
Abstract
The purpose of this study was to evaluate factors that correlated with unsatisfactory short- and long-term outcome in patients who sustained unstable pelvic ring fracture. The study subjects of this study were those of type B and C pelvic ring fractures (82 patients; mean age 54 years). Age, gender, associated injuries, fracture type, Injury Severity Score rating and treatment methods were assessed, and Majeed score for functional outcome and radiographic studies at 1 year after injury (short-term) and at final follow-up (long-term), with mean follow-up of 98 months were analyzed. Significant univariate factors (p < 0.05) were entered in a multivariate logistic regression model to determine the independent predictors of unsatisfactory functional outcome. Univariate analysis showed that fractures of the lower extremity, nerve damage, conservative treatment, and radiological outcome correlated with unsatisfactory short-term functional outcome, while female gender, brain injury, nerve damage, conservative treatment, fracture location at the posterior portion of pelvic ring, radiological outcome, and pure sacroiliac dislocation only for type C fracture correlated with unsatisfactory long-term outcome. Multiple logistic regression analysis identified fractures of the lower extremity (odds ratio (OR): 5.364), conservative treatment (OR: 13.690), and nerve damage (OR: 21.392) as determinants of unsatisfactory short-term functional outcome and nerve damage (OR: 66.926) and poor radiological results (OR: 33.944) as determinant of long-term functional outcome. In patients with unstable pelvic ring injury, fractures of the lower extremity, conservative therapy, and nerve damage influenced short-term functional outcome, while that nerve damage and the pelvic ring displacement over 20 mm negatively affected long-term outcome.
Keywords
Introduction
Pelvic ring fracture causes a variety of anatomical disruptions and potentially significant morbidities. 1,2 An unstable vertical sheer injury or an unstable lateral compression disruption or external rotational instability often requires anatomical reduction with temporary external fixation followed by often technically demanding major surgical intervention, anteriorly and posteriorly. 3 –7 Displaced fractures of the pelvic ring in association with vertically unstable disruption of the osteoarticular junction of the sacroiliac area may also require the management by either external fixation, percutaneous or mini-incisional screw fixation, conventional surgical exploration, or a combination of one or more of these procedures. 8 –14 In this regard, several reports described that malunited fractures of the pelvic ring were associated with poor functional outcome. 1,4,5,11,15 In contrast, some authors described no relationship between functional outcome and major displacement of the pelvic ring. 16,17 Furthermore, another authors reported that various factors might affect functional outcome, such as fracture type, fracture location, associated injuries, treatment methods, and anatomical reduction. 1,6,18 Thus, although prediction of prognosis may be important for patients, the factors that influence to functional outcome remain controversial. In addition, it was reported that the functional outcome of the patients with pelvic ring fracture improved during the first 18 postoperative months. 19 The factors that affect to functional outcome may also vary depending on the period after treatment, however, there was little report to compare the factors that influence to the short- and long-term outcome.
The present study was thus designed to determine the prognostic factors that correlate with short- and long-term unsatisfactory outcome in patients with unstable pelvic ring fracture using multiple logistic regression analysis and compare the factors that influence to the short- and long-term outcome.
Patients and methods
Patients
Between 1991 and 2010, 244 patients with osseous pelvic ring injuries were transferred to our University Hospital after traumatic accidents. They included 151 men and 93 women with a mean age of 58 years (range, 8–94) at injuries. Eighteen (7%) patients were pronounced dead-on-arrival, and 12 (4%) of 42 eventually died within 1 week of admission to the intensive care unit. The remaining 214 patients (133 men, 81 women; mean age, 58 years; range, 8–94) were transferred directly to the orthopedic reconstructive service or transferred to it after 1–13-day admission in the intensive care unit. The type of injury was assessed according to the AO-Orthopaedic Trauma Association (AO-OTA) classification system 20 : 132 patients were classified as type A, 51 as type B, and 31 as type C. The subjects of this study were those of type B and C pelvic ring fractures (82 patients: 62 men, 20 women; mean age 54 years; range, 8–82).
The cause of injury was vehicle crash while driving in 33 patients (40%), pedestrian injury in 17 (21%), fall from height in 12 (15%), and crash by heavy materials in 20 (24%). Associated injuries were brain trauma in 16 patients (20%), pulmonary and cardiovascular injuries in 21 (26%), abdominal injuries in 22 (27%), urinary tract injuries in 13 (16%), spine injuries in 12 (6%), fractures of the upper extremity in 17 (21%), fractures of the lower extremity in 37 (45%), and nerve damage associated with the pelvic ring fracture and/or associated injuries in 14 (17%) including 5 patients with lumbosacral plexus injury, 4 with sciatic nerve injury, 2 with the fifth lumbar nerve injury, and 3 with spinal cord injury (Table 1). We evaluated the physical magnitude of trauma by the Injury Severity Score (ISS) rating.
