
Abstract
This is a visual representation of the abstract.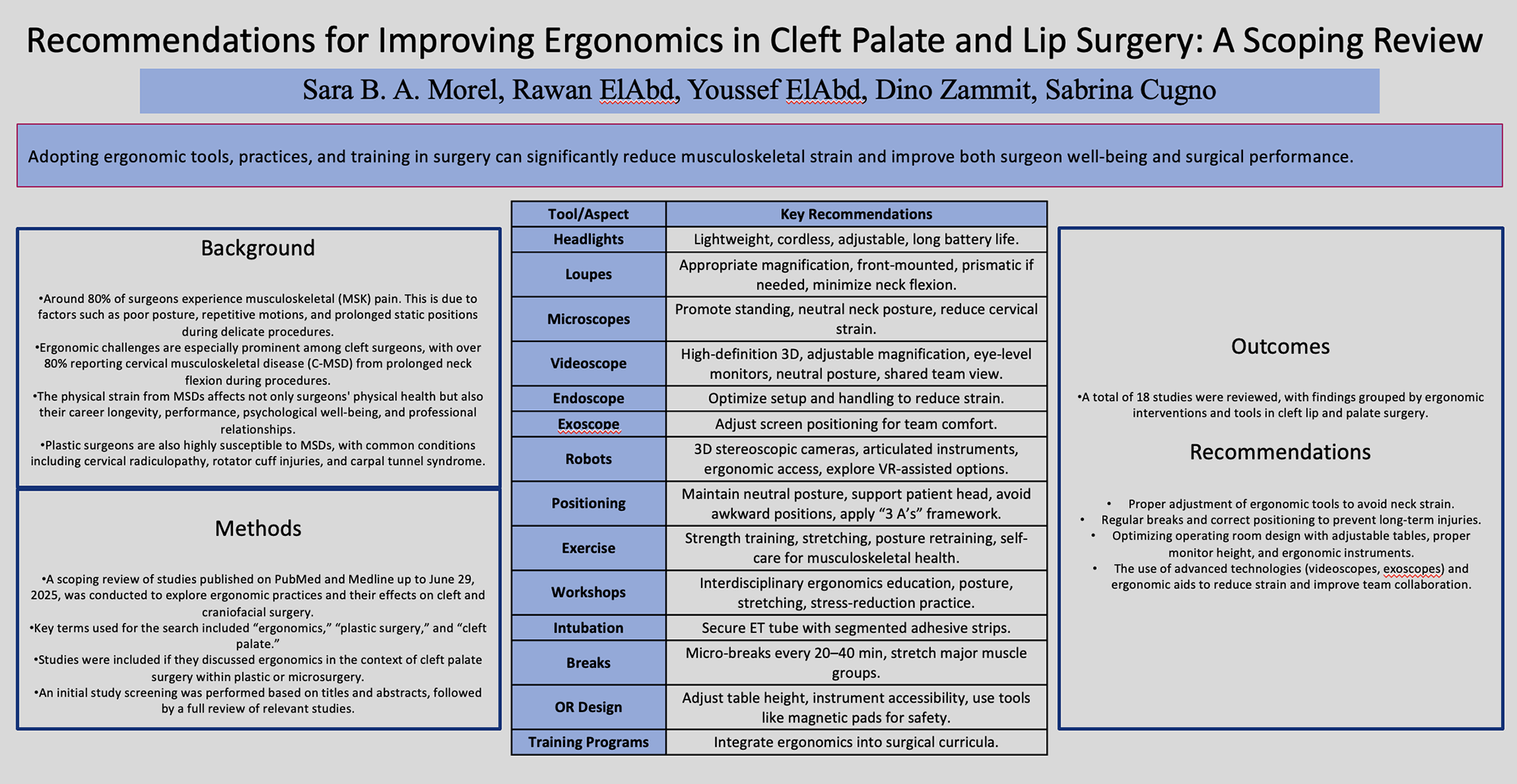
Keywords
Introduction
Occupational injuries are defined as damage from work-related events. 1 Surgeons, particularly in demanding specialties like plastic surgery, face high risks of musculoskeletal disorders due to poor posture, repetitive motions, and prolonged static positions during delicate tasks.2–4
Around 80% of surgeons experience musculoskeletal (MSK) pain while operating, with over 30% sustaining occupational injuries and 9% ending their careers prematurely due to these issues.5,6 These injuries impair performance career longevity, psychological well-being, relationships, and sleep, increasing the risk of errors.6–12
Over 80% of cleft surgeons report cervical musculoskeletal disease (C-MSD) from prolonged neck flexion required for visualizing the palate.2,13 The small intraoral visual field further complicates visibility, limiting team interaction and learner participation.14–16
Surveys reveal that 64.2% of cleft surgeons experience MSK injuries, with neck (82%), lower back (56.6%), and shoulder (54.1%). 10 These issues often lead to surgery (31%), sick leave (27%), or even early retirement (9.2%).10,17 Ergonomic practices, such as taking breaks, improving positioning, and mindfulness techniques, are essential for reducing these risks. 17
Plastic surgeons are highly susceptible to MSDs, with 5% suffering from cervical radiculopathy and disc herniation and 4% of them undergoing discectomy and 2% requiring cervical fusion. 3
Poor ergonomics, particularly sustained downward gaze during long surgeries, exacerbates cervical strain, especially when using loupes or headlamps.18,19 Other common MSDs include rotator cuff issues (18%) and carpal tunnel syndrome (9%), often caused by repetitive motions, forward head posture and static positions.6,20 This scoping review aims to elucidate different mechanism used to improve ergonomic in cleft surgery, providing new recommendations for reducing surgeon strain.
