
Abstract
Introduction
Prominent ear is the most common congenital variance of the head and neck occurring in approximately 5% of the general population.1,2 Children with prominent ears frequently experience low self-confidence, negative body image, and difficulties with social interaction. 3 These factors frequently motivate children and their parents to seek surgical intervention for the affected child. As surgical indications for prominent ears often revolve around improving self-confidence and ear appearance, it is important to understand how otoplasty impacts patients’ quality of life (QoL).
In general, otoplasty techniques are divided into 2 categories: cartilage cutting and cartilage sparing (suturing) techniques. The Mustardé technique, a common cartilage sparing technique, involves placing conchoscaphal sutures through the cartilage to create an anti-helical fold and correct the deformity. 4 This technique is known for being effective, safe, and cost-efficient.4,5
.
Several studies have found patients report improved QoL following otoplasty6–11 using the self-reported Glasgow Benefit Inventory (GBI) 12 and the parent-reported Glasgow Children's Benefit Inventory (GCBI). 13 The EAR-Q is a condition-specific patient-reported outcome measure (PROM) for children and young adults with differences in ear appearance. 14 The EAR-Q ear appearance scale specifically measures satisfaction with ear appearance, health-related QoL, and adverse effects before and after otoplasty. As the EAR-Q is a recently developed questionnaire, there is limited literature on its application for patients undergoing otoplasty for prominent ears.
To date, there is a paucity of research specifically examining how the Mustardé otoplasty technique affects QoL in relation to surgical indications and patient perspectives on post-operative ear appearance. The primary objective of this study was to describe QoL and postoperative satisfaction with ear appearance for patients who have undergone Mustardé otoplasty using the GBI/GCBI and EAR-Q ear appearance scale. Secondary objectives were to determine whether indication for surgery and post-operative ear appearance satisfaction is associated with patient-reported QoL.
Methods
This study was designed as a mixed methods study incorporating a 14-year retrospective chart review and prospective QoL questionnaires. The study was approved by the University of British Columbia (UBC) Children's and Women's Research Ethics Board (H24-01277). Informed consent was obtained from each participant and/ or their legal guardian.
Patients
Eligible patients were identified from the senior author's (J.A.) surgical database. Patients with a diagnosis of prominent ear(s) who had undergone a Mustardé otoplasty by the senior author at British Columbia Children's Hospital from January 2009 to September 2023 were invited to participate. Exclusion criteria were patients not fluent in English, or patients with less than 6 months post-operative follow-up.
Data Collection
Patient demographic data were collected, including patients’ sex, age, relevant medical comorbidities, pre-operative physical findings, and surgical indications (ie, peer ridicule, parental preference, or patient self-concern). Operative data included original surgery data, age at time of surgery, procedure details, other procedures at time of otoplasty. Post-operative data collected were complications, number of revisions, and follow-up time.
Questionnaires
Participants who consented were invited to complete questionnaires according to their age, outlined in Table 1. Questionnaires were completed over the phone or online using a secure UBC Qualtrics link. No incentives were offered for participating.
Questionnaire Administration.
The GBI is a validated retrospective questionnaire designed specifically to measure patient-reported changes in health-related QoL following an intervention. It consists of 15 questions measured individually on a 5-point Likert scale. The revised 5 factors analysis of the GBI divides questions into categories of support, general health, QoL, self-confidence, and social involvement. 15 These factors help determine which specific areas were affected by the surgical intervention. The total score and 5 factors are calculated and linear-transformed to a scale from −100 (maximal negative effective) to +100 (maximal positive effect). The GCBI is a parent-proxy version of the GBI for participants less than 14 years old. It consists of 24 questions scored individually on a 5-point Likert scale that are linearly transformed to a scale of −100 to +100.
Due to the generic nature of the GBI, the EAR-Q appearance scale was used in conjunction to collect ear specific outcomes post-operatively. The EAR-Q appearance scale is a validated questionnaire for assessing how satisfied patients are with their ears and their overall appearance. 14 It consists of 10 questions measured on a 4-point Likert scale. Question response values are added together and Rasch transformed to a scale of 0 (worst) to 100 (best).
Surgical Technique
All patients had surgery performed under general anesthesia, with perioperative antibiotic prophylaxis and local anesthesia with epinephrine administered. A retroauricular elliptical incision was made on the posterior surface of the ear to access the underlying cartilage. The posterior surface was skeletonized, conchal bowl reduction was performed at this stage of the operation for indicated ears. Mustardé conchoscaphal and/or concho-fossa triangularis horizontal mattress sutures were placed using 4-0 clear nylon sutures, and secured under appropriate tension to replicate a symmetric degree of natural ear prominence and antihelical fold correction. The head was wrapped for the first week and a protective headband was worn for 2 months postoperatively, with a graduated return to sports and avoidance of trauma during this interval.