Demographic data of all patients with unstable pelvic ring fracture.
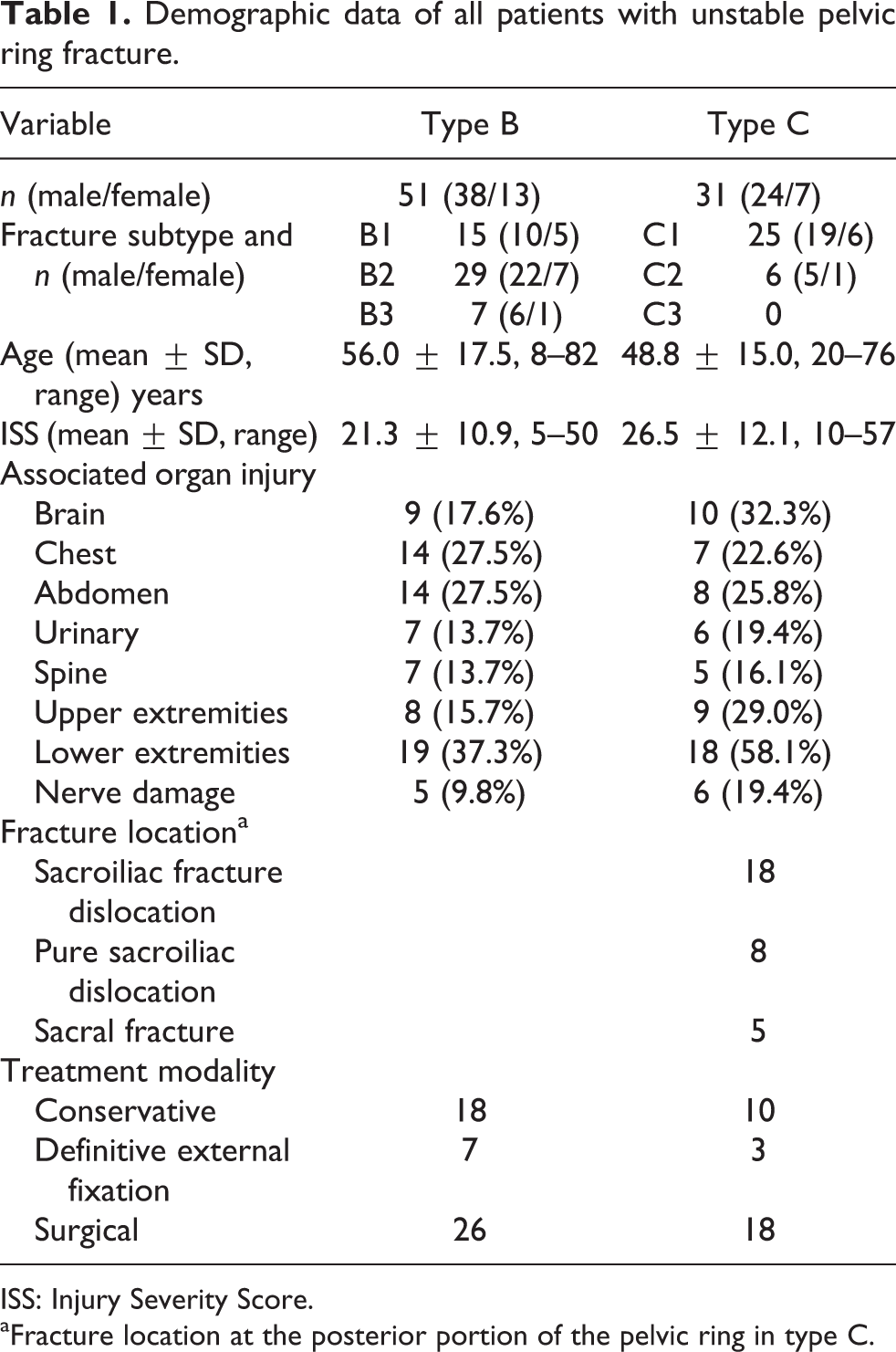
ISS: Injury Severity Score.
aFracture location at the posterior portion of the pelvic ring in type C.