Materials and Methods
This scoping review involved a comprehensive search of the literature in PubMed, Ovid, and CINAHL databases, from their inception up until June 29, 2025. The search used the following key terms: “cleft,” “cleft palate,” “cleft lip,” and “ergonomics.” The full search strategy is outlined in Supplementary Figure 1. To be eligible for inclusion, studies had to specifically address strategies and methods for improving ergonomics in cleft lip and palate surgery. The initial screening of titles and abstracts was carried out independently by two reviewers (S.B.AM and R.E.), with any disagreements resolved through discussion. Only full-text articles describing interventions related to surgical ergonomics were included in the analysis. Additionally, the references of all included articles were reviewed to identify further studies for possible inclusion.
Data extraction was performed using a standardized Microsoft Excel spreadsheet (Redmond, Washington, USA).
21
The initial extraction was done by one reviewer (S.B.AM
Risk of Bias Assessment
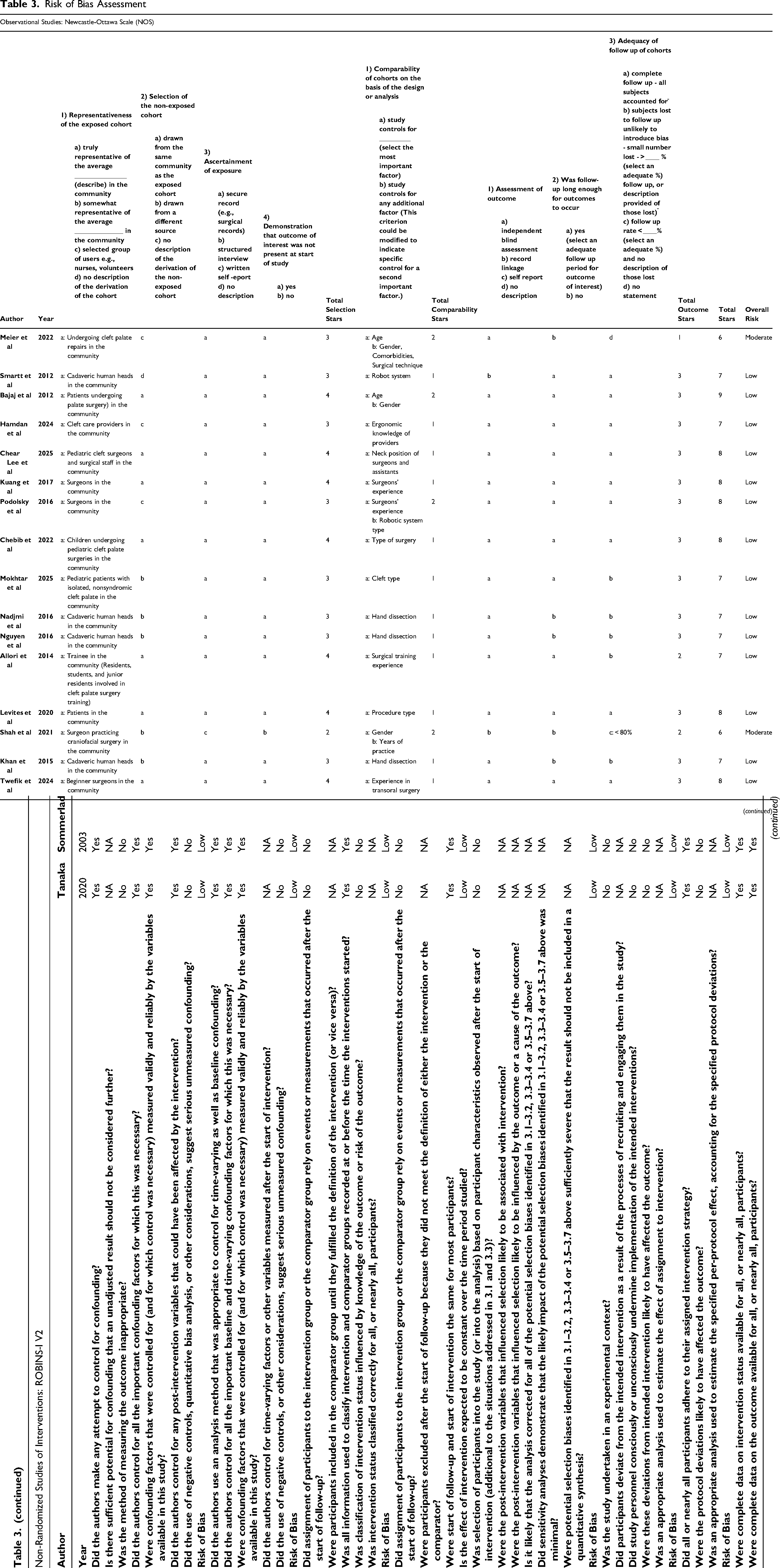
We performed a risk of bias (ROB) assessment for all studies included in our review. For observational cohort studies, we used the Newcastle-Ottawa scale (NOS), 23 while the risk of bias in non-randomized studies of interventions (ROBINS-1 V2) 24 was applied to non-randomized intervention studies.
Results
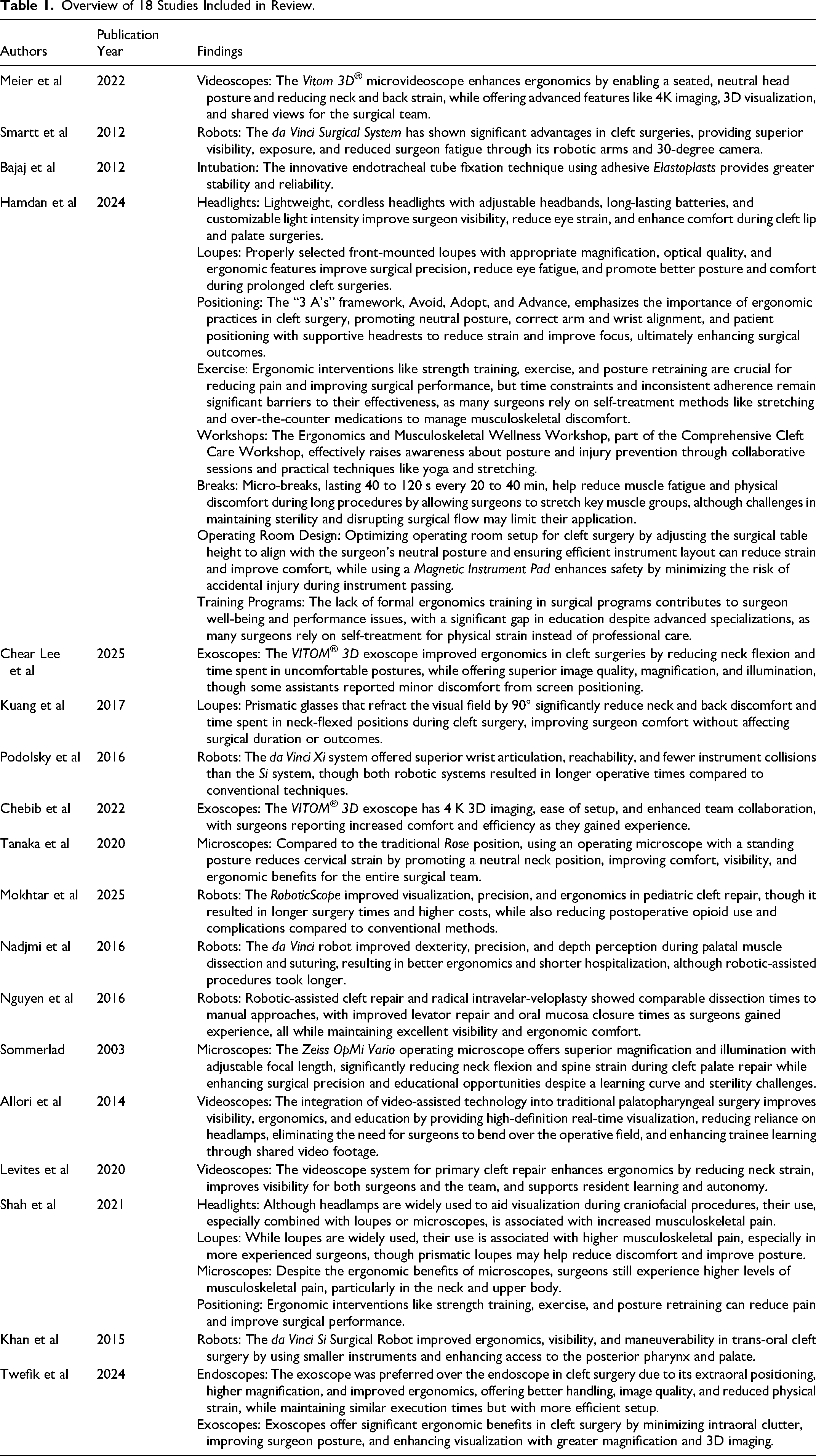
