or electrocautery. A double-loop automatic retractor (Alexis®, Applied Medical, Rancho Santa Margarita, California, USA) was used to easily retract all the soft tissue and expose the major trochanter.

Skin marks before starting the procedure. MT: major trochanter; ASIS: Anterior Superior Iliac Spine.
Bursectomy is performed to better expose gluteus medius and proximal margin of the lateral vastus (Figure 2). The anterior fibers of the gluteus medius are divided, keeping the gluteus minimus in situ. With electrocautery, the proximal end of the muscle and tendon of the lateral vastus is incised in line with its fibers. Turning the electrocautery over the anterior third of the major trochanter, the incision is directed to connect with the one performed over the gluteus medius.

Abductor release marks. GM: gluteus medius; MT: major trochanter.
One anterior flap including the vastus and gluteus medius is performed. After moving anteriorly the flap, the gluteus minimus is incised in line with its fibers, allowing access to the joint capsule. “Z-shaped” capsulotomy with the first incision anterolateral in line with the neck axis protects the deep branch of the medial femoral circumflex artery (MFCA) (Figure 3). The capsulotomy continues distally anterior and inferior to the lesser trochanter, protecting the main branch of MFCA. The proximal and posterior margin of the capsulotomy requires special care to prevent injury to the labrum.

Capsulotomy.
To perform dislocation, the ligamentum teres must be transected. Sometimes, it is torn with maximal external rotation. Dislocation maneuver is standard, with a flexion, external rotation, and adduction. After dislocating, by manipulation of the leg, the surgeon has 360° access to the femoral head with no need of the trochanteric osteotomy (Figure 4) and full exposure of the acetabulum.
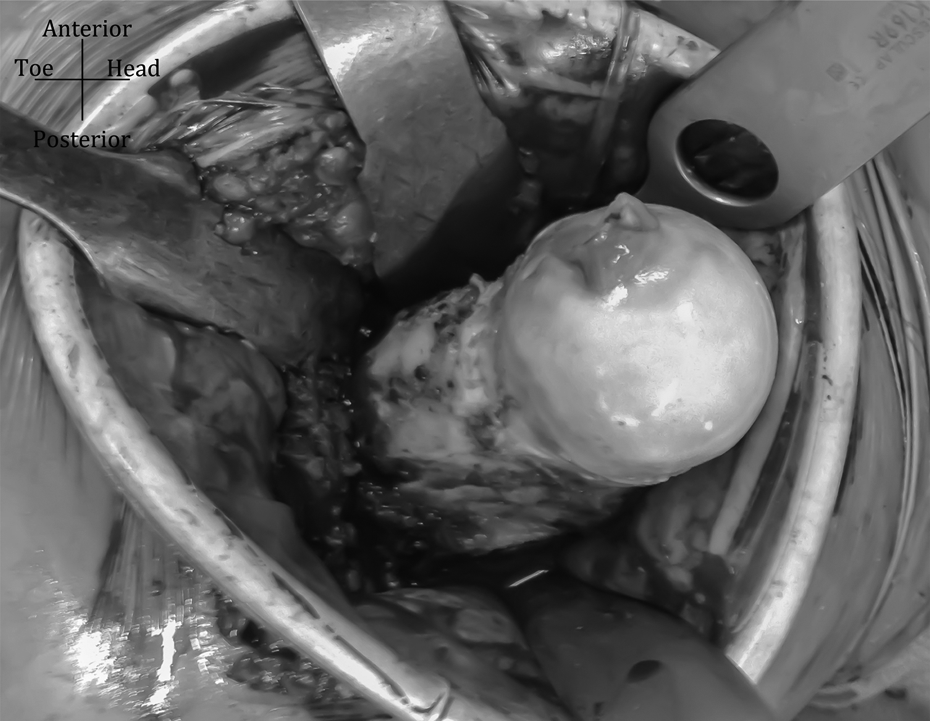
Complete exposure of the femoral head.
In two patients, four hips with multiple exostosis (cases 2 and 4) due to the abnormal metaphysis and frail femoral neck, two prophylactic screws were used before dislocating the hip (Figure 5).

