
Abstract
Purpose:
To investigate the efficiency of simultaneous correction of moderate to severe hallux valgus deformity and adult-type pes planus.
Methods:
Twenty cases of moderate to severe hallux valgus complicated with adult-type pes planus in 19 consecutive patients (15 (79%) women, 4 (11%) men; mean age: 44.50 ± 17.13 years, mean follow-up duration: 31.30 ± 17.02 months) were included. Medial calcaneal sliding osteotomy was performed to correct hindfoot valgus, whereas treatments of hallux valgus were case dependent.
Results:
The mean postoperative hallux valgus angle, intermetatarsal angle, hindfoot alignment angle, and hindfoot alignment ratio were 8.40 ± 5.29°, 4.20 ± 2.54°, 3.09 ± 2.92º and 0.41 ± 0.17, respectively. Although a hallux varus deformity occurred as a postoperative complication in one case (5%), there were no cases of postoperative recurrence.
Conclusion:
Simultaneous correction of hallux valgus and pes plano-valgus using medial calcaneal sliding osteotomy is an effective technique that reduces recurrence of hallux valgus and increases satisfaction in patients with moderate to severe hallux valgus deformity complicated with adult-type pes planus accompanying hindfoot valgus.
Introduction
Hallux valgus, a deformity that is known to affect many middle-aged and older women, is occasionally complicated with pronation deformity or pes planus. 1,2 The causes of hallux valgus can be classified into external and internal. Footwear is the principal external contributor to the hallux valgus development. 3 The internal factors include genetics, hypermobility of the tarsometatarsal joint, general ligamentous laxity, pronation deformity and weakness of the intrinsic muscles. 4
Recurrence of hallux valgus after corrective surgery is reported by many authors as the most common complication. 5 –8 The causes of the recurrence can be classified into surgical and patient risks. The choice of an inappropriate surgical technique is the main surgical factor for recurrence, 9 while the patient risks include systemic diseases such as rheumatoid arthritis or gout, hypermobility of the first metatarsophalangeal joint, and inappropriate choice of shoes or braces after operation. Although there is no report on whether adult-type pes planus may impact the recurrence rate of hallux valgus after operation, hindfoot valgus may pronate the foot, resulting in excessive pressure on the first metatarsophalangeal joint. 4 Therefore, we hypothesized that, if these two conditions are not corrected together, there will be a greater risk of recurrence. Our primary aim was to evaluate the outcomes of surgical correction of moderate to severe hallux valgus complicated with pes plano-valgus. To this end, we retrospectively reviewed the data of patients who underwent medial calcaneal sliding osteotomy with osteotomy of the metatarsal and/or phalangeal bone for hallux valgus correction.
Materials and methods
Patient selection
The study included 19 consecutive patients (20 cases) with moderate to severe hallux valgus (hallux valgus angle (HVA): >20°, first to second intermetatarsal angle (IMA): >11°) complicated with pes plano-valgus (Meary’s angle: <−4°, hindfoot alignment angle (HAA): >10°) who underwent simultaneous correction of these conditions from January 2008 to December 2014. Preoperative and postoperative assessments of all patients were conducted at the outpatient clinic by a single surgeon. This retrospective study was approved by our institution’s ethical review committee. The duration of postoperative follow-up was at least 1 year. The exclusion criteria were (1) age <18 years, (2) systemic inflammatory conditions such as rheumatoid arthritis, and (3) history of trauma that could have caused foot deformity.
Chief complaints included bunion pain and intractable plantar keratosis accompanied by pain in the second metatarsal head, both caused by moderate to severe hallux valgus, and posteromedial sole pain or discomfort upon weight bearing caused by pes plano-valgus. These symptoms did not improve with conservative treatment such as using foot aids (toe spacer, insole, second metatarsal pad).
Four participants (21%) were male and 15 (79%) were female, with the average age of 44.50 ± 17.13 (18–66) years and the mean follow-up period of 31.30 ± 17.02 (18–78) months. The left and right feet were affected in 15 (79%) and 5 (21%) cases, respectively. In 9 (45%) out of the 20 cases, operations to correct other deformities on the same foot were performed. In particular, Weil osteotomy was performed in five cases (25%) in order to remove plantar keratosis accompanied by second metatarsal head pain. The modified Broström technique was used to repair the anterior talofibular ligament in one case (5%). The S.E.R.I. (simple, effective, rapid, inexpensive) osteotomy 10 was done for correction of bunionette in two cases (10%). Finally, the Kidner technique combined with Strayer procedure was employed to remove the accessory navicular bone and reattach the posterior tibial tendon in one case (5%) (Table 1). No patients had equinus deformity of the ankle joint of the affected foot.
