
Abstract
Radial nerve palsy may result from various pathologies, including trauma, nerve sheath tumor, neuritis, or compression neuropathy. In most instances, the underlying cause is apparent preoperatively and an appropriate operative plan can be formulated. Here, we present a case where the preoperative diagnosis was inaccurate and intraoperative decision-making required deviation from the planned procedure. The patient's history, physical examination, and imaging were consistent with a radial nerve tumor; however, surgical exploration revealed a compression neuropathy with pseudoneuroma formation. This case reinforces the importance of including compression neuropathy and pseudoneuroma in the differential diagnosis of a mass-associated motor nerve palsy, even at sites where nerve compression is relatively uncommon. Surgeons should be prepared to abort a planned biopsy and instead perform complete nerve decompression at the time of exploration when intraoperative findings are inconsistent with a neoplasm.
Case Report
A 66-year-old woman noticed a new lump over the posterolateral aspect of her left arm and, 2 days later, developed a painless complete radial nerve palsy. Examination demonstrated wrist and finger drop with no active extension against gravity and numbness in the superficial radial nerve distribution. A firm, nontender, mid-humeral mass was palpable in the region of the spiral groove. Median and ulnar nerve function was normal.
Ultrasound, radiographs, and contrast-enhanced magnetic resonance imaging (MRI) were obtained. Magnetic resonance imaging demonstrated a well-defined fusiform lesion, 10 × 8 × 19 mm, appearing to arise from and remain contiguous with the radial nerve within the spiral groove, with intermediate T1/T2 signal and no invasion of adjacent structures (Figure 1). These features were interpreted as most consistent with a benign nerve sheath tumor. Nerve conduction studies showed markedly reduced radial nerve conduction velocity, and electromyography of radially innervated muscles demonstrated fibrillations, positive sharp waves, and severely reduced recruitment, attributed to mass effect.
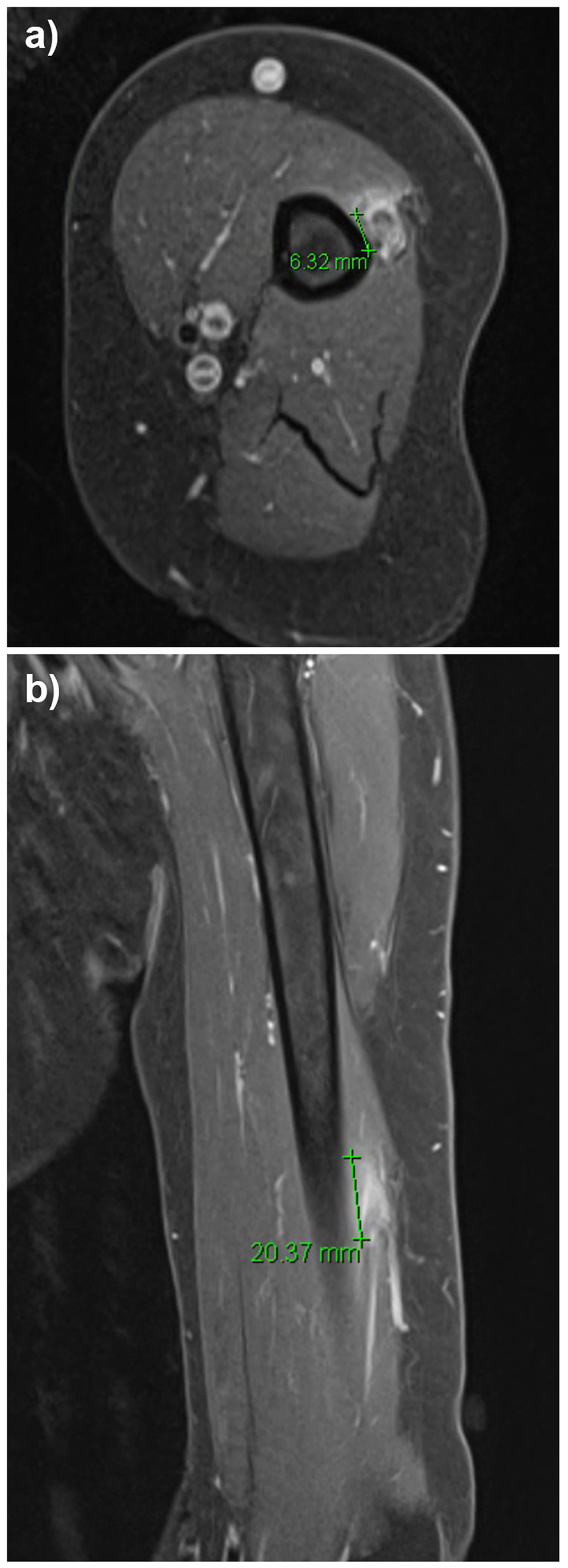
(A) Axial and (B) Coronal contrast-enhanced magnetic resonance imaging (MRI) of the left arm demonstrating a fusiform lesion (marker) arising from and contiguous with the radial nerve in the spiral groove.
Surgical Approach
The patient was taken to the operating room for presumed tumor excision and open biopsy. On the day of surgery, the mass was subjectively smaller, although the neurological examination was unchanged. Through a longitudinal posterior approach to the spiral groove, fibrous constricting bands were identified over the radial nerve and fully released. Exploration revealed no discrete tumor; instead, the nerve demonstrated diffuse swelling, hyperemia, and fusiform enlargement consistent with a resolving pseudoneuroma secondary to compression neuropathy (Figure 2). Intraoperative nerve stimulation proximal to the compressed segment produced no response, whereas stimulation distally elicited wrist and finger extension. Given these findings, the planned intraneural biopsy was aborted, and decompression of the radial nerve throughout the spiral groove was completed. At 6-month follow-up, MRI demonstrated complete resolution of the mass-like enlargement, and the patient had recovered full motor and sensory function without residual deficit. There has been no evidence of recurrence at the 5 year post-operative follow-up.

Intraoperative view of the radial nerve in the spiral groove postdecompression with no evidence of a nerve tumor.
Conclusion
This case highlights that acute radial nerve palsy with a palpable mass in the spiral groove may represent a pseudoneuroma from focal compression rather than a true nerve sheath tumor. Compression neuropathy can produce intraneural swelling and fusiform enlargement that closely mimics a benign neoplasm on MRI.1,2 When intraoperative findings are incompatible with a tumor, surgeons should be prepared to prioritise nerve preservation by performing thorough decompression and reconsidering or aborting intraneural biopsy to avoid iatrogenic injury. Careful correlation of clinical, radiologic, and intraoperative findings is essential to distinguish pseudoneuroma from neoplasm and to guide appropriate management.3–5
Footnotes
Authors’ Contribution
Colin McInnes provided the clinical case. Both Rebecca Z. Xu and Colin McInnes contributed to the writing and editing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent Statement
Written informed consent was obtained from the patient for publication of this case and the accompanying images.