
Abstract
Purpose:
The aim of this meta-analysis is to examine the efficacy and safety of intra-articular tranexamic acid (TXA) when compared to intravenous (IV) route.
Methods:
The literature search was conducted using PubMed, Cochrane Library, MEDLINE, EMBASE and China National Knowledge Infrastructure (CNKI). All randomized controlled trials evaluating the effectiveness of topical route and IV route of TXA administration were included.
Results:
Eight randomized clinical trials comprising of 857 patients were included in this analysis. We found no statistically significant difference in terms of total blood loss, drain output, transfusion requirement, thromboembolic complication, tourniquet time and surgical duration.
Conclusion:
Topical TXA has a similar efficacy to IV-TXA in reducing total blood loss, drain output, transfusion rate and haemoglobin drop without any increase in thromboembolic complications.
Introduction
Total knee arthroplasty (TKA) is one of the most effective treatments of end-stage knee arthritis. The number of patients who will be requiring TKA likely increases substantially in the near future due to our increasing ageing population. 1 However, this surgery may lead to considerable intraoperative and post-operative blood loss due to large exposed cancellous bone. 2,3 This may sometimes require allogenic blood transfusion, which has its own adverse effects, such as transmission of infectious disease, immune sensitization, transfusion-related reactions, intravascular haemolysis, transfusion-induced coagulopathy and renal failure. 4,5 Various measures have been tried to decrease the bleeding and subsequently, the transfusion requirements, such as preoperative autologous donation, controlled hypotension, cell saver, regional anaesthesia and use of erythropoietin and antifibrinolytics. 6,7
The antifibrinolytics include aprotinin, tranexamic acid (TXA) and ∊-aminocaproic acid, which have different mechanism of action. 8 TXA is a synthetic derivative of amino acid lysine and a competitive inhibitor of plasminogen activation and thus interferes with fibrinolysis. 9 It is widely used in different surgical procedures such as cardiac surgery, upper gastrointestinal bleeding and post-partum haemorrhage. 10 –13 Multiple reports have shown the effectiveness of TXA to control bleeding in knee arthroplasty. 14 –17 However, its route of administration is still a matter of debate. 18 –25 Intravenous (IV) route of administration can lead to various systemic complications such as deep vein thrombosis (DVT)/pulmonary embolism (PE). 26 –29 Topical application of TXA has been proposed to decrease these adverse effects. The available studies on this topic have shown mixed results, hence the need for this meta-analysis.
The aim of this meta-analysis is to compare the effectiveness and safety of topical and IV route of TXA administration in TKA.
Materials and methods
This study was conducted in accordance with the guidelines described in accordance with the guidelines described in the Cochrane handbook for systematic review and meta-analysis of interventions and also met the reporting guidelines outlined in PRISMA.
Criteria of eligibility
Studies selected were randomized controlled trials (RCTs) comparing topical TXA with IV-TXA in primary TKA that fulfilled the following inclusion criteria: (1) studies enrolled adult patients undergoing a primary TKA regardless of the aetiology; (2) full text of each article was available and (3) conference abstracts were included if sufficient data were provided. Patients on anticoagulation agents and patients with bleeding disorders were excluded.
Search strategy
Two of the authors searched the PubMed, MEDLINE, EMBASE, China National Knowledge Infrastructure (CNKI) and the Cochrane Library, to retrieve all available relevant articles, using the terms tranexamic acid, Cyklokapron, antifibrinolytic, topical, intra-articular, knee arthroplasty and knee replacement. The bibliographies of identified articles, including relevant reviews and meta-analyses, were manually searched for potential eligible reports. No language restrictions were set during search process. The following websites were searched to identify unpublished and ongoing studies: Current Controlled Trials (www.controlled-trials.com); Centre Watch (www.centerwatch.com); US Clinical Trials (http://clinicaltrials.gov); Trials Central (www.trialscentral.org); the UK National Research Register (http://www.nihr.ac.uk); the Cochrane Central Register of Controlled Trials (CENTRAL) (http://www.thecochranelibrary.com).