Statistical Analysis
Data collected from chart review were cleaned by reviewing entries for completeness and consistency. Information was categorized into standardized fields, non-relevant information was removed, and questionnaire data was reviewed for completeness. Demographic and clinical characteristics were tabulated with means or medians for continuous variables, and frequencies for categorical variables. Surgical indications were categorized as patient concern (ie, self-consciousness), parent concern, peer concern (ie, teasing), or pain. General concerns were defined as the presence of any of combination of these indications. GBI and GCBI were combined for statistical analysis. GBI, GCBI, and EAR-Q appearance scores (Rasch Transformed) were illustrated using box plots and summarized using means with standard deviations, and medians with interquartile ranges. Both mean and median values were reported for the following reasons: means allowed for comparisons to previous literature that reported means, and medians were also reported as suggested by the GBI/ GCBI creators since the data is unlikely to be normally distributed. 15 Relationships between QoL scores and participant, operative factors, outcomes, complications, and surgical indications were assessed using univariate linear regressions with statistical significance set at P = .05. Patients were then sub-grouped by surgical procedure, Mustardé only or Mustardé with conchal reduction, to assess operation type on GBI/ GCBI and EAR-Q appearance scores. A Spearman's correlation was done between the GBI/ GCBI and EAR-Q appearance scores.
Results
Over the 14-year period, 71 patients met the inclusion criteria, 49 consented to participate and 42 completed both GBI/ GCBI and EAR-Q questionnaires (response rate, 59%). Eighteenpatients (43%) were male, and 24 patients were female (57%) (Table 2). The mean age at the time of operation was 10.1 years old. Ten patients had unilateral operations (23.8%) and 32 had bilateral operations (76.2%). The mean number of Mustardé sutures used per ear was 2.5 sutures. The mean duration from operation to questionnaire completion was 9.0 ± 3.8 years (range, 1.9-15 years). There were 12 complications across a total of 87 ears in the cohort (13.8%), all of which were minor complications consisting of suture extrusion, and 2 patients requiring a revision for asymmetry. There were no complications of a hematoma or an infection (Table 2).
Patient Demographics and Operative Data.
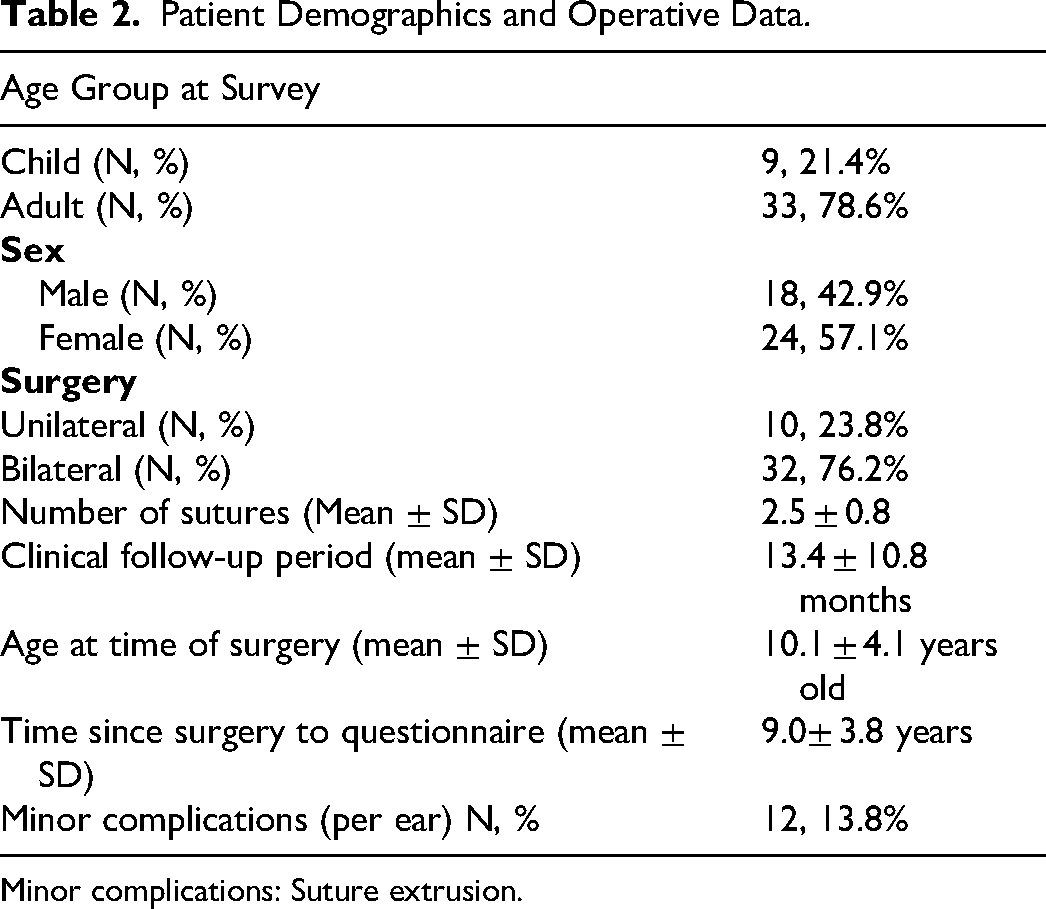
Minor complications: Suture extrusion.
