
Abstract
Purpose:
This study compared the efficacy of continuous interscalene block (CISB) and subacromial infusion of local anesthetic (CSIA) for postoperative analgesia after open shoulder surgery.
Methods:
This randomized, prospective, double-blinded, single-center study included 40 adult patients undergoing open shoulder surgery. All patients received a standardized general anesthetic. The patients were separated into group CISB and group CSIA. A loading dose of 40 mL 0.25% bupivacaine was administered and patient-controlled analgesia was applied by catheter with 0.1% bupivacaine 5 mL/h throughout 24 h basal infusion, 2 mL bolus dose, and 20 min knocked time in both groups postoperatively. Visual analog scale (VAS) scores, additional analgesia need, local anesthetic consumption, complications, and side effects were recorded during the first 24 h postoperatively. The range of motion (ROM) score was recorded preoperatively and in the first and third weeks postoperatively.
Results:
A statistically significant difference was determined between the groups in respect of consumption of local anesthetic, VAS scores, additional analgesia consumption, complications, and side effects, with lower values recorded in the CISB group. There were no significant differences in ROM scoring in the preoperative and postoperative third week between the two groups but there were significant differences in ROM scoring in the postoperative first week, with higher ROM scoring values in the group CISB patients.
Conclusion:
The results of this study have shown that continuous interscalene infusion of bupivacaine is an effective and safe method of postoperative analgesia after open shoulder surgery.
Keywords
Introduction
Shoulder surgery has been shown to result in severe postoperative pain. Pain relief after shoulder surgery has a positive effect on postoperative rehabilitation by accelerating functional return including range of motion (ROM) and muscle power besides early mobilization. Severe complications such as deep venous thrombosis and osteoporosis can be prevented and the hospitalization period is also shortened. In addition, aggressive pain relief is one of the major determinants of patient satisfaction and comfortable recovery in the early postoperative period. 1
Interscalene blockage has been demonstrated to provide successful anesthesia and postoperative analgesia in several shoulder surgical procedures. Therefore, rehabilitation of patients can be started in the early postoperative period. 2 Subacromial (bursal)/intra-articular infiltration analgesia has been used as an effective postoperative analgesia procedure. 1,3 In this study, a comparison was made of the efficacy of continuous interscalene block (CISB) and subacromial infusion of local anesthetic (CSIA) for postoperative analgesia after open shoulder surgery.
Methods
This randomized, prospective, double-blinded, single-center study was conducted in accordance with the most recent version of the Helsinki Declaration. Approval for the study was granted by the Institutional Ethics Committee. A total of 40 adult patients classified as American Society of Anesthesiologists (ASA) physical status I–II, who were to undergo elective, open shoulder surgery, were recruited to participate in this trial. Written informed consent was obtained from each patient. Preoperatively, all the patients were informed about the postoperative visual analog scale (VAS) assessment. Subjective pain scores were assessed with a 10-cm VAS scale, where a score of 0 on the scale represented no pain and 10, the most severe pain imaginable.
Patients with ASA physical status III, IV, or V, any neurological or neuromuscular disease, infection at the injection site, bleeding disorders, or a history of hypersensitivity to local or other anesthetics were excluded from the study. Patients with acute or chronic infection, psychiatric disorder, pregnancy, bronchial asthma, allergy to nonsteroid anti-inflammatory drugs, gastric ulcer, colitis, hematopoesis massive cuff tears, previous surgery in the same shoulder, any glenohumeral pathology were also excluded as were any uncooperative patients.
The patients were randomly separated into two groups according to a computer-generated list of random numbers that were placed in opaque, sealed envelopes. CISB was performed to group CISB; continuous local anesthetic infiltration was performed to group CSIA. A loading dose of 40 mL 0.25% bupivacaine was administered and patient-controlled analgesia was applied by catheter with 0.1% bupivacaine 5 mL/h throughout 24 h basal infusion, 2 mL bolus dose, and 20 min knocked time in both groups postoperatively.
Anesthesia technique
All these procedures were performed by a single anesthesiologist. During the operation, electrocardiography, noninvasive blood pressure, peripheral arterial oxygen saturation, and end-tidal carbon dioxide were monitored using Dash 5000 (GE Healthcare, Milwaukee, WI, USA). All the patients were administered general anesthesia with propofol 2–3 mg/kg and remifentanil 1 µg/kg, and rocuronium 0.6 mg/kg i.v. for induction. Anesthesia was maintained with 40% oxygen in air and sevoflurane (2–3%) and continuous infusion of remifentanil (0.1–0.2 µg/kg/min).