Extraction of data
Each retrieved citation was reviewed by two authors. Most citations could be excluded on the basis of information provided by their respective title or abstract. Otherwise, the complete manuscript was obtained and carefully scrutinized by the two reviewers. Any disagreements were resolved with consensus.
Outcome measurements
The primary outcomes were total blood loss and maximum fall in haemoglobin. The secondary outcomes were blood loss from drain, number of patients who received blood transfusion, number of blood units transfused, thromboembolic complications, tourniquet time and surgical duration.
Study quality
All studies were reviewed by two independent reviewers using the Jadad score. 30 A scale of 0 (very poor) to 5 (rigorous) was used to assess the methodological strength of studies. Any conflicts were resolved by consensus. Studies with a Jadad score of 1 were considered poor, scores of 2 were considered adequate and a score of 3 or higher was considered a high quality.
Statistical analysis
The meta-analysis programme of the Cochrane Collaboration (Review Manager 5.3) was utilized for quantitative analysis of data, using the inverse variance statistical method and either a fixed or random effects model, depending on the absence or presence of statistical heterogeneity, accordingly. Dichotomous outcome data were summarized using risk ratio (RR) and 95% confidence intervals (95% CIs). Continuous outcomes were summarized using the weighted mean differences and respective 95% CIs.
The results of each component study as well as the summarized estimate of effect size were presented graphically as forest plots. Statistical heterogeneity across all component studies was investigated with Cochran’s chi-square test (Q test) and I 2 test. Significance was set at 0.1 for the Q test. When using I 2 test, heterogeneity was interpreted as absent (I 2: 0–25%), low (I 2: 25.1–50%), moderate (I 2: 50.1–75%) or high (I 2: 75.1−100%).
Funnel plots for main outcomes of interest (total blood loss and Hb drop) were generated to evaluate potential publication bias.