Quality of Life
Out of the 42 patients, 33 completed the GBI and 9 completed the GCBI. The median GBI score was 30.0 (16.7, 46.7) and median GCBI score was 33.3 (17.7, 44.8), indicating an improvement in QoL from the operation (Table 3 and Figure 1). Only one patient reported a negative GBI score. In a follow-up phone call, this patient described lasting sensitivity behind her ears negatively affecting her overall QoL.
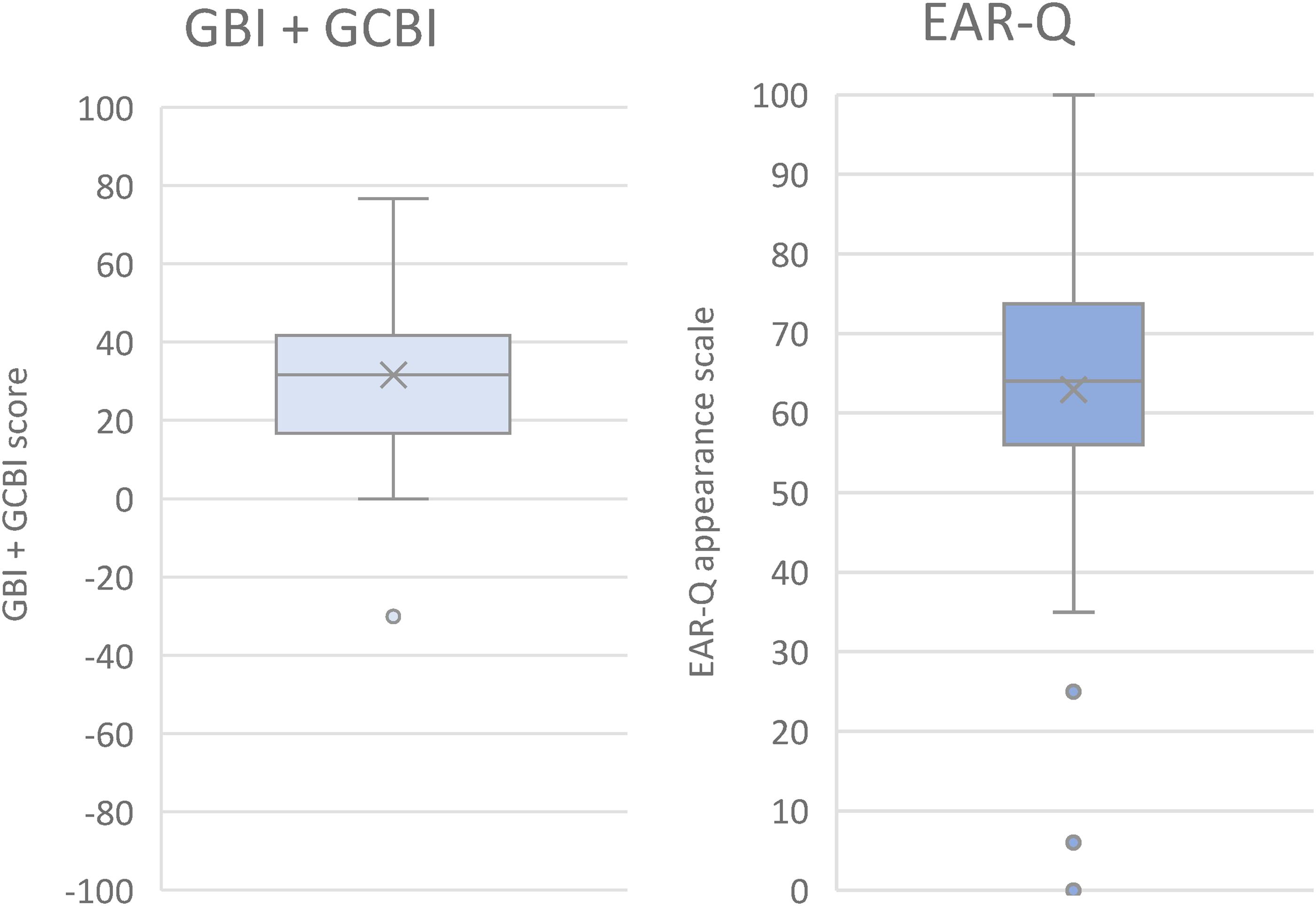
Box plot of GBI/ GCBI scores and EAR-Q scores. Horizontal line represents the median and X represents the mean. Circles represent outliers. Abbreviations: GBI: Glasgow Benefit Inventory; GCBI: Glasgow Children's Benefit Inventory.
GBI and GCBI Scores.