X-ray, prophylactic screws.
After completing the procedure, the femoral head is reduced, and then, the capsule repaired following the “Z” shape incision. The rest of the closing technique has been previously described by Hardinge 17 and other authors. 18,19
In the rehabilitation protocol for protecting abductor reinsertion, active abduction exercises were delayed 4 weeks after surgery. Patients were advised to partial weight bearing with two and then one crunches. Routine clinical and radiological follow-up was carried out at 6 weeks postoperative, then at 3, 6, and 12 months, and then once a year after that.
A review of all patients treated with a surgical dislocation of the hip was performed. Clinical and radiological data were collected. This included age, sex, primary diagnosis, and performance status preoperative and postoperative. Also, inpatient evolution and intra- or postoperative complications were prospectively recorded. Pain and abductor muscle strength, walking aids, and weight-bearing status were documented at every clinical visit during follow-up. Modified Harris Hip Score (mHHS) was also recorded at the last visit.
Results
Six surgical dislocations of the hip in four patients were carried out by the senior author (DS) between 2010 and 2015. The indications for treatment were multiple exostosis in four hips, a giant cell tumor curettage in one patient, and a bulletectomy in the last hip. There were two women (both of them with bilateral surgery) and two men. The mean age was 19 ± 3.8 years. In three patients, prophylactic fixation with cannulated screws or a dynamic hip screw was used for femoral neck fracture prevention during dislocation.
There were no intraoperatory nor surgery-related complications in the immediate nor delayed postoperatory follow-up.
Length of hospital stay was 6 days (3–10 days).
All patients were followed for a minimum of 2 years, with a median of 2.5 years (2–4.5 years). All patients were free from walking aids at last follow-up with full weight bearing. The median time for leaving one crutch was 3 months (1.5–12) and for being free from walking aids 7.5 months (3–24). A slight Trendelenburg gait was evident for 2.25 months after surgery (1.5–3).
The median mHHS was 92 (90–96). Lateral (pertrochanteric) pain was reported for 1.5 months (0–3). We have found no clinical or radiological evidence of AVN, heterotopic ossification, or any other long-term complication at that point either.
Discussion
Any new surgical technique should be comparable to those previously used for the same purpose, without adding any safety issues, also at the same time, addressing some specific points that could be an opportunity for improvement. Our small case series using the modified lateral approach for surgical dislocation of the hip without trochanteric osteotomy show good results, without any major complication related to the technique being a relatively easier access to the hip.
Epstein favored reduction after dislocation via the posterior approach, reporting 5.3 versus 18% of femoral head osteonecrosis comparing with an anterior approach. 20,21 They suggested the Kocher-Langenbeck approach for posterior wall fracture treatment, releasing the external rotators and the gluteus medius from the major trochanter, protecting the medial circumflex femoral artery and the sciatic nerve. The anterior approach for these cases would jeopardize the remaining blood flow to the femoral head, as it requires ligating the lateral femoral circumflex argtery.
For femoral head fractures, Swiontkowski et al. reported no AVN after anterior approach in a comparative study. They also reported shorter surgical time, less blood loss, better visualization of the femoral head, and easier reduction when comparing with posterior approach; in the follow-up, they found higher rate of heterotopic ossifications. 22
Our lateral approach, surgical hip dislocation, was originally thought by one of the authors after noting the easy dislocation for primary hip arthroplasty with the modified lateral approach without the need of previous trochanteric osteotomy, preserving blood flow to the femoral head. Then, the surgical team, after profound review of the surgical anatomy, decided to perform future surgical dislocations using the one approach they used the most, the modified lateral. Previous published work states the safeness for performing the lateral approach to the hip joint having some precautions. Dissecting from lateral and through anterior using the lesser trochanter as a safe limit keeps the MFCA and its deep branch from being injured. 23 –25
We found that surgical dislocation, without the need of a trochanteric osteotomy, allows full access to the femoral head and acetabulum, with a 360° view, useful for intra-articular pathology not amenable for arthroscopic treatment. This point is of special importance in tumoral conditions as described by Nisar et al. 26 and as observed in our cases.
The lateral approach has been related with higher prevalence of claudication and peritrochanteric pain after surgery. These issues were documented and briefed in these small series, with similar time frames than the authors have experienced for hip arthroplasty using the same approach. The amount of time patients used crutches is probably related more to the type of pathology treated and the bilateral compromise in two of the patients than with the approach used.
The small number of patients reported here makes it impossible to compare in terms of outcomes to those reported with posterior approach and trochanteric flip by Ganz and others, but it allows us to think of one technically easier method, an alternative for reducing the complications directly related to the trochanteric osteotomy.
Despite the growing number of indications for hip arthroscopy, there is still pathology not amenable for arthroscopic treatment because of the location or the size of the lesion; in those cases, surgical dislocation of the hip might be a helpful alternative. Some indications might be femoral head fractures, epiphyseal tumors or intra-articular pseudotumors, 26 FAI, 27,28 better reduction of acetabular fractures, 29 and slipped capital femoral epiphisis. 30
Further research is warranted, but the increasing indications for hip arthroscopy makes thinking in a randomized control trial comparing posterior versus lateral approach without flip osteotomy hard to come in the near future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.