Results
A total of 321 abstracts and titles with 857 patients were reviewed. Of these, eight satisfied the eligibility criteria and were included in the analysis. A flow chart is provided in Figure 1. One study 18 had four IV groups depending on the dosage and another study 23 had two topical groups depending on the dosage and method of TXA administration. These groups were analyzed separately, resulting ultimately in 12 component studies for the analysis. The characteristics of the study are summarized in Table 1. The quality of the studies was assessed using the Jadad scoring system (Table 2); four trials were high-quality RCTs with scores no less than three points.

Flow chart showing the selection of studies.
Characteristics of included study.
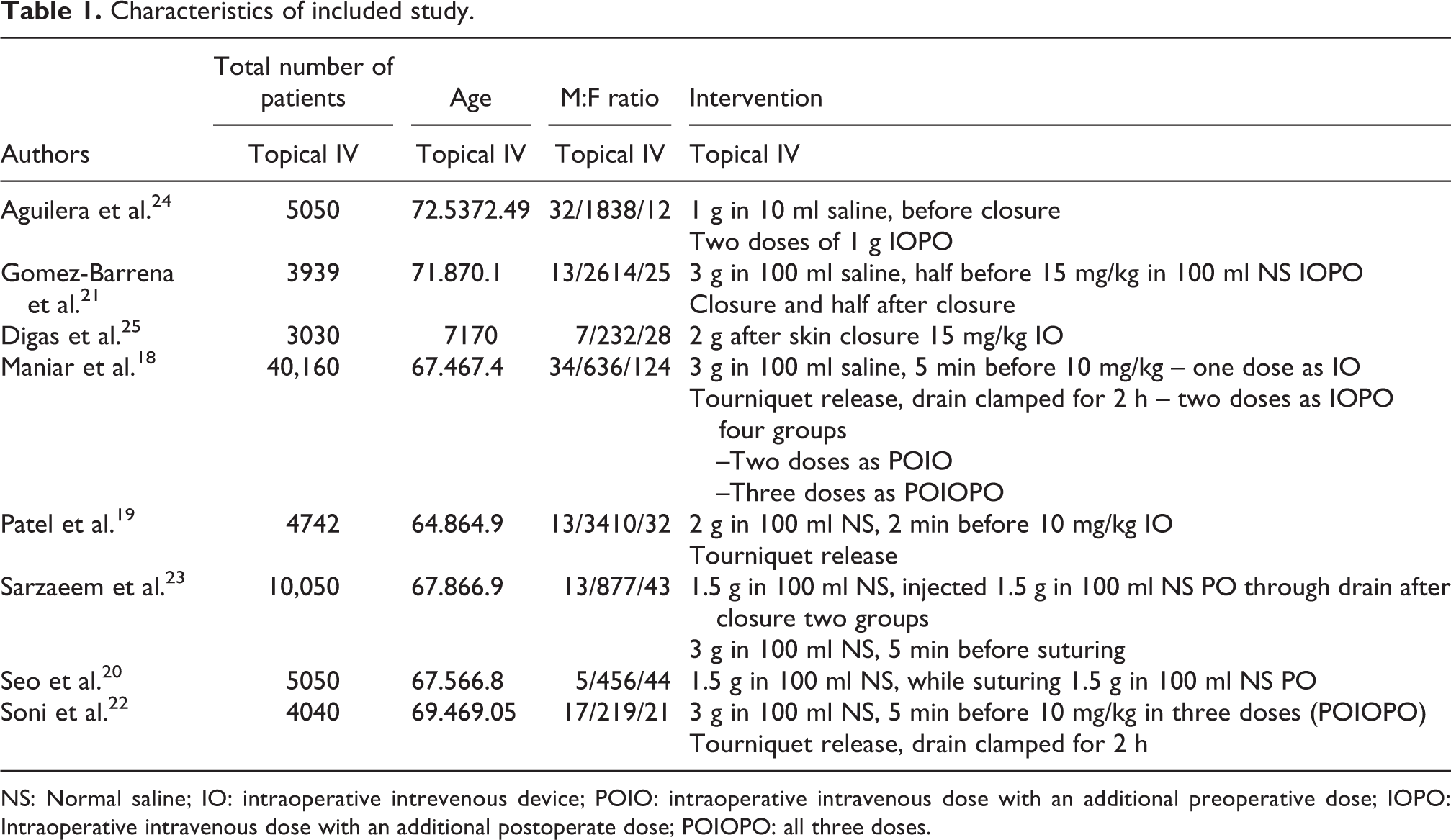
NS: Normal saline; IO: intraoperative intrevenous device; POIO: intraoperative intravenous dose with an additional preoperative dose; IOPO: Intraoperative intravenous dose with an additional postoperate dose; POIOPO: all three doses.
The Jadad assessment of quality of studies.a

aAll answers scored 1 for yes and 0 for no.
Blood loss
Total blood loss data were provided by 12 component studies. There was no statistically significant difference in total blood loss in the topical group compared with the intra-articular group (Mean difference (MD): 1.64, 95% CI: 109.98–113.27, p = 0.98). However, a significantly high heterogeneity was present between the studies (I 2 = 94%, p < 0.001). Seven component studies provided data on blood loss from drain. There was no statistically significant difference in between the two groups (MD: 9.59, 95% CI: −49.71–68.88). A significantly high heterogeneity was present between the studies (I 2 = 88, p < 0.00001; Figure 2).

Forest plot of blood loss.
Change in haemoglobin
Change in haemoglobin was mentioned in seven component studies. The use of topical route leads to increased fall in Hb (MD: 0.50, 95% CI: 0.04–0.96). However, this was not statistically significant. There was a high heterogeneity between various studies (I 2 = 94%, p < 0.00001; Figure 3).