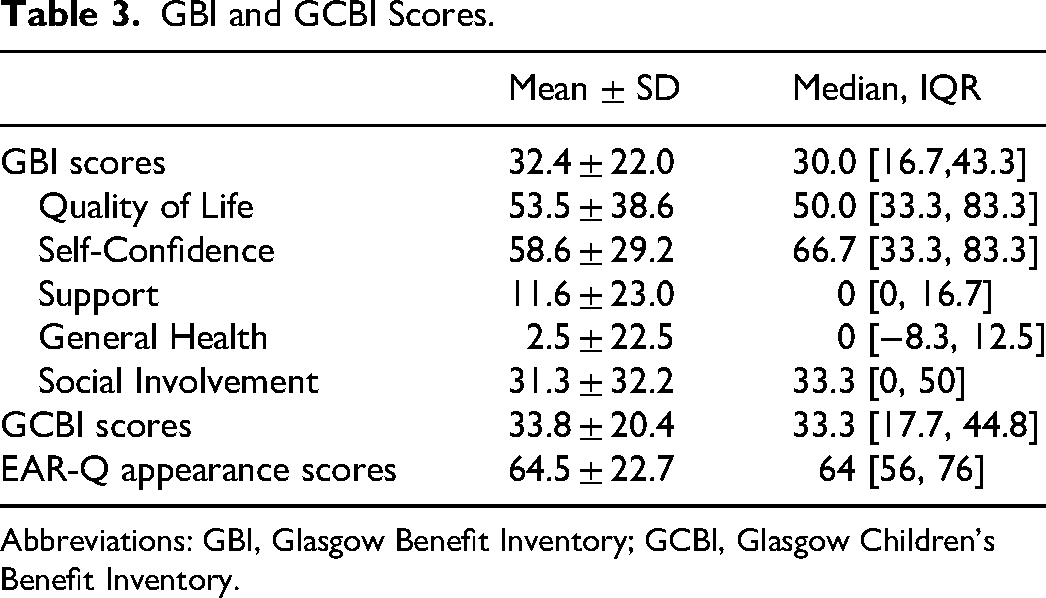
Abbreviations: GBI, Glasgow Benefit Inventory; GCBI, Glasgow Children's Benefit Inventory.
The median EAR-Q appearance score was 64 (56, 76), with 82.2% having an EAR-Q appearance score above 50, indicating high levels of post-operative satisfaction with ear appearance (Figure 1). There were no significant differences in QoL scores by sex (P = .682), age at surgery (P = .789), or time between surgery to questionnaire completion (P = .855). There were also no significant differences in EAR-Q scores by sex (P = .475).
The Mustardé only procedure was associated with a higher GBI/GCBI score (8 points) and higher EAR-Q appearance score (14 points) compared to Mustardé with conchal reduction, but these differences were not statistically significant (P = .221 and P = .07).
The GBI QoL and self-confidence subscales had the highest scores (median, 50.0 and 66.7 respectively), followed by the social involvement subscale median increase of 33.3 (Figure 2). The subscales support and general health increased the least (median, 0 and 0 respectively).
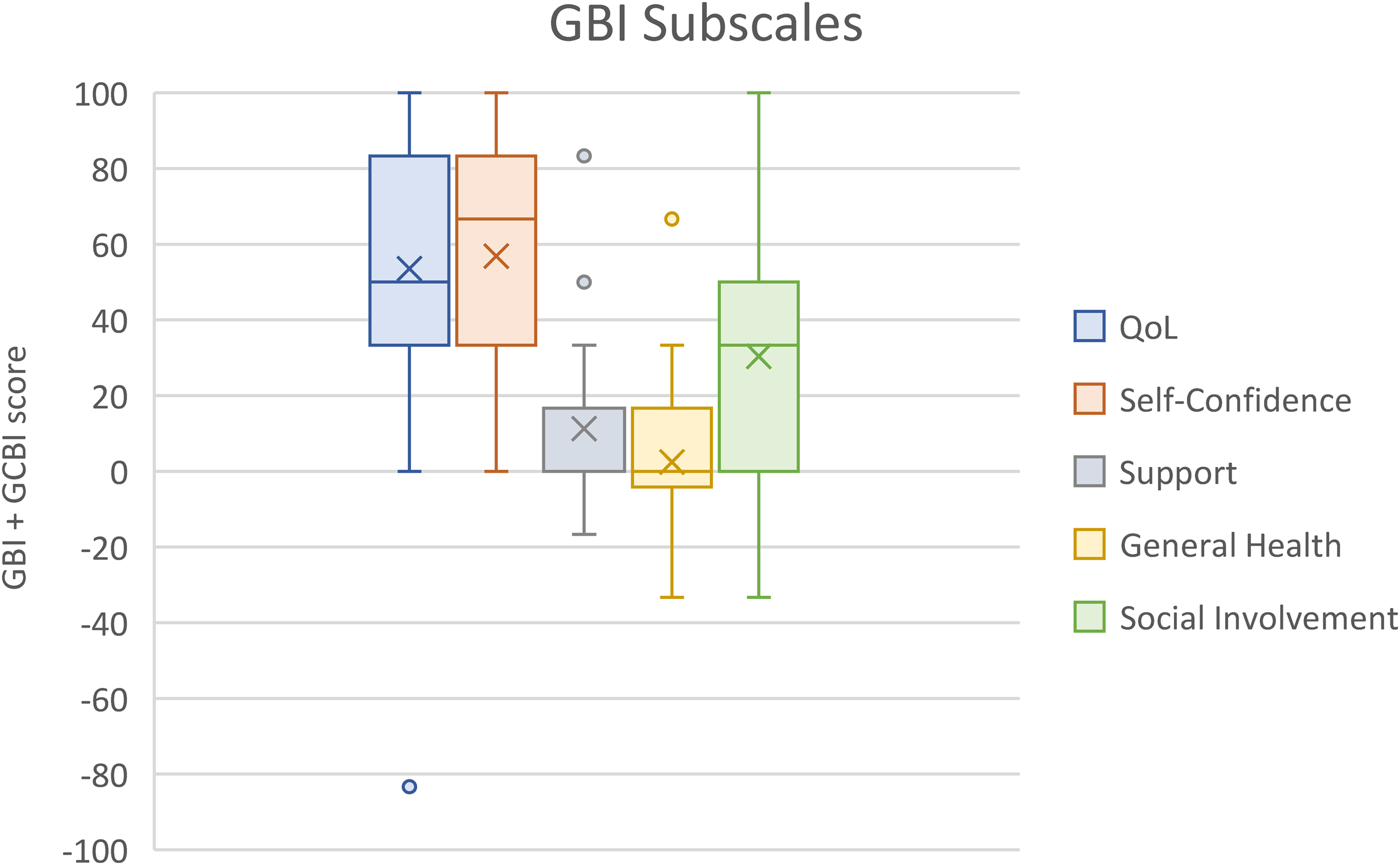