A statistical description of the cohort (N = 20 cases in 19 patients).

PCMO: proximal chevron metatarsal osteotomy; MBO: modified Broström operation; S.E.R.I.: simple, effective, rapid, inexpensive technique.
Treatment protocol
Preoperative standing antero-posterior (AP), lateral, and hindfoot alignment radiographs of the foot were taken and correlated with the patient’s clinical symptoms in order to determine the appropriate surgical approach. Of the 20 moderate to severe hallux valgus cases, 13 (65%) were treated with proximal chevron metatarsal osteotomy (PCMO) and simultaneous Akin procedure (for correcting hallux interphalangeal angle rather than HVA and first to second IMA). Five cases (25%) were treated with PCMO only, and in two younger patients (10%) with less extreme IMAs, the Scarf procedure was used. Medial calcaneal sliding osteotomy was utilized in all the cases to correct hindfoot valgus due to adult-type pes planus. Although the degree of medial sliding after calcaneal osteotomy depends on the degree of hindfoot valgus, medial sliding of 1 cm was typically considered appropriate. Twelve operations (60%) were performed under general anesthesia and eight (40%) under epidural block. Medial calcaneal sliding osteotomy was performed with the tourniquet on and a large number of surgical drapes under the buttock of the patient in order to keep the affected limb elevated in the semi-lateral position. The periosteum was dissected and calcaneal osteotomy was performed perpendicular to the lateral aspect of the calcaneus 1 cm posteriorly from the subtalar joint. The calcaneus was shifted 10 mm medially. Two 5.0 cannulated screws were fixed firmly from the calcaneal tuberosity crossing the osteotomy site. The surgical drapes were then removed, the patient was placed into the supine position, and hallux valgus correction was subsequently carried out (Figures 1 and 2). Below-knee cast immobilization was maintained for 4–6 weeks after the operation, and weight bearing was excluded during this time. The cast was removed afterwards, an AP radiograph was taken to determine the status of union, and the patient was encouraged to slowly start walking. All operations and follow-up examinations were performed by a single surgeon (JSS) in the same manner.

A 44-year-old female with severe hallux valgus deformity and pes planus. The hallux valgus angle and the intermetatarsal angle were 44° and 16°, respectively (a). Excessive hindfoot valgus deformity with the hindfoot alignment angle of 27.7° and a negative value of the hindfoot alignment ratio (b). A lateral radiograph showing the pes planus deformity (c).

At 15 months postoperatively, radiography showed successful hallux valgus correction (a) and hindfoot valgus correction (b). A lateral radiograph demonstrating no significant change in the first metatarsocuneiform angle and calcaneal pitch angle (c).
Evaluation of surgical outcome
In order to determine the extent of hallux valgus correction, HVA and IMA were measured preoperatively and during the final follow-up using standing foot AP radiographs. In addition, distal metatarsal articular angle (DMAA) was measured to determine the congruity of the metatarsophalangeal joint. DMAA reflects the relationship between the distal articular surface of the first metatarsus and the longitudinal axis of the first metatarsus. The Hardy and Clapham’s method of measurement of relative metatarsal length 11 was used to detect the shortening of the first metatarsal bone after the operation. A line was drawn between the medial point of the talonavicular joint and the most lateral point of the calcaneocuboidal joint in the standing AP radiograph of the foot. From the point where the axis of the second metatarsal bone crossed this line, another line was drawn toward the center of the first and second metatarsal bones. Two circular sectors were then drawn using the two lines as radii. The distance between the two sectors was measured to compare the lengths of the first and second metatarsal bones.
In order to evaluate the extent of pes planus correction after medial calcaneal sliding osteotomy, talonavicular coverage angle (TNCA) in standing foot AP radiographs was measured. Talo-first metatarsal angle (Meary’s angle) and calcaneal pitch angle (CPA) were also measured on lateral radiographs. In order to examine the extent of correction of hindfoot valgus, HAA formed by the axes of the tibia and the calcaneus and hindfoot alignment ratio (HAR) defined as the ratio of medial calcaneal width to its total width 12 were measured in the hindfoot alignment view (Figure 3). Clinical results were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) hallux metatarsophalangeal–interphalangeal (MTP-IP) and ankle–hindfoot scales, 13 which included 40 points for pain, 45 for function, and 15 for alignment, for a total of 100. Furthermore, cases with complications were followed and analyzed to determine how the complications impacted the clinical results. The Wilcoxon test as implemented in SPSS version 19 was used for the statistical analysis of all variables, and a p value <0.05 was considered to represent statistical significance.