A total of 18 studies were compiled into Table 1. Out of the studies, 2 were non-randomized observational studies,25,26 2 were retrospective cohort studies,10,27 and 14 were prospective cohort studies.16,17,28–39 The number of studies investigating each ergonomic strategy for cleft surgery is as follows: headlights: 210,17; loupes: 310,17,32; microscope: 310,25,26; robot: 627,29,33,35,36,38; videoscope: 4;16,28,37,39 endoscope: 1 39 ; exoscope: 331,34,39; head/neck positioning: 210,17; breaks: 1 17 ; exercise: 210,17; workshops: 1 17 ; intubation: 1 30 ; OR design: 1 17 ; and training programs: 2.10,17 A summary of the findings for each recommendation category can be found in Table 2.
Overview of 18 Studies Included in Review.
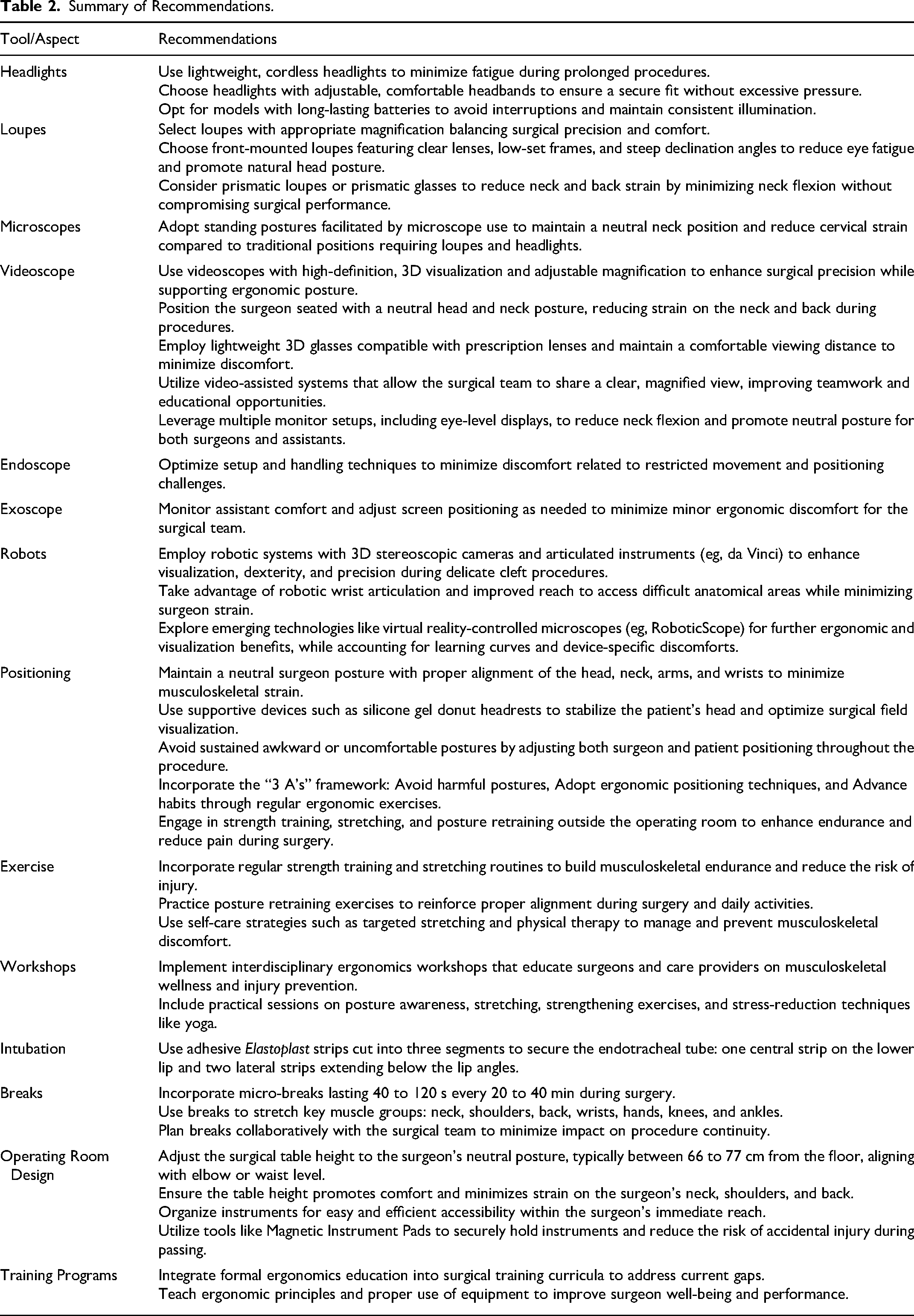
Summary of Recommendations.
Risk of Bias Assessment
As outlined in Table 3, The ROBINS-1 V2 tool was applied to 2 studies,25,26 while the Newcastle-Ottawa Scale (NOS) was used in 16 studies.10,16,17,27–39 Overall, 88.89% (n = 16) of the studies were classified as low risk, while 11.11% (n = 2) were classified as moderate risk. The higher risk studies were primarily due to the absence of a comparison group.
Risk of Bias Assessment
Discussion
Ergonomic Recommendations for Surgeons
Headlights
Hamdan 17 evaluated ergonomic strategies aimed at enhancing surgeon comfort and efficiency during cleft lip and palate surgeries. A central recommendation was the use of lightweight, cordless headlights equipped with adjustable headbands, long-lasting batteries, and customizable light intensity. These features collectively enhance visibility, reduce eye strain, and improve overall comfort.