Box plot of GBI subscale scores. Horizontal line represents the median and X represents the mean. Circles represent outliers. Abbreviations: GBI: Glasgow Benefit Inventory; GCBI: Glasgow Children's Benefit Inventory; QoL: quality of life.
Surgical Indications & QoL
Nearly all patients (90%) had a general psychosocial concern that caused them to seek out surgery, these were further categorized as: peer concern, parent concern, and patient concern. The main indication for surgical interventions was patient concern (self-consciousness) about their ear appearance (29, 59.2%), followed by teasing (20, 40.8%), and parental concerns (14, 28.6%). Of note, pain was an indicator for 6.1% of patients.
Patients who reported self-consciousness as a reason for surgery reported a higher QoL on the GBI/GCBI (mean 13.8 points higher) than patients who did not report self-consciousness as a reason for surgery (P = .04). The other pre-operative indications did not demonstrate any significant influence on the GBI/GCBI scores (Figure 3). None of the indications for surgery had a significant effect on EAR-Q appearance scale scores.
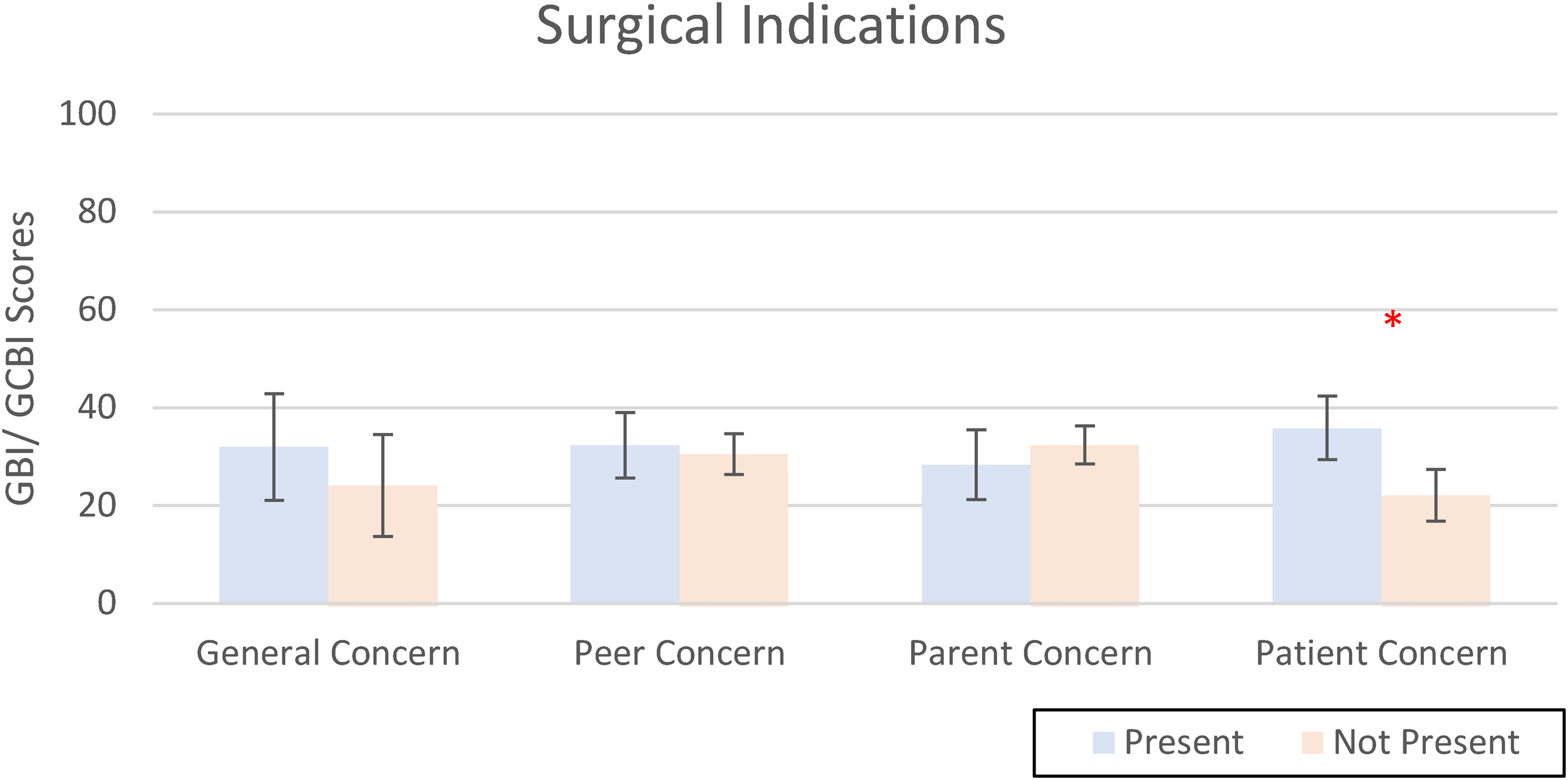
