
Abstract
Three-dimensional (3-D) printing or additive manufacturing, an advanced technology that 3-D physical models are created, has been wildly applied in medical industries, including cardiothoracic surgery, cranio-maxillo-facial surgery and orthopaedic surgery. The physical models made by 3-D printing technology give surgeons a realistic impression of complex structures, allowing surgical planning and simulation before operations. In orthopaedic surgery, this technique is mainly applied in surgical planning especially revision and reconstructive surgeries, making patient-specific instruments or implants, and bone tissue engineering. This article reviews this technology and its application in orthopaedic surgery.
Keywords
Introduction
Three-dimensional (3-D) printing technology, also named additive manufacturing, has been being applied in medical industry for more than 10 years. It is mainly applied in surgical specialties, such as cranio-maxillo-facial surgery, 1 cardiothoracic surgery 2 and orthopaedic surgery. Pelvic surgeries, joint revision surgeries and trauma surgeries with significant bone loss and bone deformities are still very challenging to most of the orthopaedic surgeons. The advanced medical imaging, including computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography, has been making the diagnosis easier and more reliable. 3-D reconstruction images from CT and MRI even provide a more superior visualization, aiming at more accurate diagnosis and better surgical management. However, 3-D pictures displayed on computer screen cannot provide a physical model perception, especially in complicated cases.
The 3-D printing technology applied in medicine was first described by Mankovich et al. in 1990. 3 The concept of this technology is to build physical model by adopting the layer-by-layer approach in which the powder-like or gel-like metal or plastic materials will deposit at particular coordination based on the data set of imaging obtained from CT or MRI. Therefore, even the physical model with a complex structure can be printed out. From the 1990s, this technique has been developing rapidly, and by now, it has been widely used in different areas, such as industrial design and manufacturing as well as medicine. 3-D printing technique has been successfully applied in orthopaedic surgery in terms of the fabrication of tissue engineering scaffold, surgical planning for complicated cases and patient-specific instruments (PSIs) and implants. It can turn a 3-D digital model into a realistic physical object, thereby giving out a direct and better visualization. Compared with conventional imaging modalities, the advantages of 3-D printing technology are obvious. The 3-D model can improve the quality of surgical planning, the accuracy of clinical diagnosis, the production of surgical implants and personalized prostheses for patients and template for surgical resection.
This article provides an overview of the recent 3-D printing technology in the field of orthopaedic applications and summarizes some of the issues and the development direction of its current existence.
Image acquisition and processing for 3-D printing
The first and most important step is the image acquisition. The quality of physical models depends on the quality of data sets and the processing afterwards, and therefore, the quality of source images is very important in creating a good 3-D model. Currently, image data used for 3-D printing are acquired from CT, MRI or other imaging modalities. Bony tissues have a relatively higher contrast and exposure than that of soft tissue showed in CT, and therefore, CT images are usually the sources of image for 3-D printing in orthopaedic surgery.
High-performance workstations and software are essential for the processing of image data. The common tools for 3-D afterward processing include cutting tool and visualized tool. The cutting tool is for separation of simple target region, while visualized tool is for surface/volume rendering, maximal/minimal projection and multiplane modification. Now, these techniques are widely used in the CT data processing, especially in surgical fields, such as diagnosis, preoperative evaluation and operative planning in vascular surgery, orthopaedic surgery and paediatric surgery.
After grid processing of those separated target regions, the outline of the target will be composed of many tiny pyramids. It is obvious the smaller of each pyramid, the more number they will be, and smoother the surface of the model, larger data volume for the model will be. Then, these data will be optimized by computer-aided design software and be transmitted to a 3-D printer for printing.
3-D printing technologies in orthopaedic surgery
There are mainly two 3-D printing techniques in orthopaedic surgery, namely subtractive and additive techniques. The subtractive technique for medical application is milling, in which the physical model will be milled from a block of polyurethane or other foam. The advantage of this technique is low material cost. However, the geometric accuracy is poor and cannot be sterilized for intraoperative use. Additive techniques are another method commonly used in orthopaedic surgery, in which the models are produced through layer by layer with powder-like or liquid-like metal or plastic material. Compared with subtractive technique, additive techniques can produce complex structures and cavities.