After the skin was disinfected with povidone-iodine, the nerve was located using a 5.0–13.0 MHz linear probe (LOGIQ e; GE Healthcare, Princeton, NJ, USA). The transducer was positioned in the transverse plane to identify the carotid artery at the level of cricoid cartilage, the transducer was moved slightly laterally across the neck, and the brachial plexus could be identified between the anterior and middle scalene muscles. An 18G needle (Techniplex, 50 mm, 30°; Vygon, Ecouen, France) was inserted using an in-plane approach and advanced until it was located between the C5 and C6 nerve trunks. After careful aspiration to avoid intravascular needle placement, 1–2 mL of saline was injected. The correct position of the catheter in the plexus was observed. A loading dose of 40 mL 0.25% bupivacaine was administered and a 20-gauge perineural catheter was then inserted through the needle and advanced to a depth of 1 cm beyond the needle tip between the C5 and C6 nerve trunks.
Surgical technique
All operations were performed by a single orthopedic surgeon using a mini-open technique with an anterolateral approach. Diagnostic shoulder arthroscopy was performed to exclude any glenohumeral pathology without infusion of saline solution to the shoulder joint. After exclusion of glenohumeral pathology, a 3–4 cm skin incision was made from the anterolateral edge of the acromion distally. Soft tissue was dissected between the anterior and middle parts of the deltoid and a stay suture was placed in the distal end to prevent any further split in the deltoid and injury risk to the axillary nerve. Acromioplasty was performed with removal of hypertrophic acromion and the adequacy of the acromioplasty was checked by direct digital palpation. After the acromioplasty, a deltoid retractor was placed under the acromion for direct visualization of the rotator cuff and humeral head. In case of any tear in the rotator cuff, a footprint was prepared on the greater tuberosity using a ring curette. The torn tendon was repaired using the single- or double-row technique with suture anchors. During closure, a bone tunnel through the acromion was prepared to secure the deltoid insertion and possible avulsion of the deltoid from the acromion was prevented. A loading dose of 40 mL of 0.25% bupivacaine was administered to the subacromial and surgical area in the CSIA group and a three-hole 20-gauge catheter was placed in the subacromial area.
Postoperative period and follow-up
The total local anesthetic consumption over 24 h was recorded. Local anesthetic-related postoperative complications and side effects (nausea, vomiting, urticaria, pruritus, erythema, tachycardia, sneezing, etc.) were recorded. Pain during rest was assessed preoperatively and at 0, 1, 2, 8, 16, and 24 h postoperatively with a VAS numbered from 0 cm to 10 cm. About 1 mg/kg of tramadol and 15 mg/kg of paracetamol IV infusion was administered to patients with a requirement for additional analgesia (VAS ≥ 4).
In patients with no rotator cuff tear, a shoulder sling was applied after surgery and pendulum exercises were initiated on postoperative day 1. Passive ROM and active-assisted ROM exercises were started on the third postoperative day. For patients with rotator cuff tear repair, an abduction brace was applied and pendulum exercises were started 3 weeks postoperatively. Shoulder scores were evaluated preoperatively and in the first and third week postoperatively in patients without any cuff tear and preoperatively and in the third week postoperatively in patients with a cuff tear.
Statistical analysis
Statistical analysis was performed using SPSS 19.0 statistical software. In the assessment of the study data, Pearson χ2, Fisher χ2, or Yates χ2 tests were used in the comparison of qualitative data in addition to descriptive statistical methods (frequency, percentage, mean, standard deviation). The Kolmogorov–Smirnov test was used to examine the conformity of data to normal distribution. The independent samples t-test (t-test for independent groups) was used to assess quantitative data with normal distribution. Repeated-measures analysis of variance was used in the comparison of repeated measurements. Tukey versus least significant difference tests were applied to determine in which groups differences lay when the groups demonstrated differences in multiple comparisons. A value of p < 0.05 was accepted as statistically significant.
Sample size was estimated using the VAS score as a primary effect variable. A difference was assumed in means of 1.5 and standard deviation of 1.4 for each group. The group sample sizes of 19 demonstrated a power of 0.90 to detect a difference of 2 between the two groups with the estimated group standard deviations of 1.4 for each group and with a significance level (α) of 0.05 using a two-sided, two-sample test. Thus, the study included 20 patients in each group in case of possible loss during follow-up.
Results
Interscalene block failed in one patient. The catheter was accidentally removed in one patient in the CISB group and in three patients in the CSIA group. The pain of those patients was controlled with tramadol and paracetamol infusion. These patients were excluded from the statistical analysis. Besides these, there were 20 patients in each group. The demographic data and preoperative variables including duration of pain, presence of tear, and preoperative pain VAS scores were statistically similar (Table 1).