Bar graph representing the results of a linear regression that determined whether the presence of a specific patient-reported indications affected overall GBI scores. Asterisks denotes a significant difference between the presence and lack of self-consciousness (P = .04). Abbreviations: GBI: Glasgow Benefit Inventory; GCBI: Glasgow Children's Benefit Inventory.
GBI/GCBI and EAR-Q Correlation
A Spearman correlation was done to assess the relationship between GBI/GCBI and EAR-Q appearance scores and a moderate positive correlation was found (rho = 0.50, P = .0007) (Figure 4).
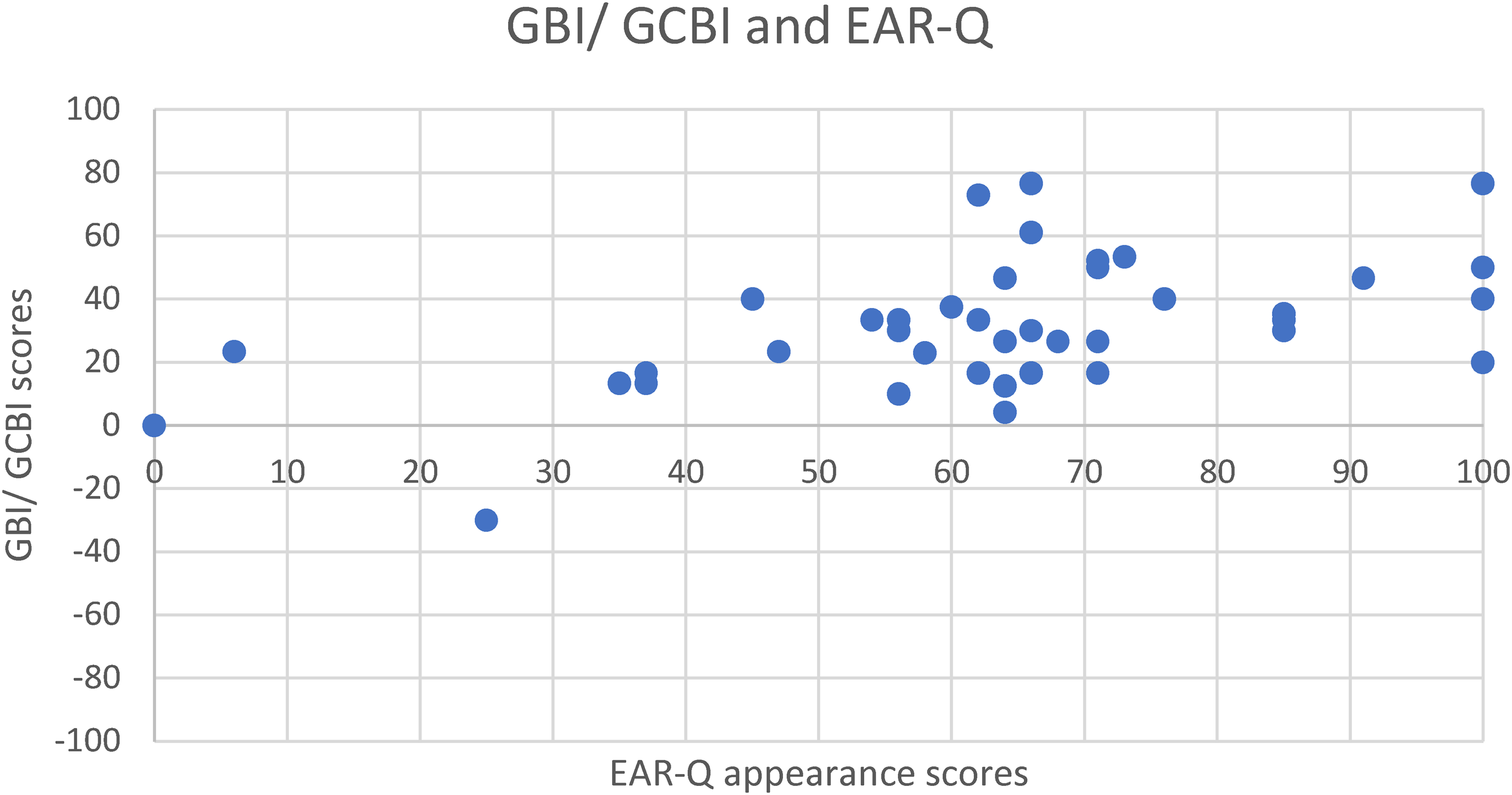
Scatter plot showing the relationship between GBI/ GCBI and EAR-Q appearance scores. Spearman’s correlation showed a moderate positive relationship between the scores (rho = 0.50, P = .0007). Abbreviations: GBI: Glasgow Benefit Inventory; GCBI: Glasgow Children's Benefit Inventory.
Discussion
Our findings suggest that the Mustardé otoplasty improves general QoL and leads to high levels of satisfaction with ear appearance for majority of patients. This is represented by the positive GBI and GCBI scores, with a median