Measurements of the extent of hindfoot valgus. HAA: hindfoot alignment angle; HAR: hindfoot alignment ratio.
Results
HVA in the AP radiographs improved from 33.85 ± 8.77° preoperatively to 8.40 ± 5.29° postoperatively, with an average correction of 25.45 ± 3.48° in 19 cases (excluding one case with a hallux varus complication). This extent of correction was statistically significant (p = 0.03). The IMA improved from 14.80 ± 2.26° preoperatively to 4.20 ± 2.54° postoperatively, and the DMAA from 33.85 ± 10.84° preoperatively to 10.20 ± 10.16° postoperatively. Both variables showed statistically significant reductions (p = 0.01). The average reduction of the first metatarsal bone, assessed based on the comparison with the second metatarsal bone, was 2.74 ± 2.44 mm. The TNCA measured in AP radiographs was 27.67 ± 10.69° before the operation and 15.78 ± 9.39° after it, with a statistically significant reduction (p = 0.001). The preoperative Meary’s angle and CPA measured in lateral radiographs were −13.15 ± 5.00° and 12.86 ± 3.73°, respectively, compared to −10.94 ± 5.07° and 13.53 ± 5.23°, respectively, after the operation. A trend toward recovery was observed, but neither measurement showed a statistically significant improvement (p = 0.63).
The HAA measured in the hindfoot alignment view was 16.17 ± 5.56° preoperatively and 3.09 ± 2.92° postoperatively, with a statistically significant improvement (p = 0.01). The HAR also showed a statistically significant improvement (p = 0.01) from 0.14 ± 0.06 to 0.41 ± 0.17. The hallux MTP-IP AOFAS score for clinical result analysis significantly increased from an average of 61.42 ± 2.63 to 88.32 ± 9.30 (p = 0.005) and the ankle–hindfoot AOFAS score significantly increased from of 68.21 ± 3.84 to 89.41 ± 6.24 (p = 0.005). This indicates the improvement in clinical symptoms, including pain reduction and increased activity. Also grossly, hindfoot valgus correction could be identified by assessing the too many toe sign disappearance (Figure 4). The changes in the radiographic and clinical measurements can be found in Table 2.
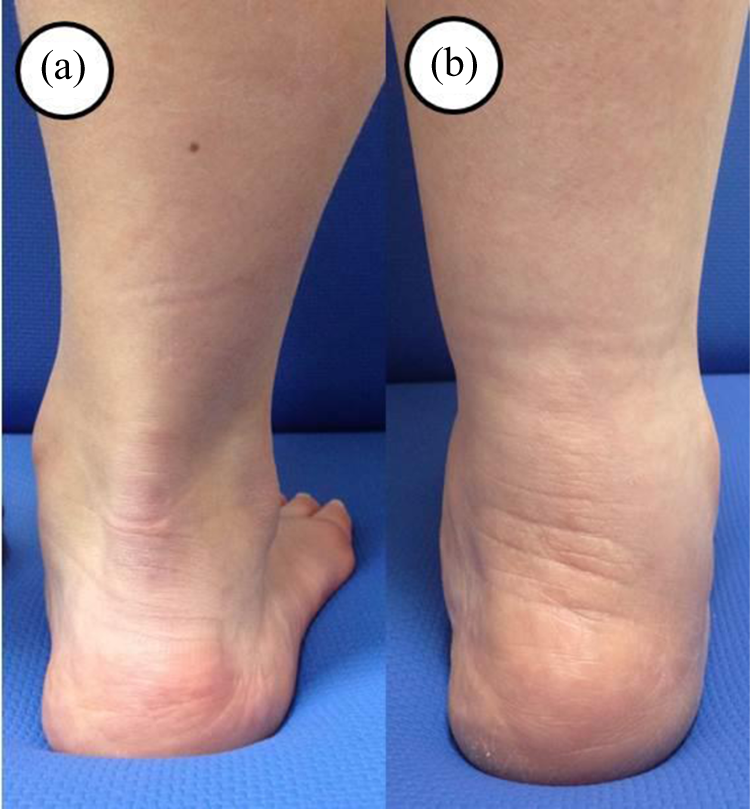
Preoperative hindfoot valgus (a) was corrected and the too many toe sign was disappeared at postoperative 1 year (b).
