
Abstract
Purpose:
This study is to report a new method to reduce and fix the displaced flexion-type pediatric supracondylar fracture in the prone position.
Methods:
Ten children with displaced flexion-type supracondylar humeral fractures treated between 2007 and 2013 were reviewed. There were three girls and seven boys, with a mean age of 9.5 years. The fracture was reduced by gentle traction of the forearm and gradual extension of the elbow in the prone position. Two or three crossed Kirschner wires (K-wires) were inserted percutaneously to secure the fracture reduction. Radiographic evaluation included the Baumann’s angle and the lateral humerocapitellar angle. Clinical outcomes were assessed using the Flynn’s criteria.
Results:
Eight children had closed reduction and percutaneous K-wire fixation. The other two children required open reduction through a posterior triceps splitting approach. The mean Baumann’s angle was 70.2° immediately after K-wires fixation and 69.5° after 3 months later. The mean lateral humerocapitellar angle was 38° immediately after K-wires fixation and 35.5° after 3 months later. The clinical outcome was excellent in nine children and poor in one child by the Flynn’s criteria.
Conclusion:
Reduction of displaced flexion-type pediatric supracondylar humeral fractures by traction and gradual extension in the prone position is an effective and safe method. When reduction is still impossible or nerve incarceration is suspected, open reduction and release of the trapped nerve through a posterior triceps splitting approach are simply accessible.
Introduction
Supracondylar humeral fractures are the most common elbow fractures in children. 1 Most of the supracondylar humeral fractures are displaced in the extension position. Flexion-type fractures are uncommon and account for only 2–10% of all supracondylar humeral fractures in children. 2 –6 The injury results from a fall directly onto the elbow rather than the outstretched hand with hyperextension of the elbow. Among the studies relating to supracondylar humeral fractures, only a few focused on flexion-type fractures.
Treatment options for flexion-type fractures included overhead skeletal traction, manipulation and casting in an extension cast, closed reduction and percutaneous pinning, and open reduction. 2 –5 Closed reduction and percutaneous pinning were often required for more displaced fractures. The techniques used in flexion-type fracture reduction, maintenance of reduction while taking radiographs, and Kirschner wire (K-wire) insertion were completely different from those used in extension-type fractures.
We found the aforementioned problems could be resolved by fracture reduction in the prone position and rotation of the fluoroscopic C-arm around the resting elbow. The purpose of this study was to report the results of a new surgical technique in treating displaced flexion-type supracondylar humeral fractures in children.
Materials and methods
After approval by the institutional review board of the author’s hospital, we retrospectively reviewed the medical records and radiographs of patients with pediatric flexion-type supracondylar humerus fractures that were treated surgically between January 2007 and December 2013. Exclusion criteria included skeletal maturity, extension-type supracondylar fractures, multidirectionally unstable supracondylar fractures, ipsilateral upper extremity fractures, fractures requiring vascular exploration, and follow-up of less than 1 year.
Surgical technique
Patients were anesthetized with endotracheal intubation and placed in the prone position. The injured arm was hung over the edge of the table and supported by a radiolucent arm board and folded towels. 7 The folded towels supported the elbow joint in proximately 45° flexion. The fluoroscopic C-arm was aligned with the long axis of the operation table, next to the patient’s lower extremities. The anteroposterior and lateral views of the elbow were obtained by the rotation of the fluoroscopic C-arm without moving the injured arm (Figure 1).

(a) The patient was placed in the prone position. The injured arm was hung over the edge of the table and supported by a radiolucent arm board and folded towels. The C-arm was aligned with the long axis of the operation table for anteroposterior imaging. (b) The C-arm was rotated to obtain lateral views of the elbow.
The first step was to reduce varus/valgus angulation and medial/lateral translation manually to achieve a proper alignment of the elbow in the anteroposterior view. Overlapping of the fracture fragments was acceptable at this stage. Then, the C-arm was rotated to obtain lateral views of the elbow. Gentle traction was applied to the forearm, and the elbow was extended gradually to reduce the angulation. The whole reduction procedure was monitored by fluoroscopy. Once the fracture was reduced on the sagittal plane, the degree of the elbow flexion was maintained by an assistant (Figure 2). Then, two or three K-wires were inserted percutaneously from the lateral and medial sides to secure the fracture reduction. K-wires were then bent at the skin edge and cut. Dressings were applied to pad the skin. The elbow was immobilized at 40–50° of flexion by a long arm cast (Figure 3).

Reduction maneuver. (a) The injured arm was firmly put on an arm board. (b) Gentle traction was applied to the forearm to reduce the humeral length, and the elbow was extended gradually to reduce the angulation.