Conservative care, external fixation, and ambulatory rehabilitation
Twenty-eight (34%) patients were placed on a conservative treatment regimen (e.g. sling suspension, sacroiliac bracing, and skeletal traction). Twenty-two (27%) patients were treated with external fixators, 10 of 22 patients were treated definitively for 4–12 weeks using external fixation, and 12 were treated surgically after improvement of physical condition. We used the external fixation assembly (Synthes, West Chester, Pennsylvania, USA) for percutaneous fixation of the pelvic ring, and this was performed immediately in the intensive care unit. Transarterial embolization of the internal iliac artery was performed in 43 (52%) of 82 cases. Ambulation was allowed 4–14 weeks after external fixation, and bony union was followed up by serial radiographs.
Surgical techniques
Forty-four (54%) patients subsequently underwent surgical treatment using various incisional approaches 0–18 days after the trauma. Iliosacral screw fixation or posterior fixation with a sacral plate to prevent osseous disruption (longitudinal fracture) was applied in four patients. Anterior extraperitoneal approach was employed in 38 patients with sacroiliac joint and part of the iliac wing involvement. When the symphysis pubis and superior and/or inferior pubic rami were also disrupted, the Pfannenstiel approach was used in combination with the anterior extraperitoneal approach. The ilioinguinal approach was used in case of major disruption of the pelvic ring with acetabular fracture in two cases. Sacroiliac fracture dislocation and pure sacroiliac dislocation were treated by anterior extraperitoneal approach and reduced and fixed using sacroiliac plate and bone grafting.
Outcome evaluation
Eighty-two patients with unstable pelvic ring fracture were evaluated for clinical and radiological outcome at 1 year after injury (short-term) and at final follow-up (long-term), with minimal follow-up period of 26-month period and mean follow-up of 89 months (range, 26–187). Functional outcome was assessed by the Majeed score, 21 which is a pelvic injury-specific functional assessment divided into seven items: pain, work, sitting, sexual intercourse, standing, gait unaided, and walking distance, with a total score range of 0–100 in order of decreasing disability. Then, we divided the patients into two groups: satisfactory outcome, which included excellent (more than 85 points in Majeed score) and good (70–84 points), and unsatisfactory outcome including fair (55–69 points) and poor (<55). Radiological evaluation 6 at follow-up included overview and inlet plus outlet views of the pelvis. The radiographic outcome was assessed by independent observers as follows: excellent (displacement <5 mm), good (displacement = 5–10 mm), fair (displacement = 11–20 mm), and poor (displacement >20 mm in any direction).
Statistical analysis
Statistical analysis was conducted using the SPSS Statistics for Mac OS version 21 software (IBM, Armonk, New York, USA). Univariate comparisons were performed using the Mann–Whitney U test for continuous variables, such as age and ISS, and Fisher’s exact test for other categorical data. Significant univariate factors (p < 0.05) were then entered in a multivariate logistic regression model to determine the independent predictors of unsatisfactory functional outcome. A p value <0.05 was considered statistically significant.
Results
Table 2 summarizes the univariate factors associated with short-term functional outcomes. A satisfactory functional outcome (both excellent and good) was noted in 52 (63%) patients at 1 year after the injury, and unsatisfactory outcome (both fair and poor) was noted in 30 (37%). Univariate analysis showed significant relationships between unsatisfactory short-term functional outcome and fracture of lower extremity (p = 0.001), nerve damage (p < 0.001), conservative treatment (p < 0.001), and poor radiological outcome (p = 0.002) but not with age, gender, ISS, fracture subtype, such as open book and lateral compression type, and fracture location in type C fracture.
Results of univariate analysis for factors associated with short-term functional outcome.
