
Abstract
Introduction:
Conventional non-vascularized bone grafts as well as vascularized bone grafts are used to treat scaphoid non-union (SN). Due to limited available studies, the field of application using both grafts for SN still remains controversial. The aim of this study was to evaluate a treatment algorithm for the use of both vascularized versus non-vascularized bone grafts based on clinical outcomes and quality of life (QoL) to improve the level of evidence.
Materials and Methods:
Based on a retrospective cohort study, including 28 patients with vascularized and 45 patients with conventional bone grafts, functional parameters, radiological outcome, Mayo-wrist-score, and QoL by SF-36 were applied to statistically compare the outcome of these two techniques.
Results:
Time between last procedure or trauma and study group scaphoid reconstruction was almost double in the vascularized bone grafting group. Comparable union rates were achieved with vascularized as well as non-vascularized bone grafts. Significant differences were observed between both groups for grip strength and radial-ulnar active range of motion. Further functional outcomes, radiological outcomes as well as QoL were found similar for both techniques in patients with surgical union.
Discussion and conclusions:
In order to achieve comparable and appropriate treatment results, vascularized bone grafts are recommended for patients with delayed treatment, impaired scaphoid vascularity, and revision surgery. Even in preselected, complex cases, the results are comparable to conventional grafts, which are the basis for further patient education and approve the powerful role of surgical angiogenesis of vascularized bone grafts.
Keywords
Introduction
The scaphoid is the most vulnerable carpal bone accounting for more than 60% of carpal fractures due to its biomechanical properties. 1 Scaphoid non-union (SN) occurs with an incidence of 5% of all scaphoid fractures. 2 If left untreated, SN leads to scaphoid non-union advanced collapse and osteoarthritis in more than 90% of cases after 10 years. 3 –5 Various non-vascularized and vascularized cortico-spongious bone grafts are employed to treat SN. 6 –8 Recently, vascularized bone grafts, such as the 1,2-intercompartmental supraretinacular artery pedicled vascularized bone graft (1,2-ICSRA-VBG), 9 the free femoral condyle, 10 –12 and the free iliac crest bone graft 13 have become increasingly popular in the treatment of SN. Here, treatment principles include surgical angiogenesis due to optimized graft perfusion and stability due to safe internal fixation. 14 –17 However, treatment strategies for SN remain controversial: conventional non-vascularized bone grafting, such as cortico-spongious iliac crest non-vascularized bone graft (IC-NBG), 18 –21 is still widely performed. These are technically easier compared to vascularized bone grafting requiring microsurgical techniques and show relatively satisfactory results. 13,22 While various techniques are validated and widely accepted, patient selection and individual management still remain controversially discussed. To date, literature focusing on a direct comparison of vascularized versus non-vascularized cortico-spongious bone grafts for the treatment of SN is limited. 23 Here, we present a retrospective analysis of SN patients treated with vascularized or with non-vascularized cortico-spongious bone graft in a single center over a 13-year period. Functional and radiologic outcomes as well as quality of life (QoL) were analyzed to gain more evidence for individualized indications and surgical strategy.
Methods
Selection of study samples
After approval of the local ethics committee (no. 837.074.11 [7616], Mainz, Germany), all medical records of patients with SN between January 1997 and November 2010 were retrospectively reviewed. Patients who met the inclusion criteria were selected for further analyses. The inclusion criteria were (a) SN diagnosed by computed tomography (CT) or X-ray, (b) treatment by vascularized (1,2-ICSRA-VBG) or non-vascularized (IC-NBG) bone grafting, and (c) adequate postoperative follow-up showing osseous union or non-union on CT scans or conventional X-ray.