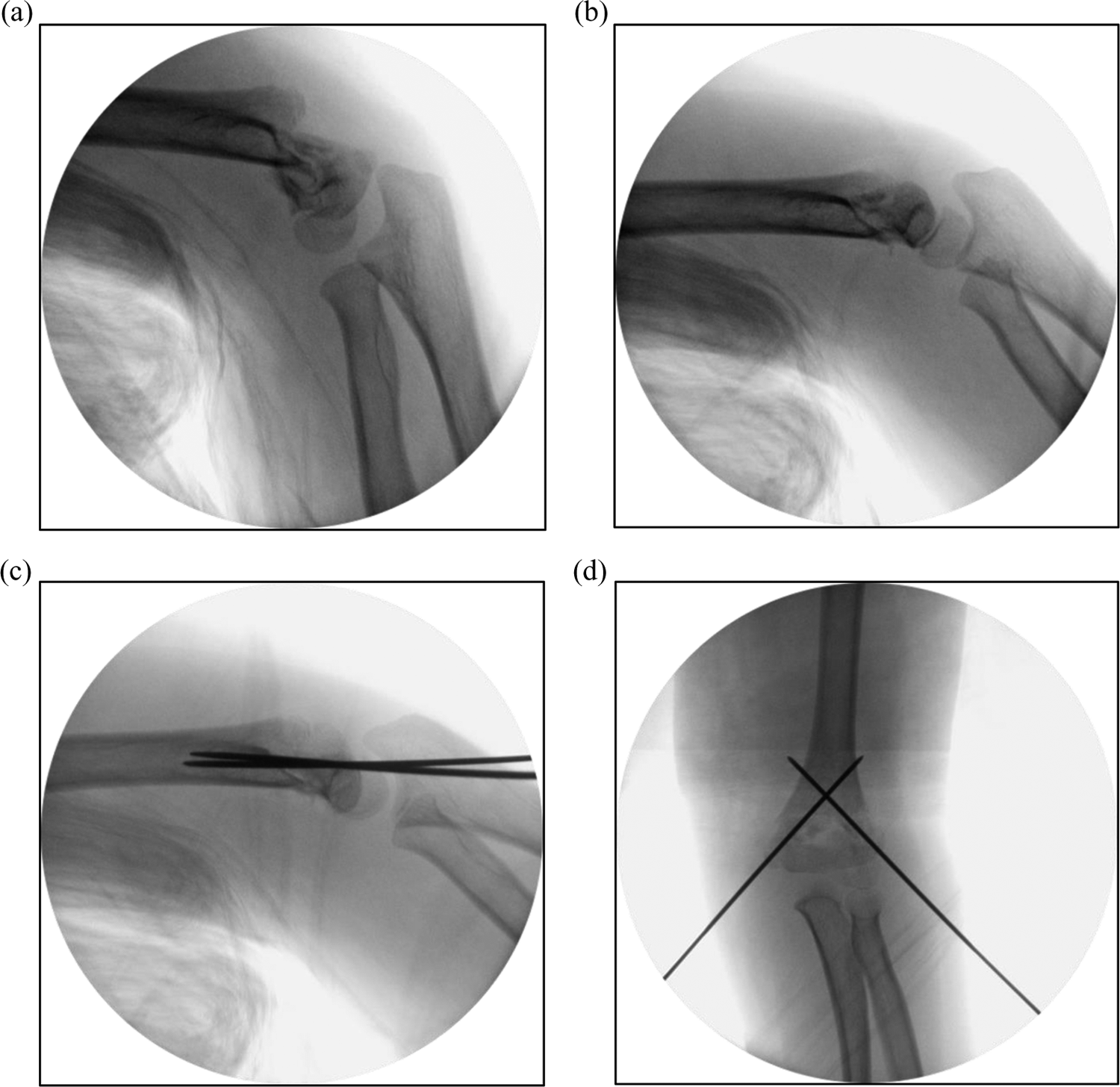
Intraoperative fluoroscopy of fracture reduction and fixation in the prone position. (a) The distal fragment was anteriorly displaced and angulated. (b) The fracture was reduced by elbow traction and extension. (c) Two K-wires were inserted from the lateral and medial sides. (d) The postoperative anteroposterior image demonstrated restoration of the Baumann’s angle. K-wire: Kirschner wire.
After the operation, the patients had clinical and radiographic follow-ups at 2 weeks, 4–6 weeks, 3 months, 6 months, and 1 year. The cast and K-wires were removed after fracture union in the outpatient clinic, usually 4–6 weeks.