A statistical description of the preoperative and postoperative radiological and clinical variables (N = 20 cases in 19 patients).
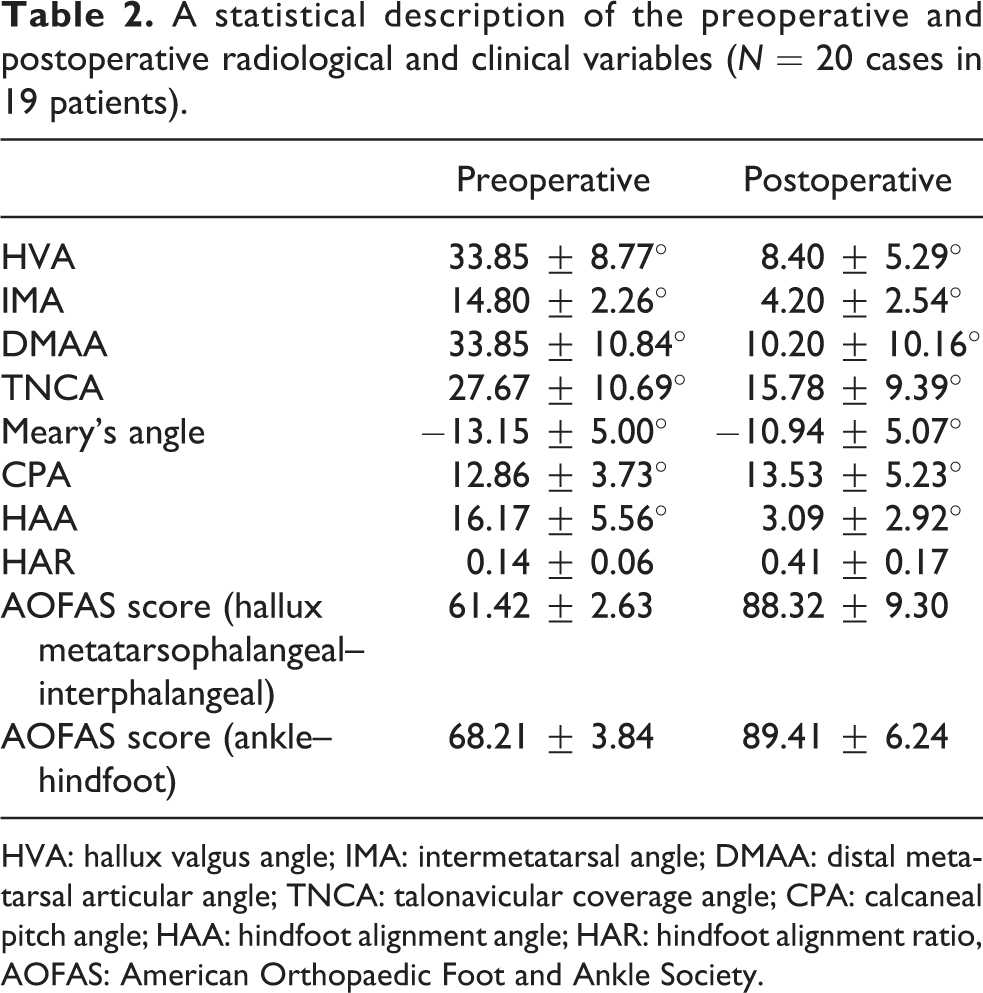
HVA: hallux valgus angle; IMA: intermetatarsal angle; DMAA: distal metatarsal articular angle; TNCA: talonavicular coverage angle; CPA: calcaneal pitch angle; HAA: hindfoot alignment angle; HAR: hindfoot alignment ratio, AOFAS: American Orthopaedic Foot and Ankle Society.
There was one case (5%) with a hallux varus complication caused by overcorrection of hallux valgus. However, no recurrence of hallux valgus was observed among the patients, and no evidence of inflammation or malunion was present.