Patient characteristics and intraoperative data in the two groups.a

ASA: American Society of Anesthesiologists; BMI: body mass index; CISB: continuous interscalene block; CSIA: continuous local anesthetic infiltration; VAS: visual analog scale; SD: standard deviation.
aValues are the number of patients (n) or means ± SD.
b p < 0.05 between groups.
No minor side effects (nausea, vomiting, etc.) were determined in the patients of group CISB, but there were complications in 30% of the patients in group CSIA (p < 0.05). A statistically significant difference was found between the additional analgesic requirements of the CISB and CSIA groups (p < 0.05), with a lesser requirement in the CISB group. The VAS scores were significantly lower in group CISB at all times (p < 0.05; Table 2). A statistically significant difference was determined between the groups in respect of the total consumption of local anesthetic (p < 0.05) with a lower amount consumed in the CISB group (Table 3). There were no significant differences in the preoperative and postoperative third-week ROM scores of the two groups (p > 0.05). A significant difference was determined in the postoperative first week (p < 0.05) with a higher ROM score in group CISB patients (Table 4).
Comparison of VAS between groups.a
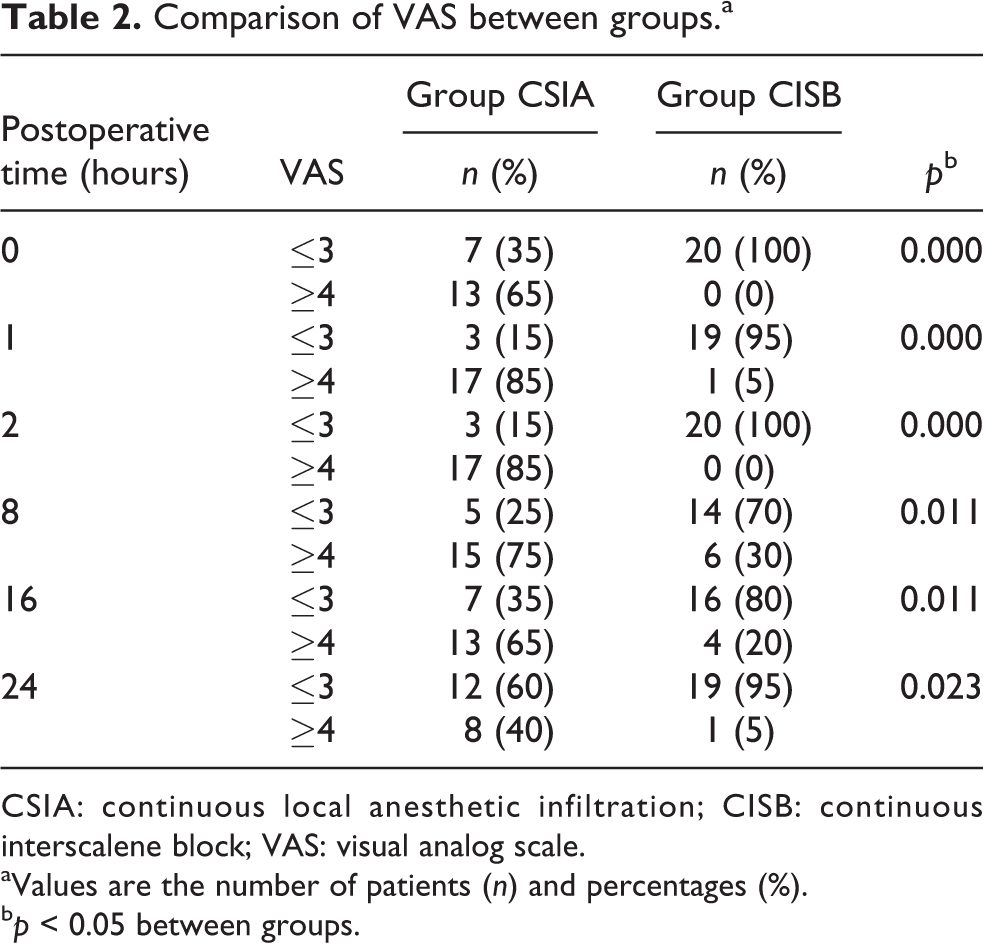
CSIA: continuous local anesthetic infiltration; CISB: continuous interscalene block; VAS: visual analog scale.
aValues are the number of patients (n) and percentages (%).
b p < 0.05 between groups.
Comparison of CLA between groups.a

CLA: consumption of local anesthetic; CSIA: continuous local anesthetic infiltration; CISB: continuous interscalene block; SD: standard deviation.
aValues are the number of patients (n) or means ± SD.
b p < 0.05 between groups.
Comparison of ROM scores between groups.a

CSIA: continuous local anesthetic infiltration; CISB: continuous interscalene block; ROM: range of motion; SD: standard deviation.
aValues are the number of patients (n) or means ± SD.
b p < 0.05 between groups.
cPreoperative period.
dPostoperative first week.
ePostoperative third week.
