
Abstract
Background:
The frequency of the complications following total hip arthroplasty (THA) using the two-incision technique is well documented. However, few reports have analyzed the preoperative patient–related factors associated with the complications. The purpose of this study was to estimate the incidence of early complications following primary two-incision THA and to define the risk factors associated with perioperative complications.
Materials and Methods:
The subjects of this retrospective study were 1218 consecutive patients who underwent primary two-incision THA. The incidence of hip dislocation, stem subsidence, intraoperative femoral fracture, and nontraumatic postoperative femoral fracture was evaluated. The association between complications and preoperative patient–related factors, including gender, obesity, Crowe classification, age, body mass index (BMI), and morphological parameters of the proximal femoral medullary cavity, were investigated.
Results:
The incidences of complications were dislocation (1.1%), stem subsidence (0.9%), intraoperative femoral fracture (1.2%), and postoperative femoral fracture (0.7%). Obesity (BMI > 30) influenced the occurrences of stem subsidence and postoperative femoral fractures (p = 0.0001, p = 0.019). Crowe classification significantly correlated with intraoperative femoral fractures (Grade II: odds ratio (OR) 4.63, 95% confidence interval (CI), 1.32–15.6; Grade III and IV: OR 8.96, 95% CI, 2.2–34.94). Additionally, the outer diameter of the femur 10 cm below the lesser trochanter tended to be small in patients who developed a femoral fracture.
Conclusions:
The early complication rate was comparable to other methods used in uncemented THA. It is necessary for patients with risk factors revealed in this study to pay careful attention or consider other surgical approaches to avoid complications. Further studies considering femur morphology are required.
Introduction
In cases where conservative treatment was unsuccessful, total hip arthroplasty (THA) provides pain relief and improves the quality of life in patients who suffer from hip arthritis. However, there is a possibility of extension of hospital stay and poor final outcome if a complication occurs.
Minimally invasive surgery (MIS) has been used for THA to facilitate rapid recovery, shorten hospitalization duration, and obtain satisfactory long-term radiological and clinical outcomes with small incisions and minimal tissue damage. The two-incision technique has been developed as an MIS; however, there have been a number of reports regarding early complications such as femur fractures.
The frequency of complications associated with the two-incision technique has been well documented. 1 –3 However, there are few reports analyzing the preoperative patient–related factors associated with the complications.
The purpose of the following retrospective study was to estimate the incidence of early complications following primary THA using the two-incision technique and to define the risk factors associated with perioperative complications.
Materials and methods
The current study was a retrospective, single-center, observational study. Demographic data were entered into a retrospective database and later abstracted for analysis. The study was approved by the hospital research ethics committee.
The subjects included 1218 consecutive patients who had undergone primary THA using the two-incision technique as described by Mears 4 and Berger, 5 between April 2004 and April 2014. All primary THA in this period were performed using the two-incision technique except for cases that need to have the osteosynthesis implant removed. There were 1105 women and 113 men, with a mean age of 66.0 years (range 39–91). The mean body mass index (BMI) of the subjects was 23.6 ± 3.7 kg/m2. Based on the Crowe classification, there were 927 type I hips, 180 type II hips, 73 type III hips, and 10 type IV hips. The classification of 28 hips was unknown because preoperative radiographs that were conducted by another medical facility had been returned.
All procedures were performed without cement and with the use of fluoroscopic guidance. A monoblock, distally tapered design stem (VerSys Fiber Metal Taper Hip Prosthesis; Zimmer, Inc, Warsaw, IN) and a proximally modular, tapered wedge-design stem (M/L Taper with KinectivTM Technology; Zimmer, Inc), was used. The patients were mobilized immediately after surgery and encouraged to bear weight.
The minimum clinical follow-up time was 12 months (mean 64.9 months; range 12–133 months).
The incidence of hip dislocation, stem subsidence, intraoperative femoral fracture, and nontraumatic postoperative femoral fracture following THA was evaluated as the early complications. The incidences were compared among the groups, which were categorized based on each of the preoperative patient–related factors. The preoperative patient–related factors included gender, obesity, and Crowe classification. In addition, patients were divided into complication and noncomplication groups. Clinical data, including age and BMI, were analyzed between these groups.