Outcome measurements
Range of elbow motion (ROM), carrying angle, and any neurovascular injury were recorded. Radiographic evaluation included the Baumann’s angle on the anteroposterior radiograph and the lateral humerocapitellar angle on the lateral radiograph. 8,9 Intraoperative fluoroscopic images after K-wire placement were compared with the 3-month postoperative radiographs. Because any change in fracture fixation would be clinical significance, whether an increase or decrease in a value, we used absolute value to present the outcome of treatment. According to the criteria reported by Skaggs et al., a loss of reduction was defined by a change in the Baumann’s angle of more than 12°or by the anterior humeral cortex line being unable to intersect the ossification center of the capitellum on the lateral radiograph. 10 Clinical outcomes were assessed using the criteria of Flynn et al., based on the carrying angle and the ROM. 11
Results
Ten children with displaced flexion-type supracondylar humeral fractures were treated in this manner between January 2007 and December 2013. There were three girls and seven boys. All had a unilateral fracture including seven right elbows and three left elbows. The mean age at fracture was 9.5 years (range: 4.8–13.3). The displacement was anterolateral in seven children, anteromedial in two children, and anterior in one child.
All the children were treated on the arrival date or the next morning. Eight children had closed reduction and percutaneous K-wire fixation. The other two children who had preoperative ulnar nerve palsy underwent open reduction because a fracture gap was sill noted after closed reduction. Open reduction through a posterior triceps splitting approach revealed that the ulnar nerve was trapped within the fracture site (Figure 4).

Open reduction through a posterior triceps splitting approach. (a) Intraoperative exposure showed that the ulnar nerve (arrow) was trapped within the fracture site. (b) The ulnar nerve was released from the fracture site and protected.
The mean follow-up period was 17.8 months (range: 12.5–28.6 months). Complete union was achieved in all patients. The K-wires were removed at a mean of 39.1 days (range: 28–58 days). The mean ROM was 136° (range: 115–150°) at the last follow-up. The clinical outcome was excellent in nine patients and poor in one patient (case 8), using the criteria of Flynn et al. (Table 1).
Clinical data of 10 patients with displaced flexion-type supracondylar humeral fractures.
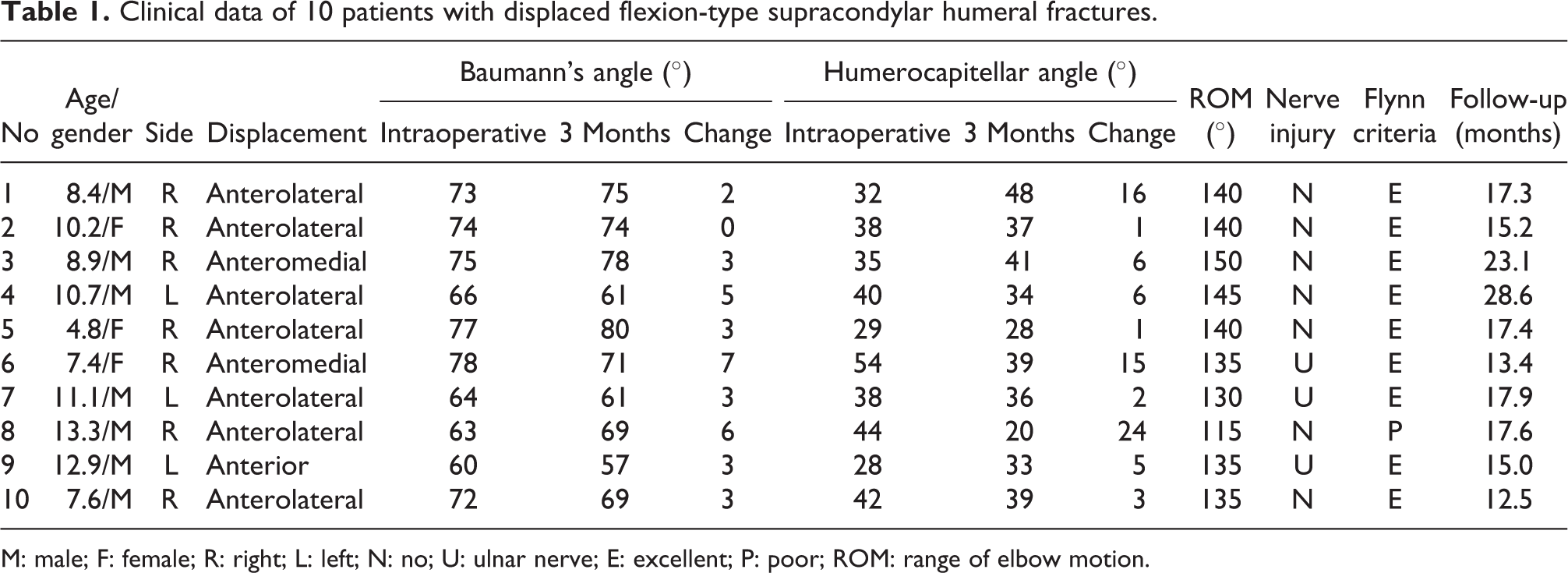
M: male; F: female; R: right; L: left; N: no; U: ulnar nerve; E: excellent; P: poor; ROM: range of elbow motion.