Discussion
This study compared the efficacy of equal bolus doses, basal infusion rates, and patient-controlled additional bolus doses of CISB and CSIA for pain relief after open shoulder surgery. The results of the study showed that after open shoulder surgery, compared with CSIA, CISB provided effective pain control with less additional analgesic and used volume of bupivacaine, a better clinical outcome and ROM in the early period of the first week without side effects. Interscalene block is widely used after shoulder surgery. Baskan et al. reported that a single injection of interscalene brachial plexus blockade had shown good results in postoperative analgesia with 40 mL 0.25% bupivacaine in the early postoperative period (initial 12 h). 4 Following major shoulder surgery, patients might experience severe pain extending beyond the duration of a single injection block so the placement of an interscalene catheter allows for long-term effective analgesia after CISB with or without concomitant patient-controlled interscalene analgesia (PCIA). 5 –7
Different analgesia regimens have been used for PCIA. Kabangoo et al. used CISB maintained by a continuous infusion at 5 mL/h and PCIA boluses of 2.5 mL/30 min of 0.1% bupivacaine. 8 This PCIA protocol was similar to the protocol of the current study and both were effective and safe protocols. Previous studies have shown that subacromial infiltration analgesia provided acceptable pain relief after open acromioplasty surgery. 9,10 It has been demonstrated that the subacromial area tendered a suitable compartment for the administration of local anesthetics for the spread of these analgesics to the injured area and single or continuous local anesthetic infiltrations were also useful methods for postoperative pain relief after shoulder surgery. 11 –13 Continuous infusion after 20–50 mL local anesthetic injection to the joint space or subacromial area has been reported to be effective in postoperative analgesia.
Laurila et al. reported that CISB was found to be more effective than the subacromial continuous infusion of local anesthetic for pain control after arthroscopic shoulder surgery. 12 Nisar et al. reported that there was no significant difference between interscalene block and subacromial bursa block groups with regard to pain scores in the first 12 h postoperatively. 14 Another study reported that CISB provided better postoperative analgesia than a continuous subacromial infusion. 15 In the current study, it was shown that patients in both the CISB and CSIA groups achieved a significant decrease in postoperative pain scores. The CISB group demonstrated a lower total volume requirement for bupivacaine, more effective pain control, reduced supplementary analgesic requirement, fewer minor side effects, and good patient satisfaction compared with the CSIA group after surgery. The low-dose regimen of this protocol substantially reduced the risk of systemic toxicity. In addition, higher concentrations of bupivacaine also produced motor block and would limit postoperative mobilization and rehabilitation. No acute complications or severe side effects were observed in either the CSIA or CISB group during the study period. Minor adverse effects were less frequent in the CISB group than in the CSIA group, which could have been due to the use of a higher volume of bupivacaine.
CISB is an effective method of postoperative analgesia after major surgery of the shoulder. However, the success of CISB requires an experienced anesthesiologist and the application of nerve stimulator or ultrasonography. In the current study, the block was unsuccessful in one patient. The subacromial bursa is a suitable compartment for the administration of local anesthetics. The insertion of a subacromial catheter is simple as there are no significant adjacent structures as there are in the interscalene plane. If a suitable dose and concentration of bupivacaine is used, CSIA should be an efficient method for postoperative analgesia after shoulder surgery. However, a larger volume of local anesthesia has the potential risk of toxicity due to accumulation of the drug and cases of glenohumeral chondrolysis have been described in patients at 48–72 h following intra-articular infusions of local anesthetic. 1 Although CSIA is not as effective as an interscalene block, CSIA may be a simple and safe alternative to CISB in infusions of local anesthetics in a 24-h period as it provides good pain relief, is practical to apply, and has a lower incidence of serious adverse effects and motor-sensory deficits. According to the result of the present study, patients in Group CISB had a better clinical outcome and ROM in the early period of the first week after surgery. Although the patients had similar clinical outcomes in the third week, the differences in the first week were valuable in respect of patient comfort and adaptation to rehabilitation in the early period.
There were some limitations to this study. First, this study did not evaluate the more invasive conventional open technique. Second, patients with glenohumeral pathology were excluded from the present study, so the effect of concomitant pain of glenohumeral pathology was not reported. Finally, massive rotator cuff tears were excluded in the present study, so the comparative effect of CISB and CSIA could not be evaluated in patients with massive tears in respect of pain and function. Despite these limitations, the present study has shown that continuous interscalene infusion of bupivacaine is an effective and safe method of postoperative analgesia after open shoulder surgery. The clinical relevance of the study is that CISB provides better analgesia and uses a lower volume and dosage of local anesthetic compared with CSIA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.