Shah 10 investigated MSK symptoms and ergonomic practices among members of the American Cleft Palate-Craniofacial Association. In a survey of 873 surgeons, 79.5% reported using headlamps during craniofacial procedures. While these devices aid in visualization, their use, particularly when combined with loupes or microscopes, was associated with higher reported pain scores.
Loupes
Hamdan 17 emphasized the critical role of properly selected loupes in cleft lip and palate surgery, highlighting the importance of magnification strength, optical quality, and ergonomic design. Front-mounted loupes with 2.5×, 3.5×, or 4.5× magnification were recommended for their ability to enhance surgical precision while maintaining comfort. Key ergonomic features, such as clear lenses, low-set frames, and steep declination angles, not only improve visualization but also help reduce eye fatigue. These loupes promote a wider working distance, which facilitates better arm positioning and contributes to sustained ergonomic posture during complex, prolonged procedures.
In a broader survey, Shah 10 found that 83.2% of surgeons used loupes in practice. However, those who did report higher pain scores compared to users of headlights or microscopes. Notably, surgeons with over 15 years of experience had nearly twice the odds of reporting MSK symptoms, underscoring the long-term physical toll of poor ergonomic practices.
Supporting these findings, Kuang 32 examined the use of prismatic glasses, which refract the visual field by 90°, in cleft palate surgeries performed by oral-maxillofacial surgeons. In a controlled comparison involving three surgeons and six patients, the use of prismatic glasses led to significantly reduced neck and back discomfort, along with less time spent in neck-flexed positions. Importantly, these ergonomic benefits were achieved without compromising surgical duration or outcomes.
Microscopes
Sommerlad 26 explored the use of the Zeiss OpMi Vario 40 operating microscope in cleft palate repair, highlighting its advanced features such as a tiltable binocular, beam splitter, teaching arm, and integrated video camera. This microscope provides superior magnification and illumination compared to traditional loupes or headlights, while its adjustable focal length allows for precise visualization. Critically, it supports improved neck ergonomics by minimizing the flexion required during prolonged procedures. The system also enhances the educational experience, enabling assistants and trainees to follow the procedure via the teaching arm or video monitor. While there is a learning curve and initial manual adjustments can be time-consuming, the ergonomic and visual benefits, along with improved surgical precision, make it a valuable asset.