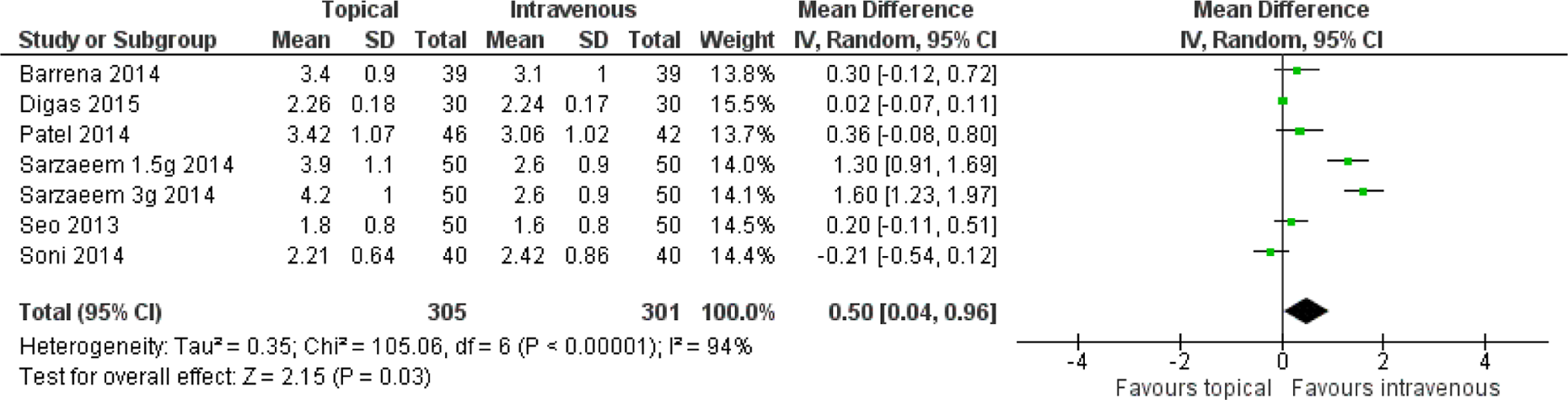
Forest plot of change in haemoglobin.
Blood transfusion
All component studies provided data on the number of patients transfused with allogenic blood. There was no significant difference in between the two groups (RR: 1.06, 95% CI: 0.74–1.50, p = 0.96) in the absence of statistical heterogeneity (p = 0.25, I 2 = 19%). Five component studies presented data on the number of units transfused. There was no significant difference in terms of the number of units transfused (RR: 5.10, 95% CI: 0.36–71.34, p = 0.23). Heterogeneity between the studies was significantly high (I 2 = 83%, p = 0.0006) (Figure 4).
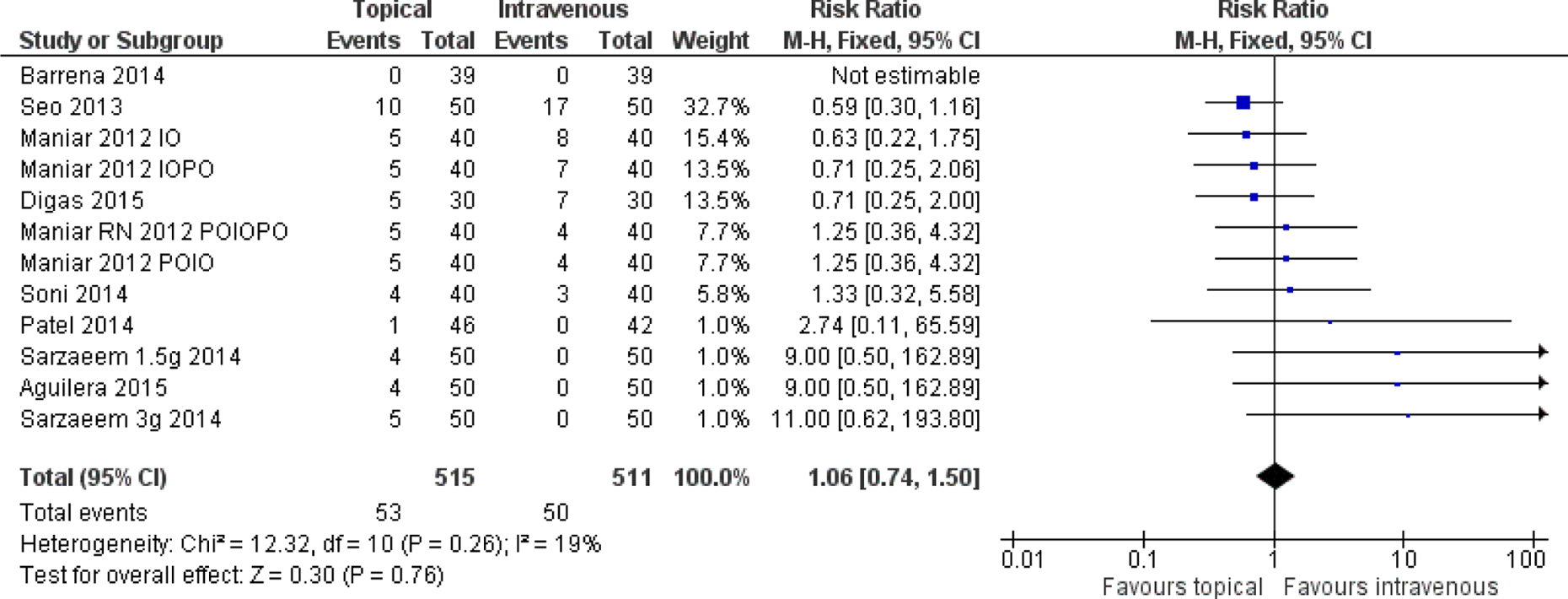
Forest plot of blood transfusion.
Thromboembolic complications
Eleven component studies provided data on thromboembolic complications. Out of these, eight studies have no thromboembolic complications and hence they couldn’t be analyzed. There was no statistically significant heterogeneity between the studies (p = 0.37, I 2 = 0%). The data analysis revealed no statistical difference in the risk of developing thromboembolic complications based on three studies (RR: 2.25, 95% CI: 0.59–8.59, p = 0.23; Figure 5).

Forest plot of thromboembolic complications.
Tourniquet time
Eight component studies reported tourniquet time. There was no statistically significant difference between the two groups (MD: 1.00, 95% CI: 0.72–2.72, p = 0.15).
Surgical duration
Six studies reported on surgical duration. There was no statistically significant difference between the two groups (MD: 1.98, 95% CI: 0.23–4.20, p = 0.08).
Discussion