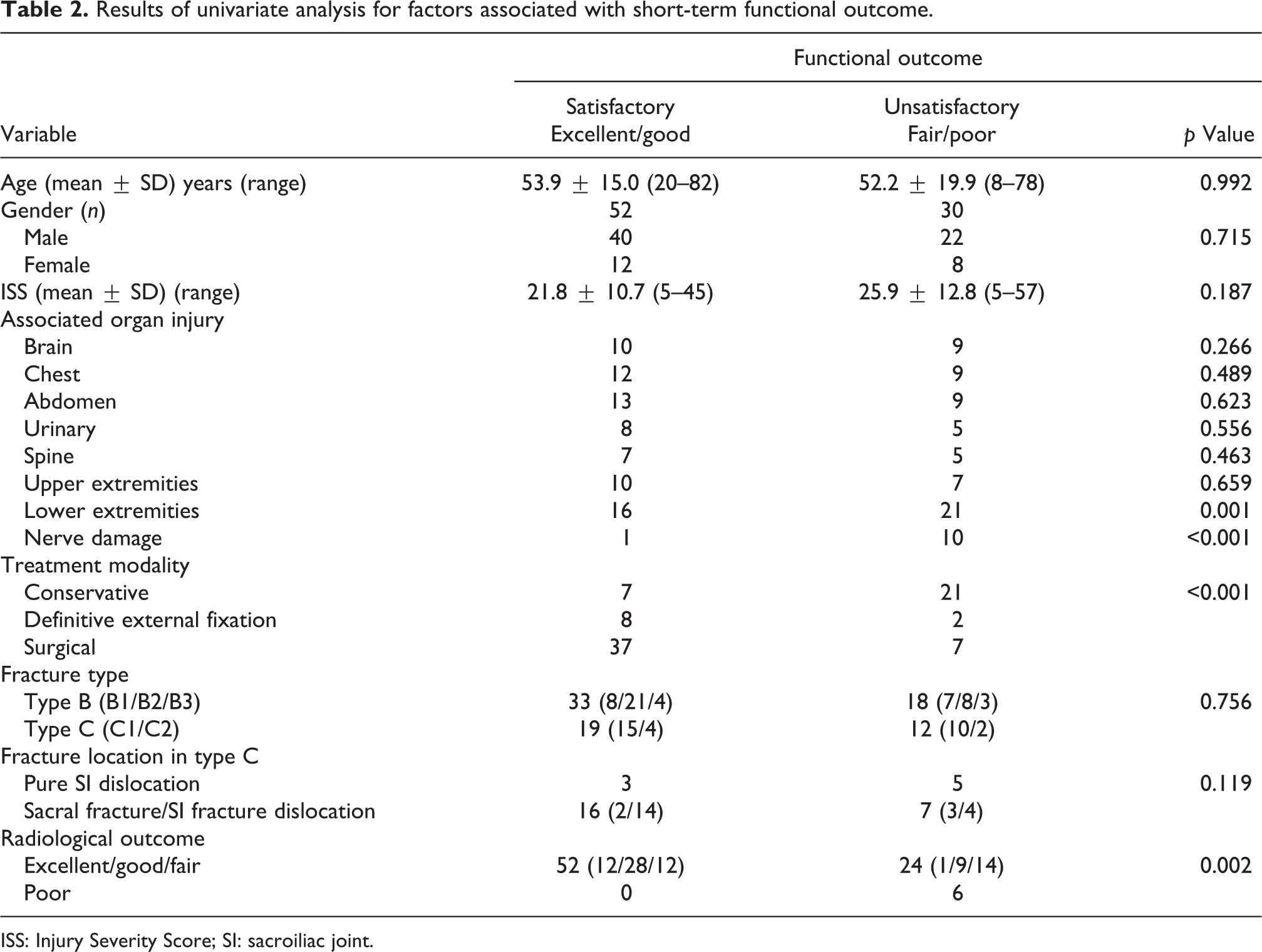
ISS: Injury Severity Score; SI: sacroiliac joint.
Table 3 summarizes the results of univariate analysis of the factors associated with long-term functional outcome. Seventy (85%) patients, including 12 patients of type B and 6 patients of type C, who showed unsatisfactory functional outcome at short-term, achieved satisfactory functional outcome at the final follow-up. Univariate analysis showed significant relationships between unsatisfactory long-term functional outcome and female gender (p = 0.036), brain injury (p = 0.027), nerve damage (p < 0.001), conservative treatment (p = 0.004), pure sacroiliac joint dislocation (p = 0.026), and poor radiological outcome (p = 0.004).
Results of univariate analysis for factors associated with long-term functional outcome.

ISS: Injury Severity Score; SI: sacroiliac joint.
Multiple logistic regression identified the following risk factors for unsatisfactory short-term outcome: fracture of lower extremity (odds ratio (OR): 5.364; 95% confidence interval (95% CI): 1.409–20.425), conservative treatment (OR: 13.690; 95% CI: 3.483–53.798), and nerve damage (OR: 21.329; 95% CI: 1.867–245.128). On the other hand, fracture associated with nerve damage (OR: 66.926; 95% CI: 9.455–473.724) and poor radiological results (OR: 33.944; 95% CI: 3.176–362.754) were risk factors for unsatisfactory long-term outcome (Table 4).