Stem subsidence was defined as a decrease of >5 mm in vertical distance from the tip of the greater trochanter to the shoulder of the prosthesis measured on anterior–posterior (AP) radiographs.
The canal flare index (CFI), cortical thickness index (CTI), outer diameter of the femur 10 cm below the level of the lesser trochanter, and inner diameter of the medullary cavity at the canal isthmus in preoperative anteroposterior radiographs were also evaluated. The morphological parameters of the proximal femoral medullary cavity were compared between each complication group. CFI was defined as the ratio of the intracortical width of the femur at a point 20 mm proximal to the lesser trochanter and at the canal isthmus by Noble et al. 6 CTI was calculated using the following equation: CTI = (α − β)/α, where α is the outer diameter of the femur and β is the inner diameter of the medullary cavity 10 cm below the level of the lesser trochanter. 7
Excel (version 2007) and JMP 11.0 (SAS Institute Inc, Cary, NC) were used for statistical analysis. We determined differences in each complication incidence among the groups divided in terms of each of the preoperative patient–related factors using chi-square test. The complications with multiple preoperative factors were examined by adding a multivariate analysis using the logistic regression analysis with each risk factor as a covariate. After the data distribution was tested with a Shapiro–Wilk test for normality, the Mann–Whitney U test was used for comparison between the complication and noncomplication groups. For radiological assessment, the differences in morphological parameters among each complication group were determined. The comparison was conducted using a Tukey’s range test when the normality condition was satisfied and using a Steel–Dwass test when the normality was not satisfied. To test for normality, a Shapiro–Wilk test was used. All tests were two tailed, and statistical significance was assumed when a p value of < 0.05 was obtained.
Results
The incidence of complications was dislocation (1.1%), stem subsidence (0.9%), intraoperative femoral fracture (1.2%), and nontraumatic postoperative femoral fracture (0.7%).
No significant difference in the incidence of hip dislocation was evident among the groups divided in terms of gender, obesity, and Crowe classification. There was no significant difference in the mean age and mean BMI between the dislocation and nondislocation groups. The incidences of hip dislocation in each group are shown in Table 1. The incidence of stem subsidence was significantly higher in the obesity group than in the nonobesity group. The incidences of stem subsidence in each group are shown in Table 2. There was a significant difference in the mean BMI ranks between the stem subsidence and nonstem subsidence groups (p < 0.01, Mann–Whitney U test).
The incidences of hip dislocation.

BMI: body mass index.
The incidences of stem subsidence.

BMI: body mass index.
a p < 0.01.
Analysis using the chi-square test suggested that obesity (BMI > 30) and a high grade of the Crowe classification were related to intraoperative femoral fracture. The incidences of intraoperative femoral fracture in each group are shown in Table 3. Analysis using logistic regression suggested that the Crowe classification was significantly related to intraoperative femoral fracture. The grade II group as well as the grades III and IV groups had a significantly higher frequency of intraoperative femoral fracture (Grade II: odds ratio [OR] = 4.63, 95% confidence interval [CI] = 1.32, 15.6; p = 0.017; Grades III and IV: OR = 8.96, 95% CI = 2.2, 34.94; p = 0.0036) than the grade I group (Table 4).
The incidences of intraoperative femoral fracture.

BMI: body mass index.
a p < 0.05.
b p < 0.01.
Multivariate analysis for intraoperative femoral fracture.

CI: confidence interval.
a p < 0.05.
b p < 0.01.
The incidence of nontraumatic postoperative femoral fracture was significantly higher in the obesity group with a BMI > 30. The incidences of nontraumatic postoperative femoral fracture in each group are shown in Table 5.
The incidences of nontraumatic postoperative femoral fracture.