The efficacy of TXA to reduce bleeding in knee arthroplasty has been well established in the literature. The route of administration can be IV, intramuscular (IM), oral and intra-articular. 31 Maximum plasma concentration of TXA is reached within 5–15 min after IV injection, 30 min after IM injection and 2 h after oral tablets. 32,33 Compared with the IV-TXA in TKA, topical TXA was considered to be of less systemic absorption and better local effect. Thus, a growing number of studies have focused on the topical application of TXA in TKA and the results are promising. 22 Our meta-analysis showed that, in overall comparison, there was no statistically significant difference in total blood loss, drain output, transfusion requirements and thromboembolic complications when comparing topical TXA and IV-TXA in primary TKA
The potential mechanism and advantage of topical application of TXA into the surgical field is to directly target the site of bleeding just before wound closure, but after operative haemostasis has been achieved, thus attenuating the marked increase in local fibrinolysis associated with a release of the tourniquet. Such inhibited local fibrinolytic activity will help to prevent fibrin clot dissolution and increase its volume and strength at the surgical surfaces and therefore, enhance microvascular haemostasis.
Most intravenous regime of tranexamic acid requires it to be given in a minimum of two doses. Maniar et al. noted that a single regimen of TXA cannot be recommended as the most effective regimen. 18 In his study, local intraoperative application produced reduction in total blood loss when compared with the control, whereas a single intravenous intraoperative dose did not. Soni et al. concurred with Maniar et al. and concluded that intra-articular regimen of TXA is as effective as three doses IV regimen in preventing blood loss without any difference in thromboembolic complications. 22 It is easier for surgeons to administer a single topical TXA dose rather than the two IV doses often administered by the anaesthesiologist.