Results of multiple logistic regression analysis for prognostic factors associated with functional outcome.

OR: odds ratio; CI: confidence interval.
Discussion
In the present study, we evaluated short- and long-term outcome in 82 patients with unstable pelvic ring fracture using multivariate logistic regression analysis. Our results showed that concurrent fractures of the lower extremity, conservative treatment, and fractures associated with nerve damage are risk factors for unsatisfactory short-term outcome, whereas nerve damage and the poor radiological outcome, that the pelvic ring displaced over 20 mm, were the determinant of unsatisfactory long-term outcome. Majeed score, 21 which was used to evaluate functional outcome, is a functional grading scale specific for pelvic injury and was designed to determine the functional status about certain aspects of life. This grading scale is divided into seven categories, which include pain, work, sitting, sexual intercourse, walking aids, gait unaided, and walking distance. Although this scoring system is simple, it provides consideration to the most important aspects that can be limited after pelvic injury, though it does not include specific findings at physical examination or radiological outcome, making it suitable for assessment of functional outcome in an individual patient, not as an outcome based on findings at physical examination or at radiographs. Majeed 19 also stressed the superiority of assessment of functional outcome compared with anatomical results and reported in serial observations of 42 patients with pelvic ring fracture treated by external fixation improvement during the first 18 months followed by stabilization of functional outcome. Our results were in agreement with the above study: in 18 patients who showed unsatisfactory outcome at 1 year (short-term), functional outcome improved later during further follow-up. We considered the reason of this outcome improvement that some patients with fractures of the lower extremity had poor muscle power of the lower extremities and pelvic girdle at 1 year after injury, but this improved gradually. We considered that the associated fractures of lower extremity and conservative therapy in these patients had a negative impact on the short-term outcome, as reflected by the results of multivariate logistic regression analysis. In other words, these factors negatively influenced walking ability in the first year after injury. Thus, we stress the importance of proper management of fractures and muscle injury of the lower extremity, simultaneously with treatment of unstable pelvic ring disruptions for a better outcome.
Traumatic disruption of the pelvic ring should be treated for the following important anatomic features: horizontally round configuration of the ring, femoro-sacral longitudinal weight bearing axis, the ‘keystone’ structure of the sacrum, and symphysis pubis that ‘anchors’ the oval ring. 22 Surgical treatment of unstable pelvic ring fractures, which was associated with satisfactory short-term outcome in the present study, was recommended by many authors to provide anatomical reduction of the pelvic ring. 10,22 Several reports described that the anatomical reduction was significantly associated with the functional outcome, 4,6,11,18,23,24 however, several authors reported that there was no relationship between functional outcome and anatomical reduction. 15,16,17 In this regard, our results demonstrated that the pelvic ring with displacement over 20 mm related to poor functional outcome. The pelvic ring displacement, especially the vertical displacement, influenced to the sitting balance and the gait abnormality caused by the difference of the length of lower extremity, however, our results showed that the displacement within 20 mm had no influence to the long-term functional outcome. We believe disrupted pelvic ring alignment must be reconstructed surgically, but the strict anatomical reduction is not necessarily needed.
On the other hand, our results demonstrated that nerve damage affected both the short- and the long-term outcomes. Rommens and Hessmann 12 reported that the neurological recovery rate was worse in patients with type C fracture than in those with type B because of the more severe injury of neurological structures in the former group at the time of injury. Several reports described that anatomical reduction and rigid fixation with nerve decompression might reduce the rate of neurologic damage. 4,25,26 However, others indicated that the course of the nerve damage was not affected by satisfactory reduction, 6,15,27 and that permanent neurological deficit might aggravate the functional outcome, even if the reduction of the pelvic ring fracture is anatomic. 4,17 Our results showed that nerve damage was the significant determinant of long-term functional outcome, probably because such injury negatively influenced pain, work, and walking within the Majeed score, which depend on the recovery of nerve damage. In addition, recovery of nerve damage did not correlate with anatomical reduction in our cases. Thus, utmost care should be practiced in the management of patients with unstable pelvic ring disruptions associated with injury of the lumbosacral plexus and sciatic nerves, in order to improve neural function.
In conclusion, fracture of lower extremity, conservative therapy, and nerve damage showed significant relationship with unsatisfactory short-term functional outcome. Nerve damage and the pelvic ring displacement over 20 mm were significantly associated with unsatisfactory long-term functional outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.