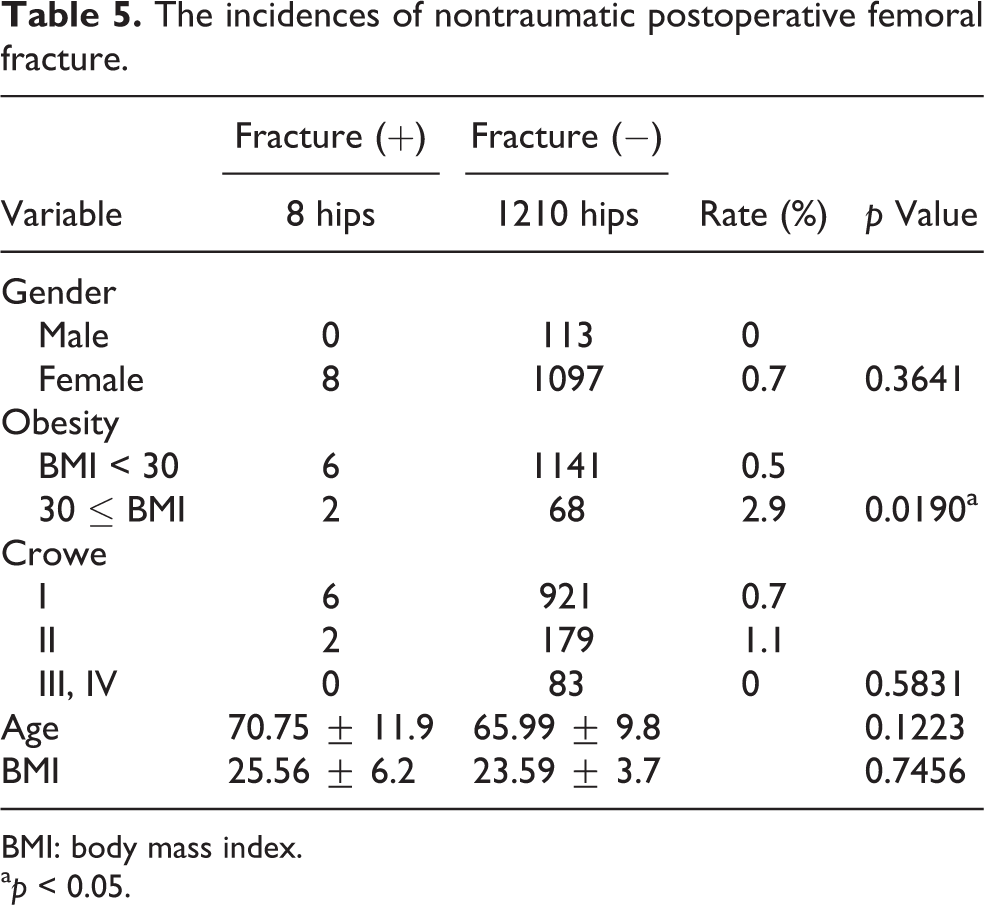
BMI: body mass index.
a p < 0.05.
Evaluation of the preoperative radiograph showed that no significant difference in CTI was evident among each complication group. CFI and the inner diameter of the medullary cavity at the canal isthmus in the stem subsidence group were statistically different than those seen in the group with intraoperative femoral fractures (p < 0.05, p < 0.05, respectively).
There was a significant difference in the outer diameter of the femur 10 cm below the level of the lesser trochanter between each complication group (Figure 1). The outer diameter of the femur tended to be small in the group with an intraoperative or postoperative femoral fracture.

The mean outer diameters of the femur 10 cm below the level of the lesser trochanter between each complication group are shown (†p < 0.01, *p < 0.05).
Discussion
The two-incision technique has been developed as an MIS. This technique uses an anterior incision for acetabular cup replacement and a posterior incision for femoral stem insertion to minimize tissue damage, enhance recovery, and shorten hospitalization duration. 3,8 However, some clinicians are skeptical of the technique because of restricted visualization during surgery and the need for special equipment, which results in a longer operation time and higher complication rates than the conventional surgical techniques. 1,9 In addition, the two-incision technique has a longer learning curve than the other methods. 2,3
The present study has some limitations that should be considered. First, there is a possibility that intraoperative fractures were overlooked at the time of surgery and were later found as postoperative femoral fractures. It is indeed difficult to distinguish between an intraoperative and postoperative fracture. Invisible intraoperative fractures may have been counted as postoperative fractures because of restricted visualization during surgery and confirmation with fluoroscopy. Second, we dealt with various types of periprosthetic femoral fractures throughout the study. The periprosthetic femoral fractures ranged widely with respect to the location, pattern, and stability of the fracture for various reasons such as improper stem insertion, mismatch of stem size, and shape. These observations should have been considered but were not examined. Third, there was no comparison group treated in another approach. All primary THA in this period were performed using the two-incision technique except for cases that need to have the osteosynthesis implant removed. However, it might contribute to avoid any bias in patient selection.