Tanaka 25 compared the traditional Rose position with a standing posture facilitated by the operating microscope in cleft surgery. The Rose position, which involves considerable neck flexion to accommodate loupes and headlights, was associated with increased cervical strain. In contrast, the standing posture allowed by the microscope helped maintain a neutral neck position, improving comfort and reducing MSK stress for both surgeons and assistants. The microscope also promoted visibility and posture, regardless of height. While the setup requires specialized training and may not be feasible in all resource settings, its benefits in ergonomics were evident.
However, Shah 10 reported that despite these advantages, surgeons using microscopes still experienced higher levels of MSK pain, particularly in the neck and upper body. These findings underscore the importance of proper ergonomic training and techniques, even when using tools designed to improve posture and visualization.
Videoscope
Meier 28 evaluated the Vitom 3D®(StorzEndoscope) microvideoscope across eight consecutive cleft palate repairs, highlighting its advanced features such as 4K imaging, 3D visualization, and 30× magnification, all controlled via a sterile joystick. This system improved surgeon ergonomics by enabling a seated position with a neutral head posture, significantly reducing neck and back strain. Lightweight 3D glasses, compatible with prescription lenses, and a comfortable 2-m viewing distance further minimized discomfort. Additional benefits included enhanced image clarity, precise surgical performance, and a shared 3D view for the entire surgical team, which supported teamwork and education.
Allori 37 examined the integration of video-assisted technology into traditional palatopharyngeal surgery to enhance visibility, ergonomics, and education. Maintaining the conventional position with the surgeon at the patient's head, the setup incorporated a high-definition laparoscope connected to a video tower for real-time visualization. Using a flexible Endocameleon scope 41 positioned upside down to match the surgeon's perspective, this approach optimized lighting and oropharyngeal views while allowing smooth transitions between conventional and video-assisted methods. The video footage was recorded to create an educational library for asynchronous learning. Benefits included improved visualization and better ergonomics by eliminating the need to bend over the operative field.
Levites 16 investigated a videoscope system for cleft repair featuring a 5-mm, 30-degree high-definition laparoscope mounted on a holding arm. Surgeons could alternate between direct and video-assisted views, with images displayed on multiple monitors, including one positioned at eye level. This setup improved ergonomics by reducing neck strain and enhanced visibility for both surgeons and the surgical team. Despite greater resident involvement, operative times remained comparable. Advantages included increased surgeon comfort, superior visualization, enriched resident learning, and real-time monitoring via multiple room monitors that allowed residents greater autonomy while enabling detailed feedback from attending surgeons. Additionally, the system improved operating room efficiency and generated an educational video archive. The primary drawbacks were the need for additional equipment and setup time.
Endoscope
Twefik 39 compared endoscopes and exoscopes in cleft surgery. Execution times were similar, but the exoscope had a clear advantage in setup. Feedback from questionnaires showed that the exoscope was less demanding, with higher satisfaction ratings for setting, handling, image quality, and 3D capabilities. Both devices improved ergonomics by reducing physical strain, but the exoscope was preferred due to its extraoral positioning, higher magnification, and reduced intraoral encumbrance. Endoscopes are commonly used in cleft surgeries for their compact size and high-quality 2D/3D images, but their rigid positioning and intraoral placement can limit mobility.
Exoscopes
Exoscopes provide notable ergonomic advantages over traditional endoscopes in cleft surgery. Their extraoral placement minimizes intraoral clutter, allowing surgeons to maintain a more natural and comfortable posture. Additionally, the enhanced magnification and 3D imaging capabilities of exoscopes improve visualization of critical anatomical structures, which is essential for successful repairs. 39
Chear Lee 31 investigated the ergonomic benefits and surgical outcomes of the Vitom3D®exoscope in pediatric cleft surgeries, comparing its performance to conventional tools such as loupes and microscopes. The study measured surgeons’ neck flexion angles during procedures. Use of the Vitom3D®exoscope significantly reduced the time spent in ergonomically unfavorable postures (less than 10% compared to 93% with traditional loupes) and enhanced overall working ergonomics. Surgeons rated the exoscope highly for image quality, magnification, illumination, and ergonomic comfort, although some assistants reported minor discomfort related to screen positioning.
Similarly, Chebib 34 evaluated the Vitom3D®exoscope across a range of pediatric surgeries, including cleft repairs. Surgeons compared the exoscope to microscopes and loupes on factors such as ease of setup, visualization, lighting, and comfort. The exoscope was strongly preferred, with 94%–97% of surgeons rating it superior in all categories. Its 4 K 3D imaging and screen-based visualization not only enhanced surgical precision but also improved collaboration and communication among team members by allowing everyone to view the procedure on the same display. As surgeons gained experience with the device, they reported increased comfort and efficiency.