Indication of bone grafts and diagnosis of surgical union
Vascularized bone grafting was employed in cases with avascular proximal pole or proximal pole non-union and in secondary cases after failed scaphoid reconstruction using non-vascularized bone grafts. Non-vascularized, standard cortico-spongious bone grafts were used in patients without impaired scaphoid vascularity and large osseous defects after SN resections or humpbeck deformity. Small defects treated with cancellous bone from the distal radius during primary procedure were not included in this study because of the different bone morphological features and healing conditions compared to cortico-spongious grafts. All surgeries were performed according to the methods previously reported. 9,18
Postoperative radiologic follow-up
Postoperatively, radiological examinations were performed at 6, 12, and 16 weeks and at the latest follow-up. X-rays were performed in posterior–anterior, lateral, and Stecher views. CT was employed if the X-ray film had any doubt for union/non-union. Surgical union was diagnosed by a team of two hand surgeons and an independent radiologist. Cast immobilization was performed for at least 6 weeks. After that, the cast was removed if union was diagnosed, or cast immobilization was finished at the latest at 16 weeks postoperatively with or without scaphoid union.
Follow-up and clinical data extraction
Postoperative data were collected at the latest follow-up. Hand strengths and active range of motion (AROM) were measured in both injured and uninjured (contralateral) hands. Jamar grip strength and key pinch strength were used to evaluate hand strength. Jamar grip strength was measured with a Jamar hand dynamometer (Sammons Preston, Bolingbrook, Illinois, USA), and key pinch strength was measured with a Jamar pinch gauge (B&L Engineering, Tustin, California, USA). AROM for extension-flexion (E-F) and radial-ulnar (R-U) abduction were applied to evaluate the motion of hand. AROM were measured with a goniometer (Prestige Medical, Northridge, California, USA). The Mayo wrist score was used to assess hand function. The scapholunate angle and the Nattrass carpal height ratio were assessed by X-ray as previously described. The German version of Short Form 36 Item Health Survey (SF-36) 24 was used to access QoL.
The following baseline data were extracted from medical records: age at the latest scaphoid reconstruction, gender, body mass index, delay between injury and the last scaphoid reconstruction, numbers of scaphoid operations, smoking history, injured hand (dominant/non-dominant), adjunctive wrist denervation therapy, type of internal fixation, length of operation, immobilization time, scapholunate angle, and Nattrass carpal height ratio. 25
Statistical analysis
Normally distributed continuous variables were presented with mean ± SD or N (%) and analyzed by Student’s t-test or Wilcoxon rank sum test. Categorical variables were compared using χ 2, Fisher’s exact test, or Wilcoxon rank sum test. All statistical analyses were two-sided end, and the value of p < 0.05 was considered significant. Statistical analyses were performed using SPSS 17.0 (SPSS Inc., Chicago, Illinois, USA).
Results
Patient characteristics
Of 181 patients diagnosed with SN in our center between February 1997 and December 2010, 39 patients were treated with vascularized (1,2-ICSRA-VBG) cortico-spongious bone grafts, and 11 patients were lost in follow-up; 52 patients were treated with non-vascularized cortico-spongious (IC-NBG) bone grafts, and 7 were lost in follow-up. Altogether, 73 patients were included in the present study, and their clinical outcomes were further analyzed.
Demographic and clinical characteristics of the two studied groups are summarized in Table 1. Patients in the vascularized graft group were significantly older when compared to patients after non-vascularized bone grafting (29.8 years vs. 27.0 years; p = 0.037). The time between the last scaphoid reconstruction and the study procedure was almost double in the vascularized bone grafting group (54.0 vs. 22.9 months; p < 0.001). In the non-vascularized graft group, fewer patients received adjunctive posterior interosseous nerve denervation (6.6 vs. 35.7%; p = 0.003); and the mean length of operation was obviously shorter (78 vs. 112 min; p < 0.001).
Demographic and clinical characteristic of all patients.a

BMI: body mass index; OP: operation; PIN: posterior interosseous nerve.
aValues are described as N (%) or mean (range).
Union rate
Osseous union was predominantly achieved in both groups. Union was observed in 21 patients (75.0%) after vascularized bone grafting, whereas 37 patients (82.2%) in the non-vascularized treatment group showed uneventful osseous healing (p = 0.555).