In the current study, dislocations were found in 13 cases (1.1%); however, it was not possible to clarify the preoperative factor associated with the dislocation. In most of the dislocation cases, there was no implant malposition; however, the patients may have made movements or may have been in positions that led to a dislocation in the early postoperative period. Postoperative strict restrictions regarding the range of motion and further patient education may also help to reduce dislocations.
A high incidence of intraoperative periprosthetic fracture is one of the reasons for which the two-incision technique is not favored. However, we have made improvements on devices such as rasps with cutting teeth on the lateral face only and shortened side-cutting reamers to remove an additional bone from the medial portion of greater trochanter and to sufficiently help avoid varus stem positioning. Furthermore, we inserted prosthesis with great care to maintain proper anteversion and to avoid varus positioning. Therefore, the incidence of perioperative femoral fractures in the present study decreased to 1.9%, which was a combined incidence of intraoperative and early postoperative fractures. This is comparable to the incidence of perioperative femoral fractures in uncemented total hip replacements in general. 10 Therefore, fracture risks inherent to the two-incision technique may have been nearly overcome.
In general, intraoperative femoral fractures while using a cementless stem have a higher incidence than that of the cement system used; it has been reported to be 1.5 –27.8%. 10 –13 It is often a consequence of the effort to obtain a sufficient press fit to gain initial stem stability. Female gender and increased age have been suggested as independent risk factors of intraoperative fracture 14 ; however, we have not observed the influence of gender and age on intraoperative fracture in the current study. On the other hand, other factors such as obesity and Crowe classification have been revealed. The stem design also has significant influence on intraoperative fractures obviously. We used two different cementless stems. But it is difficult to evaluate the influence of stem design with respect to intraoperative fractures because the indications for stem were not the same in the current study. VerSys Fiber Metal Taper stem was often used for narrower femurs, which do not fit the smallest size of M/L Taper Kinectiv stem according to preoperative measurement of the femoral bone shape.
The incidence of complications in our first 200 cases was dislocation (0.5%), stem subsidence (0.5%), intraoperative femoral fracture (4%), and nontraumatic postoperative femoral fracture (0%). It was considered that only intraoperative femoral fracture was affected by learning curves.
Altered bone morphology or deformity, as seen in Paget disease, can also increase the risk of fracture. 15 To evaluate proximal femoral morphology in the current study, the CFI, CTI, outer diameter of the femur 10 cm below the level of the lesser trochanter, and inner diameter of the medullary cavity at the canal isthmus were investigated. The outer diameter of the femur 10 cm below the level of the lesser trochanter tended to be small in the femoral fracture groups. However, further studies regarding femur morphology are required because the current study did not make comparisons with the nonfracture group.
The present investigation did not show a clear trend in the other X-ray parameters using an AP radiograph. The reason for this may be due to an inappropriate evaluation because many hip osteoarthritis patients often have a hip contracture in the external rotation position. In the femoral shaft cross-section 10 cm below the level of the lesser trochanter, the medullary cavity is an almost oval shape in the longitudinal direction. On the other hand, the periphery of the femoral shaft is relatively close to a circle. As a result it has been speculated that the outer diameter of the femur is difficult to be affected by hip rotation. An additional investigation using a lateral radiograph or computed tomography is necessary.
Conclusion
In conclusion, the complication rate of THA using the two-incision technique was acceptable. Obesity influenced the occurrences of stem subsidence and nontraumatic postoperative femoral fractures, and the Crowe classification was significantly correlated with intraoperative femoral fractures. In addition, the outer diameter of the femur 10 cm below the level of the lesser trochanter tended to be small in patients who developed a femoral fracture. Therefore, it is necessary for patients who have risk factors revealed in the current study to consider other surgical approaches to avoid complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.