Discussion
The association of pes planus with the development of hallux valgus is controversial. 2,4,14 –25 Mann and Pfeffinger 14 reported that the etiologies of adult-type pes planus and hallux valgus are unrelated and did not influence the success rate of the operation. However, the presence of adult-type pes planus, as mentioned above, causes pronation of the foot and hindfoot valgus. Pronation of the foot causes a longitudinal rotation of the first ray that places the axis of the MTP joint in an oblique plane relative to the floor. In this position, the foot appears to be less able to withstand the deforming pressures exerted on it by either shoes or weight bearing. 1,16 –25 Furthermore, excessive lateral pressure on the distal part of the proximal phalanx in the first metatarsophalangeal joint may induce hallux valgus. The severity of hallux valgus can be exacerbated by previous history of this disease or presence of the causative factors described above. 4,16
If the age and pathology of the patient are properly taken into consideration, a simultaneous correction of the forefoot and hindfoot can be achieved and maintained by combining medial sliding calcaneal osteotomy for the correction of hindfoot valgus deformity with proximal metatarsal correction. Based on this concept, we assumed that it may also be possible to obtain better results by correcting hallux valgus and hindfoot valgus at the same time.
For correction of adult-type pes planus complicated with functional abnormality of the posterior tibial tendon, medial calcaneal sliding osteotomy employed in this study or lateral column lengthening (open-wedge osteotomy performed on the proximal calcaneocuboid joint followed by tricortical bone grafting) can be used. If the symptoms are severe, subtalar or triple arthrodesis is another option. Medial calcaneal sliding osteotomy is a technique that restores laterally displaced attachment of the Achilles tendon while reducing the antagonism/counteraction of the Achilles tendon against the flexor digitorum longus, thus reestablishing the tension of the tendon and the ligament of the medial hindfoot. In addition, the technique can reduce the distance between the point where the hindfoot contacts the ground and the longitudinal axis of the lower limb, thereby reducing the torque on the subtalar joint. The exact therapeutic mechanism for lateral column lengthening is unknown, but this technique increases the tension of the plantar ligament, fascia, and peroneus longus tendon through tricortical bone grafting. The secondary windlass effect from this procedure contributes to restoring the medial longitudinal arch as well as correcting the forefoot and hindfoot valgus. Although lateral column lengthening is effective in correcting the deformity, 26 it may induce arthritis in the calcaneocuboid joint. Therefore, it was excluded from this study as the subjects were middle-aged and older adults.
Cao and colleagues 27 reported that medial displacement calcaneal osteotomy with reconstruction of the posterior tibial tendon insertion on the navicular bone was an effective treatment for flexible flatfoot with symptomatic accessory navicular and that this approach was associated with excellent clinical outcomes and correction of the deformity. This signifies that, in treatment of pes planus with pronation deformity, realigning the foot by correcting the hindfoot valgus is more important than simply repairing the posterior tibial tendon. However, to the best of our knowledge, there is no report on the positive results of correcting pes planus with medial calcaneal sliding osteotomy combined with hallux valgus correction in cases of pes planus caused by symptomatic posterior tibial tendon functional abnormality coexisting with hallux valgus.
All the cases included in this study showed moderate to severe hallux valgus deformity with the HVA >30° and the IMA >13°. The HAA ranged from 10° to 27.7°, and the HAR ranged from negative values to a maximum of 0.2. Accordingly, we recommend performing medial calcaneal sliding osteotomy simultaneously with osteotomy to correct hallux valgus in cases of adult-type pes planus complicated with hindfoot valgus.
Hypermobility of the first ray could be an important factor for considering the Lapidus procedure as one of the surgical options. However, we did not utilize the Lapidus procedure because we did not expect that forefoot surgery alone would properly correct the problems caused by hindfoot valgus deformity. Furthermore, the Lapidus procedure is associated with a risk of nonunion and shortening of the first metatarsal bone.
Overcorrection of hallux valgus led to hallux varus in one case (5%). This patient refused further treatment and is being currently followed up. Nevertheless, it is remarkable that there was no recurrence of hallux valgus in any of the 20 cases. Since the follow-up period of this study was <2 years, further research is warranted to investigate long-term effects of the treatment.
The main limitation of this study is the lack of comparison with results of corrective osteotomy for hallux valgus performed without correcting the hindfoot in cases with hallux valgus with similar severity complicated with adult-type pes planus. The retrospective design of the study is another limitation.
In conclusion, simultaneous correction of hallux valgus and pes planus using medial calcaneal sliding osteotomy is an effective and safe technique that potentially improves hindfoot alignment, brining benefit to the longevity of the forefoot surgery in patients with moderate to severe hallux valgus deformity complicated with adult-type pes planus accompanying hindfoot valgus. The results of the present investigation could be used in the development of future randomized controlled trials or prospective cohort studies that focus on simultaneous correction of hallux valgus and concomitant adult-type pes planus.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.