Functional outcome
Jamar grip strength, key pinch strength, E-F AROM, and R-U AROM were evaluated compared to the contralateral hand and between groups. The results are summarized in Table 2. Comparison to the contralateral uninjured side revealed that hand function (Jamar grip strength, E-F AROM, and R-U AROM) was markedly impaired after vascularized as well as non-vascularized bone grafting (Table 2). Significant differences were observed between the two groups for grip strength (vascularized vs. non-vascularized bone grafting; 35.8 ± 11.7 vs. 42.2 ± 9.1 kg; p = 0.031) and R-U AROM (vascularized vs. non-vascularized bone grafting; 57.0 ± 17.2 vs. 68.1 ± 14.0 degrees; p = 0.007). However, when results were normalized to contralateral values (ratio: injured/contralateral values) and were assessed, differences were not found to be significant.
Functional outcomes of patients with surgical union.a

E-F: extension-flexion; R-U: radial-ulnar; AROM: active range of motion; CL: contralateral; Postop/CL: postoperational value/contralateral value.
aValues are described as N (%) or mean ± SD.
The Mayo score of vascularized graft group and of non-vascularized graft group was 71.7 ± 18.3 and 77.0 ± 8.5, respectively. Differences were not significant (p = 0.128).
Radiological outcomes
Scapholunate angle and Nattrass Carpal height index of patients with surgical union were assessed (Table 3). No significant change (p > 0.05) was found within (preoperative vs. postoperative) or between groups.
Anatomical integrity of patients with surgical union.a
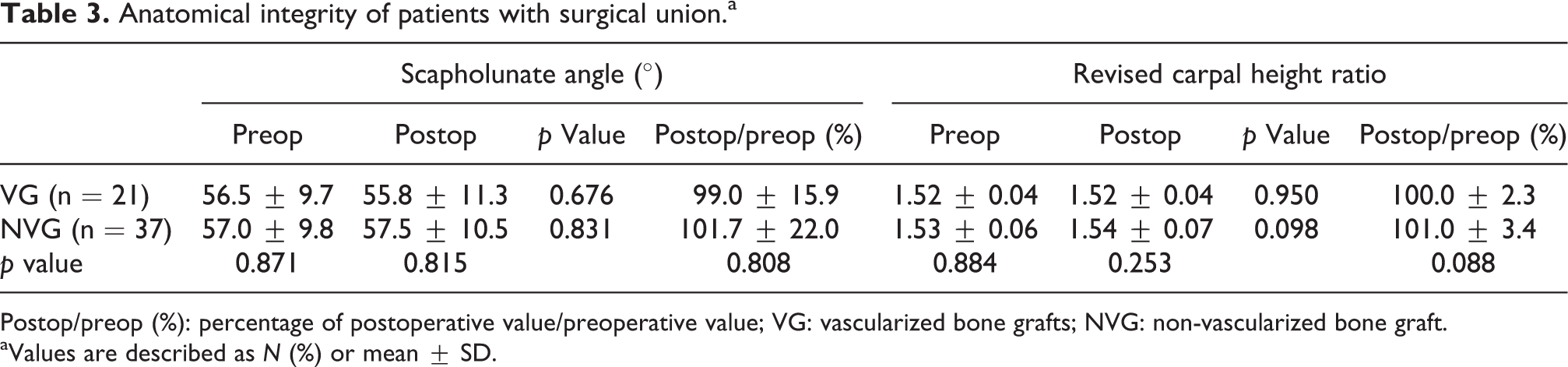
Postop/preop (%): percentage of postoperative value/preoperative value; VG: vascularized bone grafts; NVG: non-vascularized bone graft.
aValues are described as N (%) or mean ± SD.
No difference in the QoL
The postoperative QoL was measured by SF-36. Physical summary (PCS) and mental summary (MCS) of patients with surgical union were evaluated. No significant difference were observed for neither PCS (p = 0.387) nor MCS (p = 0.686) between two groups (Figure 1).

Comparison of QoL of union patients between vascularized (n = 21) and non-vascularized (n = 37) groups. QoL was described by PCS and MCS summaries. QoL: quality of life; PCS: physical summary; MCS: mental summary.