The mean Baumann’s angle was 70.2° (range: 60–78°) immediately after K-wire fixation and 69.5° (range: 57–80°) after 3 months later. The mean change in the Baumann’s angle was 3.5 ± 1.9° (range: 0–7°). The mean lateral humerocapitellar angle was 38° (range: 29–54°) immediately after K-wire fixation and 35.5° (range: 20–48°) after 3 months later. The mean change in the humerocapitellar angle was 7.9 ± 7.4° (range: 1–24°). The intraoperative Baumann’s angle and the lateral humerocapitellar angle were restored to a satisfactory range when compared with the literature. 9,12 One patient (case 8) was regarded as having a loss of reduction due to overcorrection of the distal fragment. The distal fragment became posterior angulation, and the anterior humeral cortex line was unable to intersect the capitellum.
Three of the 10 cases had preoperative ulnar nerve injuries. Two of them showed fracture gap after closed reduction, and the fractures were explored to check the ulnar nerve. The other one fracture was reduced well and only fixed by percutaneous pinning. The three ulnar nerve injuries resolved within 6 months. There were no pin-related nerve injuries. No patient suffered from compartment syndrome or Volkmann’s ischemic contracture.
Discussion
Fracture reduction and fixation could be a technique demanding in flexion-type supracondylar fractures. The reduction could be obtained by traction and extension of the elbow. However, it was hard to maintain the reduction and to obtain lateral fluoroscopic view in the supine position. Therefore, the rate of open reduction was significantly higher in displaced flexion-type supracondylar fractures. Fowles and Kassab reported that open reduction was performed in 3 of 17 patients (17.6%) with flexion-type supracondylar humeral fractures. 3 Mahan et al. even reported that open reduction was performed in 17 of 44 (38.6%) displaced flexion-type supracondylar fractures. 4 We reported a new method to place the elbow firmly on an arm board in the prone position. The C-arm was rotated to obtain anteroposterior and lateral radiographs rather than using rotation of the injured arm. Fracture reduction could be maintained on the arm board, and the position was good for K-wire insertion. The two cases of open reduction were for ulnar nerve exploration rather than fracture reduction.
In extension-type supracondylar humeral fractures, the proximal fragment could have pierced the brachialis muscle. Peters et al. reported a milking maneuver to milk the entrapped brachialis muscle off the proximal fracture spike. 13 In flexion-type fractures, the pierced muscle was the triceps muscle. It was difficult to milk the triceps muscle when the patient was in the supine position. We found the triceps muscle could be milked off the proximal fragment easily in the prone position.
The most common reason for a failed reduction in extension-type fractures was the proximal fragment’s buttonholing through the brachialis muscle. 14,15 The anterior approach was through the torn brachialis muscle to reduce the fracture directly without further destabilizing the fracture. 16 However, in flexion-type fractures, the torn muscle was the triceps. Therefore, the posterior approach in the prone position was the direct method for open reduction, rather than anteromedial or medial approach. 4,17 Triceps splitting via a posterior was relatively simple. 18 The ulnar nerve could also be identified and protected to avoid iatrogenic nerve injury during fracture reduction and fixation.
The incidence of neurologic injury before surgery has been reported between 10% and 20% in supracondylar humeral fractures. 6,19 –22 In flexion-type fractures, the distal fragment displaced and carried the ulnar nerve anteriorly. The ulnar nerve was stretched over the fracture margin of the proximal fragment. The incidence of ulnar nerve injury was significantly higher than that in extension-type fractures. 3,4,6 Babal et al. reported a 16.6% rate of nerve injury associated with flexion-type fractures, and ulnar nerve accounted for 91.3% of all neuropathy. 6 In our study, 3 of 10 patients had ulnar nerve injury before surgery. If fracture reduction cannot be obtained after several attempts at closed reduction, soft tissue interposition, possibly the ulnar nerve, should be suspected. Open reduction was required to ensure that the ulnar nerve is not entrapped in the fracture site.
The drawbacks of this technique were related to the prone position. Placing a patient prone takes longer and is less desirable for airway management. Furthermore, when a patient has concomitant chest or abdominal injuries, the prone position is less desirable. The limitations of this study included the small case number, retrospective case series study design, the lack of radiographs of the noninjured elbow to assess the accuracy of fracture reduction, and the lack of a control group with flexion-type supracondylar humeral fractures treated by other methods to compare the treatment results.
Conclusion
Treatment of flexion-type supracondylar humeral fractures in children in the prone position could be considered as a treatment option. Putting the elbow firmly on an arm board and rotating the C-arm to obtain proper anteroposterior and lateral radiographs facilitated closed reduction and pinning. When reduction could not be achieved or nerve incarceration was suspected, open reduction and nerve exploration could be carried out through the posterior triceps splitting approach without changing position. This technique could be a good alternative when a flexion-type fracture could not be reduced properly in the supine position.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.