Additive technologies commonly used in orthopaedics are stereolithography, selective laser sintering (SLS) and fused deposition modelling (FDM).
Stereolithography uses an optical light energy source to scan over a vat of light-curable resin, solidifying specific areas on the surface of the liquid. The floor of the fluid container gradually descends, which increases the depth of the material as the model grows and successive layers of resin are cured on top of each other. SLS uses high-power laser to fuse small powders made of plastic, metal, ceramic or glass into a physical model based on the 3-D images created by computer-aided design. It can provide a more accurate geometry. However, the cost of SLS is high and cannot be used in operating theatre. FDM works by extraction and solidification of materials in layers. Layers are made by the deposition of a heated polymer with the use of a computer-controlled extrusion nozzle. Different materials and colours can be chosen using this technique. The geometric accuracy is high and can be used in operating theatre. However, the production time is long and the surface quality is not good enough.
Clinical application in orthopaedic surgery
Surgical planning
3-D printing techniques have been used in surgical planning for complicated cases, aiming at reducing the duration of surgery and the risk of complications. Based on the patients’ preoperative images like CT or MRI (Figure 1(a) to (c)), a 3-D physical object model (Figure 2) with accurate anatomy around the surgical region can be directly printed out, and it is more intuitive and applicable than that of 3-D images. Surgeons can make a more accurate diagnosis and more detailed surgical planning, and is more readily aware of the risks of surgery (Figure 3). Furthermore, surgeons can do surgical simulation and operate directly on the physical models. As a result, the surgical time may be shortened and may improve the surgical outcomes. 4,5

(a) CT pelvis transverse film showed fracture left acetabulum. (b) CT pelvis coronal film showed fracture left acetabulum. (c) CT 3-D reconstruction of the fracture left acetabulum. CT: computed tomography. 3-D: three-dimensional.
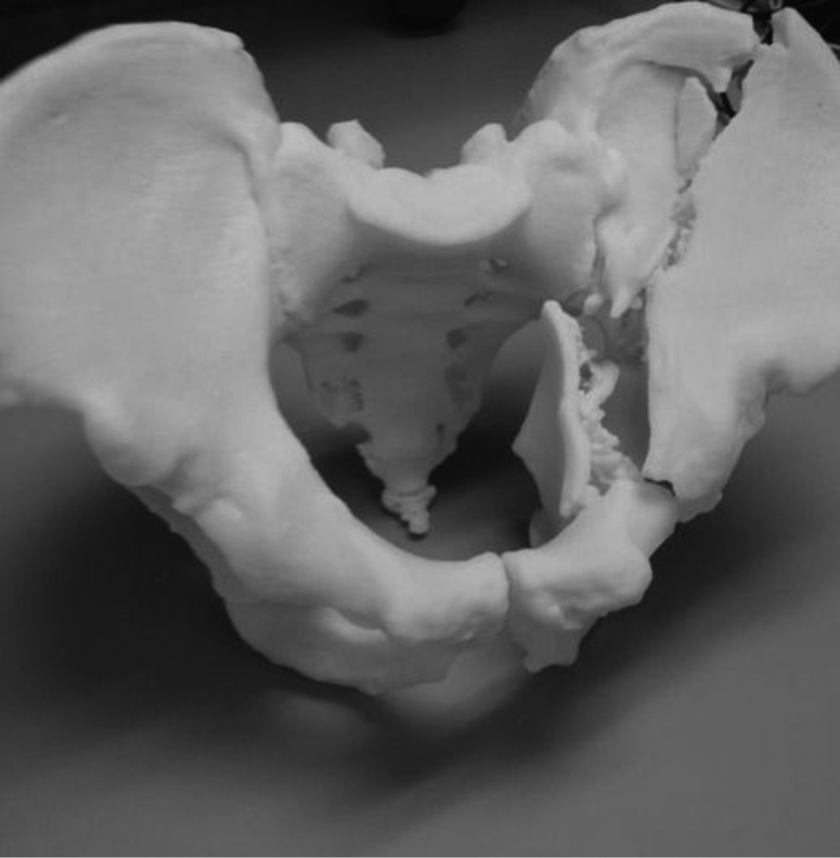
A 3-D life size physical model of a pelvis showing fracture left acetabulum after 3-D printing. 3-D: three-dimensional.