Discussion
Major aims of scaphoid reconstruction are restoration of the physiologic anatomy with osseous consolidation and good function as well as prevention of posttraumatic arthritis. 8,26 The present study revealed that similar outcomes can be achieved with both vascularized and non-vascularized transplants for SN, despite the fact that patients in the vascularized bone grafting group were older and the onset of treatment was significantly longer post trauma. Non-vascularized grafts, for example, IC-NBG, are widely applied as a standard technique, providing relatively large volumes and grafts that are relatively easy to harvest with good biomechanical properties. 18,27,28 As well, conventional bone grafts from the distal radius have been demonstrated to be an alternative to the IC-NBG in the past two decades. Mirly et al. 29 approved the volume of non-vascularized bone grafts from the distal radius to be sufficient for most hand and wrist surgeries, even though the volume is less compared to grafts from the iliac crest. Also, the biomechanical properties of both osseous grafts have been shown. 30 Nevertheless, conventional grafts only provide reduced angiogenetic potential and thus have limitations compared to their vascularized counterparts. Vascularized bone grafts from the distal radius, such as the 1,2-ICSRA-VBG, additionally apply the principle of surgical angiogenesis and therefore may increase the likelihood of osseous healing when compared to conventional bone grafts from iliac crest, 11,17,31 especially in patients with poor scaphoid perfusion. Satisfactory osseous union rates have been documented for this graft. 15,32 In contrast, positioning and internal fixation of pedicled, vascularized bone grafts are more difficult in order not to compromise transplant perfusion. While there is evidence of studies focusing on either vascularized or non-vascularized grafts for SN, studies directly opposing vascularized and conventional grafts for the treatment of SN are scarce as the basis for a therapeutic algorithm. To the best of our knowledge, only two studies have been published so far. Bao et al. 33 demonstrated that vascularized bone grafts from Lister’s tubercle are more effective to treat SN than IC-NBG. However, given the small sample size (13 patients), the strength of their conclusion is limited compared to the sample size in this study. Braga et al. 23 found similar union rates and functional outcomes in a prospective study comparing 35 patients treated with the 1,2-ICSRA-VBG and 45 patients with the IC-NBG. Likewise, we found similar union rates, functional outcomes, and QoL comparing these bone grafts. However, the initial condition of the scaphoid was worse in the group with vascularized bone grafting, when compared to patients treated with conventional bone grafts, because the period from injury to last operation was longer (54.0 months in the 1,2-ICSRA-VBG group and 22.9 months in the IC-NBG group). Against this background, it is well-known that the perfusion and osteogenic potential of scaphoid fragments decreases over time, which impairs surgical union and requires additive stimulation by angiogenesis. 3,34 Since equal outcomes could be achieved in patients who per se have worse scaphoid conditions, our data suggest that vascularized bone grafts provide improved angiogenesis and osteogenic potential and can therefore be regarded as more effective when compared to non-vascularized bone grafts. Limitations of both surgical techniques were observed in terms of functional outcome. The grip strength and the AROM of both groups significantly maintained lower levels than the contralateral, uninjured hand (75.9 –89.3%), although surgical union and anatomical integrity were achieved. However, outcome scores, such as the Mayo-wrist-score and SF36 score, were still satisfactory.
The present study has some remarkable limitations. First, cohort allocation based on the study design was retrospective, and different grades of SN have been the basis for either vascularized or non-vascularized grafts. Second, 11 (28.2%) and 5 (13.5%) patients from 1,2-ICSRA-VBG and IC-NBG groups were lost in follow-up, respectively. Third, the concrete osseous healing time has not been recorded due to the long intervals between follow-ups.
Conclusion
Comparable union rates and functional outcome can be achieved with vascularized as well as non-vascularized bone grafts for the treatment of SN in this retrospective study. A therapeutic algorithm for the surgeon and patient education should include vascularized bone grafts to be preferable for patients with delayed treatment, revision surgery, and impaired scaphoid vascularity to benefit from surgical angiogenesis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by a scientific grant of the BG Trauma Center Ludwigshafen and Tübingen gGmbH, Ludwigshafen, Germany.