of 30.0 for participants 14 years and older and a median of 33.3 for children aged 8-13 years. More interestingly, we found that patients with personal concerns about their ears showed greater improvements in QoL compared to those whose primary concerns were reported by parents or peers.
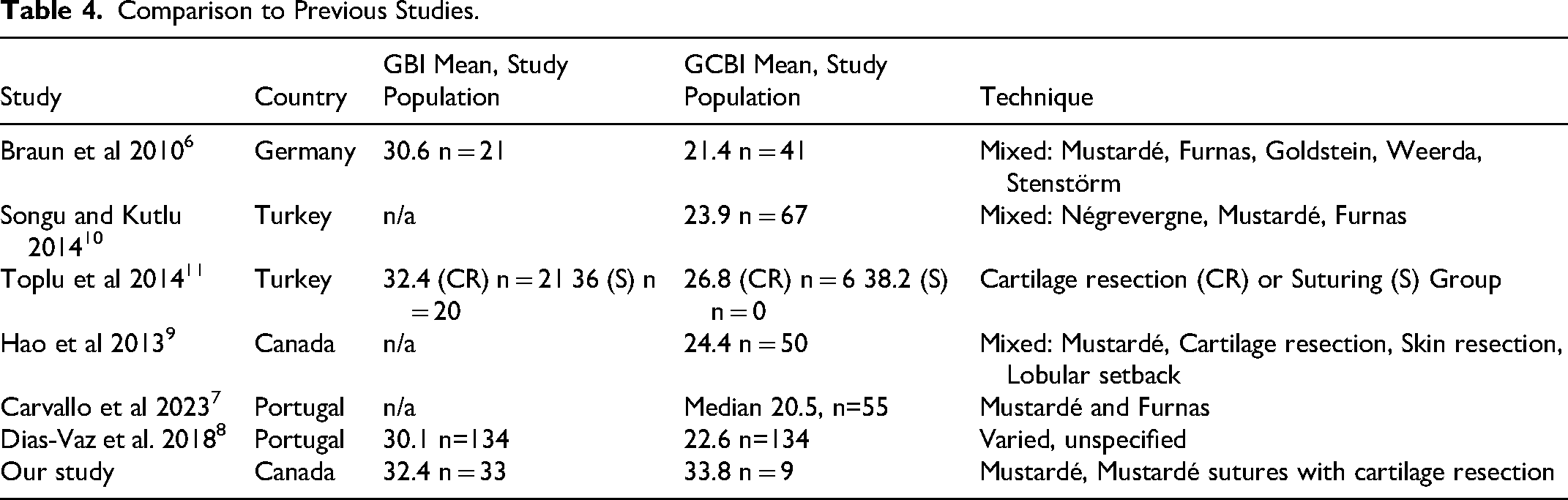
In comparison to the literature, the mean GBI/GCBI scores were comparable to published reports with varied surgical techniques and regional differences (Table 4). Although nearly all patients (41/42) reported that the Mustardé otoplasty improved their QoL, it is important to acknowledge the wide range of scores, including one patient having a negative score. On the EAR-Q appearance scale, 78.6% (33/42) reported to be satisfied with their ear appearance after their surgery. For the EAR-Q, no comparative values exist as ours is one of the first studies specifically applying the EAR-Q on patients with prominent ears. While the EAR-Q field testing did apply the scale on children with prominent ears, there was heterogeneity across the cohort with multiple different ear diagnoses. 16
Comparison to Previous Studies.