A detailed surgical plan achieved with the presence of a true 3-D pelvis model. 3-D: three-dimensional.
By now, 3-D printing technique has been successfully being applied in surgical planning. As early as 1997, Kacl et al. had reported that rapid prototyping (RP) might be useful in teaching and surgical planning, although his article did not reveal any difference between stereolithography and workstation-based 3-D reformations in the management of intra-articular calcaneal fractures. 6 Yang et al. did a retrospective study on the effectiveness of RP technology in corrective surgery for idiopathic scoliosis patients and concluded that this technology might reduce operation time and perioperative blood loss, but complication rate was the same. 7 Guarino et al. reported 10 cases of paediatric scoliosis and 3 complicated pelvic fracture cases and concluded that 3-D printing could improve the accuracy of pedicle and pelvic screws placement, and thereby reduced the risk of iatrogenic neurovascular injury. 8 Brown et al. reported 117 complicated surgical cases managed with the help of 3-D printing. The research concluded that 3-D printing technology was effective in surgical planning and the technology could help in reducing the exposure of radiation during surgeries. 9 Hurson et al. reviewed 12 cases of fracture acetabulum being classified and planned with RP prior to surgery and showed that physical models greatly assisted surgeons understanding the complexity of fracture, especially for less experienced surgeons. 10 Bagaria et al. concluded that RP technology could help surgeons to understand more on the fracture configuration of complex fractures and to achieve near anatomical reduction. 11 Xu et al. did a pilot study on the effectiveness of RP in surgical planning of patients with developmental dysplasia of hip and found that the use of RP could facilitate the surgical procedures due to better planning and improved orientation. 12
Manufacture of PSIs and implants
Apart from preoperative surgical planning, another application of 3-D printing technology in orthopaedic surgery is manufacture of patient-specific surgical guides and implants. Its application is mainly in total joint arthroplasty, tumour and deformity correction. RP technology can help surgeons to design surgical cutting guides (Figure 4) that can perfectly match patients’ anatomy, and accurate resection can be achieved. For total knee arthroplasty, several authors have reported that there are no significant differences in the overall alignment between patient-matched instrument and conventional instrument, and further studies have been suggested regarding functional outcomes and longevity of the prostheses. 13 –21

PSIs for total knee arthroplasty. PSI: patient-specific instrument.
Rathod et al. found that PSI could reduce blood loss in bilateral total knee replacement because of avoidance of intra-medullary instrumentation. 22 Nunley et al. reported that PSI showed slight improvement in the time management of operating room. 19
On the other hand, RP technology shows promising results in tumour and deformity correction surgeries. Cartiaux et al. showed that PSI could improve pelvic bone tumour surgery by providing good cutting margin. 4 Bellanova et al. did a retrospective review on patients with tibial sarcoma managed by PSI-assisted resection and allograft reconstruction. 23 The work concluded that PR techniques might help to improve the accuracy of resection margin. Kunz et al. used the PSI to perform distal radius osteotomy and found that PSI could minimize the need for intraoperative fluoroscopy. 24 Otsuki et al. evaluated seven patients with acetabular dysplasia being managed by PSI-assisted curved periacetabular osteotomy. No major complications were noticed and the actual cutting line corresponded exactly to the planned cutting line. 25 For the individual printed implants and synthetic devices, this technology is mainly being used in some complicated cases, such as pelvic tumour 26 and spinal tumour. 27 Further research is required to determine its long-term clinical benefits, cost effectiveness and complications. 28
Bone tissue engineering
Bone tissue engineering is an interdisciplinary field that aims to combine the knowledge of cells, biomaterials and biochemical factors to create a surrogate structure to regenerate new bone. It provides a structural scaffold for cell attachment and proliferation as well as the subsequent bone formation in vivo. 29 The 3-D printing technology is currently for the production of structurally sophisticated bioscaffolds. 29,30 To achieve significant biological and mechanical properties, the 3-D bioscaffolds should be designed according to the need of clinical application. For instance, the bioscaffold for hard tissue regeneration must be mechanically strong, while a flexible bioscaffold is recommended for cartilage regeneration. Moreover, the structural parameters, such as porosity, the diameter of pore and interconnectivity, can be precisely controlled by computer program in order to maintain the adhesion, proliferation and differentiation of cells. The other attractiveness of 3-D bioscaffold is able to allow bony tissue in-growth, thereby facilitating superior fracture healing. 31 –33 Currently, hydroxyapatite and calcium phosphate are the main biomaterials for porous scaffold fabrication, as they are highly biocompatible and biodegradable. However, low mechanical strength is a major challenge and most of scaffolds are only used in non-loaded bearing regions. 34 Hence, the development of new 3-D printable bioinks is needed.