Robots
Robotic systems, particularly the da Vinci Surgical System, 42 have demonstrated significant promise in improving both precision and ergonomics in cleft palate and lip surgeries. Smartt 29 conducted cadaveric studies using the da Vinci system for posterior pharyngeal flap surgery, finding that the robotic arms and 30-degree camera offered superior visibility and exposure compared to traditional methods, while reducing surgeon fatigue. This early feasibility was expanded upon by Podolsky, 33 who used a high-fidelity simulator based on infant CT data to compare the da Vinci Si and Xi systems. The Xi system outperformed the Si with better wrist articulation, reachability, and fewer instrument collisions, although both systems resulted in longer operative times than conventional techniques. Further clinical application was demonstrated by Nadjmi, 35 who utilized the da Vinci robot for palatal muscle dissection in cadaver trials and then in 10 pediatric patients. The robot's 3D stereoscopic camera and EndoWrist instruments enhanced dexterity, precision, and depth perception, improving visibility during dissection and suturing. While robotic-assisted procedures averaged 122 min, longer than the 87 min of manual surgery, they provided better ergonomics and shortened hospitalization from 2.4 to 1 day. Similarly, Nguyen 36 investigated robotic-assisted cleft repair and radical intravelar-veloplasty in cadaveric heads, demonstrating comparable dissection times between robotic and manual approaches. With experience, surgeons improved levator repair and oral mucosa closure times while maintaining excellent visibility and ergonomic comfort. Khan 38 further explored the da Vinci Si Surgical Robot's feasibility for trans-oral cleft surgery in a pediatric airway manikin, testing various configurations to optimize access and safety.
More recently, Mokhtar 27 introduced the RoboticScope, 43 a 3D virtual reality microscope controlled via head gestures. Compared to conventional surgery, the RoboticScope improved visualization, precision, and ergonomics, though surgeries took on average 28 min longer. Importantly, patients in the robotic group required less postoperative opioid use and experienced no complications, contrasting with one uvula dehiscence in the conventional cohort. Despite its benefits, the RoboticScope high cost, learning curve, and potential discomfort from the head-mounted display pose limitations.
Positioning
Hamdan 17 emphasizes the critical role of ergonomic practices in healthcare, particularly in cleft surgery, introducing the 3 A's framework: Avoid, Adopt, and Advance. This approach encourages surgeons to avoid uncomfortable postures, adopt proper positioning techniques, and advance their ergonomic habits by incorporating exercises into their routines. In cleft palate surgery specifically, maintaining a neutral posture with correct arm and wrist alignment is essential for reducing strain and enhancing focus. Patient positioning is equally important, with the use of a silicone gel donut headrest to support the head and optimize surgical visualization.
Supporting this, Shah 10 highlights the value of ergonomic interventions such as strength training, exercise, and posture retraining to reduce pain and improve surgical performance over the long term. However, Shah also notes challenges surgeons face in committing time to these practices and sustaining ideal posture during lengthy procedures.
Exercise
Hamdan 17 found that ergonomic interventions, including strength training, exercise, and posture retraining, play a vital role in reducing pain, enhancing surgical performance, and supporting long-term health among surgeons. Complementing this, Shah 10 reported that surgeons commonly use self-treatment methods such as stretching, over-the-counter medications, and strength training to manage MSK discomfort. Treatments often involve physical therapy and diagnostic imaging. Shah's study highlighted that MSK issues frequently impair posture, stamina, and surgical speed, with nearly 30% of surgeons requiring prescription medications or injections. However, time constraints and inconsistent adherence remain significant barriers to the effectiveness of these interventions.
Workshops
This study by Hamdan 17 describes the Comprehensive Cleft Care Workshop, an annual interdisciplinary event that equips cleft care providers with evidence-based knowledge and technical skills. A key component, the Ergonomics and Musculoskeletal Wellness Workshop, addresses MSK challenges faced by providers through collaborative sessions led by surgeons, dentists, therapists, and psychologists. The workshop introduces ergonomic principles and practical techniques such as yoga, stretching, and strengthening exercises to promote long-term health and reduce injury risk. While the session effectively raises awareness about posture, technology use, and injury prevention, its brief two-hour duration may limit skill retention.