When evaluating our surgical technique, neither the addition of a conchal bowl reduction nor the number of Mustardé sutures placed (both surrogates of the severity of the prominent ears) demonstrated no significant differences in the GBI/GCBI or EAR-Q scores between patients. It is possible that our sample size was insufficient to detect a trend, as Toplu et al did report cartilage resection was associated with lower GBI/GCBI scores compared to the suture only group. 11 The differences in surgical methods between our study and Toplu et al may also account for this discrepancy. 11
Using the revised GBI factor analysis, 15 most factors were elevated with the exception of general health and support not being affected (Figure 2). Highest improvements were seen in general QoL and self-confidence aligning with existing literature that otoplasty can improve self-confidence and reduce self-consciousness in children, contributing to an increased QoL. 17
Importantly, patients who were personally concerned about their ear appearance experienced greater improvements in QoL scores compared to those whose concerns were primarily peer- or parent-driven. This observation is further supported by the GBI subscale analysis, where the highest increases were noted in the self-confidence domain. This contrasts previous research that linked teasing and bullying (peer concerns) with higher GBI/GCBI scores after otoplasty while parental concern and low self-confidence (patient concern) had no significant effect on GBI/GCBI scores. 9 Our findings may suggest that personal motivation has a bigger impact on perceived increases in QoL than previously thought and highlights an important consideration for clinicians when discussing the timing and indications of otoplasty with children and their caregivers. This may suggest the importance of shared-decision making in the pediatric realm and the importance of patient concern in guiding treatment. Our results suggest surgeons should wait until children are old enough to develop their own perception of the condition before undertaking surgery to achieve the greatest improvements in QoL.
There was also a moderate positive correlation between the GBI/GCBI scores and EAR-Q appearance scores, suggesting a possible relationship between the aesthetic satisfaction and overall positive impact on QoL. Therefore, the Mustardé otoplasty may be considered effective from both the surgical point of view and patient perspectives.
Limitations
There were several limitations in this study. Recall bias may have affected the scores as on average patients had 8.9 years from surgery to questionnaire completion. Nonetheless, the timing of questionnaire completion did not have a statistically significant effect on QoL scores and prior studies have demonstrated no significant differences in quality-of-life outcomes when comparing short- and long-term post-operative follow-up, suggesting that PROMs may remain stable over time.6,18 While both EAR-Q and GBI/GCBI were used to assess QoL, the retrospective nature of our study prevents a direct comparison of pre- and post-operative outcomes.
Future prospective studies combining pre- and post-operative EAR-Q with GBI/GCBI would create more comprehensive evaluation of patients’ QoL improvement. Using the EAR-Q and GBI/GCBI in a dynamic fashion such as prospective study would enable a more comprehensive evaluation of patients’ QoL improvement.
Self-selection bias may have been at play as patients who had a negative experience may have been less likely to participate. This may have skewed our results to be overly positive. The GCBI is parent report, and it's possible that parent-reported benefits may have been influenced by confirmatory bias where parents seek to validate decisions they made for their children. 9 Furthermore, the absence of a preoperative measurement of EAR-Q appearance limits our ability to fully assess the true impact of otoplasty on QoL.
Conclusions
The Mustardé otoplasty was found to improve QoL and satisfaction with ear appearance, consistent with other techniques performed, which suggests any otoplasty technique should yield good results from a patient's perspective. Furthermore, children experiencing self-consciousness as the indications for surgery were found to have the largest improvements in QoL after surgery. These findings may help guide conversations between patient and surgeon around surgical outcomes, timing of surgery, and post-operative QoL expectations. Finally, future studies should continue to explore these factors and consider integrating the EAR-Q pre and post operatively to better understand the effects of the Mustardé otoplasty on patient QoL.
Footnotes
Acknowledgments
We would like to thank all of the participants for contributing to this study and Sophia Shayan and Stephanie Cooper for their administrative support. We also would like to acknowledge the use of the EAR-Q, authored by Drs. Anne Klassen and Karen Wong, which was made under license from McMaster University, Hamilton, Canada.
Ethical Statement
This project was approved by the University of British Columbia Children's and Women's Research Ethics Board (H24-01277). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Consent to Participate
All participants provided informed consent.
Author Contributions
Study conceptualization and design was led by JA and supported by SRB, RC, and MB. SRB and RC contributed to data collection and analysis. SRB drafted the initial manuscript. All authors contributed to data interpretation, manuscript writing and editing, and approved the manuscript version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sue Rim Baek was awarded a University of British Columbia Summer Student Research Program Award. Dr Jugpal Arneja was supported by a UBC Surgery Clinical Faculty Research Support Award.
Presentations
2025 Western Medical Research Conference, January 16-18, 2025; Carmel, California.