Post-operative anaemia can be an important problem that could lead to increased morbidity and mortality and an increased duration of stay in the hospital. There was a tendency in our meta-analysis of more Hb drop with topical TXA as compared to intravenous group. However, this difference did not reach statistical significance. Seo et al. and Sarzaeem et al. in their study noted decreased post-operative Hb drop with intravenous administration as compared to intra-articular administration. 20,23
More blood units were transfused in the topical group (27/219) than in the intravenous group (14/219), but this difference did not reach statistical significance. Out of all the studies included in this analysis, only one study 25 comprised of all the blood units transfused in intravenous group, that is, 14 units in 30 patients. If this study was excluded from the analysis, then there was statistically significant risk of blood transfusion in the topical group. Wind et al. compared the two forms of TXA and reported decreased transfusion requirements with both forms of TXA compared to placebo. 34 Similarly, Ishida et al. reported intra-articular administration of TXA not only decreased blood loss but also decreased joint swelling after TKA. 35
The right dosage and appropriate method of TXA application are still not clear. Most authors use a dose, ranging from 1.5 g to 3 g in 100 ml Normal Saline (NS). Jang et al., in their retrospective study about intra-articular injection of TXA, found that reduction in haemoglobin levels was significantly greater in placebo group than in 1500 mg TXA group and the 3000 mg group, with a significant difference between the two TXA groups, so they suggested a dose-dependent effect of TXA on blood loss. 36 Panteli et al. in their meta-analysis noted that 2 g was more effective in terms of transfusion requirements. 37 The method of topical application varies among the studies. There is no consensus on the most appropriate method of topical application. Sarzaeem et al. compared two different methods of topical TXA administration, through drain or irrigation of the knee joint. They found that intra-articular administration of TXA through drain decreased drainage volume by 45% and irrigation of the knee joint with TXA decreased it by 14% when compared to the control group. 23
In spite of the significant literature support for the use of TXA in TKA, many common medical conditions, including renal insufficiency, history of previous DVT and cardiac and cerebrovascular disease, may preclude the use of IV-TXA at the time of surgery. These same contraindications may not apply to the topical use of TXA, perhaps due to the presumed delay in systemic absorption after application into the knee joint. Wong et al. measured plasma concentration of TXA after intravenous injection and topical administration. 38 They found plasma levels of TXA following topical administration were significantly (70%) less than an equivalent dose of intravenous injections. Topical TXA may be helpful in patients with contraindications to systemic TXA, as absorption from the joint is clinically negligible. 38
TXA carries a risk of thrombosis, although this has not been proven clinically. We concur with other authors regarding the safety of TXA irrespective of the chosen route. Our analysis did not demonstrate increased risks of DVT or PE. A total of four documented cases of DVT were seen out of 857 patients. In one study, Seo et al. 20 reported three cases of DVT were in the topical group and no cases in the intravenous group. However, this study also reported two cases of DVT in the placebo group. There was no case of PE in any of the included studies. Nonetheless, uncertainty still remains because of the difference of DVT and PE screening. Many studies have evaluated only symptomatic DVT and PE. The number of asymptomatic DVT and PE events needs to be evaluated as well. Furthermore, the small number of patients involved also prevented us from drawing an accurate conclusion. Considering the above factors, these findings require further confirmation.
Some authors have reported that combining intravenous and topical TXA is more effective than either regimen used alone. 39 The topical application combined with povidone–iodine solution or epinephrine has also shown promising results in terms of lower blood loss and higher post-operative haemoglobin levels. 40,41,42
The main strength of our meta-analysis is that it included only RCTs. However, there are several limitations. First, the dosage and the method of application vary in each study. Second, there was significant heterogeneity between the various studies. Third, there was no uniformity on tourniquet application and drain clamping.
Conclusion
In conclusion, topical administration of TXA had comparative efficacy to intravenous administration on reducing total blood loss, drain output, blood transfusion and haemoglobin drop, without any increase in thromboembolic complications. However, studies with more uniform dose and technique of application are required to establish the most effective regimen and technique.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.