Intubation
Bajaj 30 presents an innovative method for endotracheal tube fixation during cleft lip and palate surgery using adhesive Elastoplasts, 44 cut into three segments, a 2 cm central strip fixed to the lower lip and two 1.5 cm lateral strips extending below the lip angles. This technique stabilizes the tube, prevents lateral movement, and eases mouth gag application, offering greater reliability than single-point adhesive methods.
Breaks
Hamdan 17 examined the impact of micro-breaks, lasting 40 to 120 s every 20 to 40 min. These breaks allowed surgeons to stretch key muscle groups, including the neck, shoulders, back, wrists, hands, knees, and ankles, while maintaining sterility. The practice was found to improve ergonomics by reducing muscle fatigue and physical discomfort during long procedures. However, potential drawbacks include the risk of disrupting surgical flow.
Operating Room Design
Hamdan 17 explored the ergonomic optimization of operating room setup for cleft surgery, focusing on surgical table height and instrument accessibility. It recommends adjusting the table to the surgeon's neutral posture, typically 66 to 77 cm from the floor, aligning with elbow or waist level, to promote comfort and reduce strain. The study also highlights the importance of efficient instrument layout and the use of a magnetic instrument pad to enhance safety by minimizing the risk of accidental injury.
Training Programs
Hamdan 17 highlights a gap in surgical education, noting the lack of formal ergonomics training. Incorporating ergonomic principles and equipment into training curricula could improve surgeon well-being and performance, while reducing the risk of MSK injuries. Supporting this, Shah 10 found that despite 71% of fellowship-trained surgeons having advanced specializations, only 7.4% reported formal ergonomics education. This significant shortfall reflects a broader reluctance to address ergonomic issues openly during training. Additionally, the study revealed that many surgeons, faced with demanding schedules, often rely on self-treatment for physical strain rather than pursuing professional care.
Conclusion
Collectively, the studies emphasize the multifaceted nature of ergonomic optimization in cleft surgery, highlighting that no single intervention suffices. Personal visualization aids improve precision but may still contribute to MSK strain if improperly used. Emerging technologies like videoscopes, exoscopes, and robotic systems show promise in enhancing both visualization and surgeon comfort, though they often require additional setup, training, and investment. Interventions targeting posture, scheduled micro-breaks, and physical conditioning complement equipment-focused strategies by addressing surgeon well-being holistically.
Nonetheless, limitations persist across the literature, including heterogeneous study designs, small sample sizes, and variability in outcome measures related to MSK symptoms. Additionally, few studies comprehensively evaluate long-term impacts or incorporate standardized ergonomic training, underscoring a critical gap in surgical education.
Future research should prioritize robust, controlled trials comparing ergonomic modalities with standardized outcome metrics and explore the integration of formal ergonomics curricula into surgical training. By continuing to refine and combine ergonomic strategies, the surgical community can better safeguard surgeon health while maintaining high standards of patient care in cleft lip and palate repair.
Supplemental Material
sj-docx-1-psg-10.1177_22925503251386782 - Supplemental material for Recommendations for Improving Ergonomics in Cleft Palate and Lip Surgery: A Scoping Review
Supplemental material, sj-docx-1-psg-10.1177_22925503251386782 for Recommendations for Improving Ergonomics in Cleft Palate and Lip Surgery: A Scoping Review by Sara B. A. Morel, Rawan ElAbd, Youssef ElAbd, Dino Zammit and Sabrina Cugno in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503251386782 - Supplemental material for Recommendations for Improving Ergonomics in Cleft Palate and Lip Surgery: A Scoping Review
Supplemental material, sj-docx-2-psg-10.1177_22925503251386782 for Recommendations for Improving Ergonomics in Cleft Palate and Lip Surgery: A Scoping Review by Sara B. A. Morel, Rawan ElAbd, Youssef ElAbd, Dino Zammit and Sabrina Cugno in Plastic Surgery
Footnotes
Acknowledgments
Not applicable.
Author Contributions (Credit Statement)
Conceptualization: [Sara Morel, Rawan El Abd].
Methodology: [Sara Morel, Rawan El Abd].
Literature Review: [Sara Morel, Rawan El Abd].
Writing Original Draft: [Sara Morel, Rawan El Abd].
Writing Review & Editing: [Sara Morel, Rawan El Abd, Youssef ElAbd, Dino Zammit, Sabrina Cugno].
Supervision: [Dino Zammit, Sabrina Cugno].
Declaration of Interest
None of the authors have conflict of interests.
Ethical Approval and Informed Consent
Not applicable.
Funding
Not applicable.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.