Current limitations
3-D printing is an innovative technique and has been being applied extensively in medicine. Its advantages are obvious that it can create a true physical model and allow surgeons to have a better understanding on the complexity of diseases prior to surgery. In addition, it can make surgical cutting guides according to patients’ geometry to increase the accuracy of resection. Scaffolds production for bone tissue engineering by this technology is another application used in orthopaedic surgery. However, it has its limitations.
First, the costing of 3-D printing technology is high. It includes hardware, software, manpower for maintenance and the cost of printing materials. In contrast to physical products for commercial purpose by 3-D printing, those 3-D products in medicine usually are patient specific. As a result, the cost of production is high and unlikely to decrease through increasing the production. The cost to process a spleen 3-D model is around €300. 35 A polymethyl methacrylate (PMMA) cement implant for cranioplasty costs US$300–400. 36
Another problem of 3-D printing is the timescale for production of physical models. It is variable and dependent on the size and complexity of the physical models. Imaging and data processing of the objects need around hours. Depending on the type of printing machines, the process of actual printing is usually within 24 h and rarely more than 24 h. This may limit its clinical application, especially when there are emergency procedures.
The 3-D printing materials that are commonly used in orthopaedic surgery are metals, ceramics, polymer materials and bone cement. Since this technology is based on raw material being placed layer by layer and then bonded together, the mechanical strength of the printed objects is inferior to the real ones 37 and not suitable for long-term use. Farzadi et al. suggested increasing the layer thickness might increase the mechanical properties of the printed objects. 38
Safety and regulation of 3-D printing technology is another consideration as this technology continues to integrate and gain popularity into medical practice. Fewer studies have evaluated the potential risks of the technology and the physical products. The US Food and Drug Administration has drafted and published some guidelines on the safety and sustainability of 3-D printing. 39
Future trend
3-D printing has been playing an important role in orthopaedic surgery, through its application in surgical planning, manufacture of customized instruments and prostheses and making scaffolds for tissue engineering. Recent advance in 3-D printing technology is bioprinting, layer-by-layer positioning of biological, biochemical materials and even living cells to fabricate complex organs. There are several challenges that being encountered at this stage. First, there is a difficulty to reproduce the extracellular matrix and different cell types to rebuild the biological function. Another problem is the vasculature of the bioprinted products. For orthopaedic surgery, another challenges that should be settled are the stability and mechanical strength of the bioprinted products.
In situ bioprinting, in which implants or complex organs are printed during operations, is another anticipated future trend. 40 Through the use of bioprinting, scaffolds that made of cells, biomaterials can be deposited to repair the lesions of various types and sizes immediately during operations. Currently, in situ printing has been applied to repair skin defects. 41 With the advancement of in situ bioprinting technique, bone and soft tissue defects can be repaired during operations in the very near future.
Conclusions
3-D printing is an innovative technology that has been being used in various fields, in particular, orthopaedic surgery. Although this technology is not commonly used by now, however, with the advancement and popularity of this technology, its use in preoperative surgical planning, implant design and tissue engineering and even as a training tool is likely to become widespread in the near future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.