
Abstract
Introduction
The World Health Organization estimates 7.8 million women have breast cancer, making it the most prevalent cancer in the world. 1 In 2012, the Canadian Cancer System Performance Report reported that roughly 40% of breast cancer resections performed were mastectomies. 2 In 2014, Porter et al reported that mastectomies accounted for 39% of all breast cancer-related surgeries among patients with unilateral invasive breast cancer, highlighting their prominence as a treatment modality. 3
The increasing preference for enhanced aesthetic outcomes has led to popularization of conservative mastectomy combined with reshaping and reconstruction. A 2015 meta-analysis found that of 4663 patients undergoing mastectomy, 30% underwent nipple-sparing mastectomy (NSM) and 15% underwent skin-sparing mastectomy (SSM).4,5 In 2020, Wang et al reported that of 798 patients undergoing either NSM or SSM, 27.2% received NSM and 72.8% received SSM. 6 Meanwhile, rates of NSM have increased from 2.9% to 8.0% between 2010 and 2013, while prevalence rates of SSM remain unclear. 5
In some Canadian institutions, only 21% of patients who underwent mastectomy also received reconstruction of any type, with 14% receiving immediate breast reconstruction (IBR) and 8% delayed breast reconstruction (DBR). 7 A nationwide study from the United States conducted estimated that between 14%-40% of patients undergo reconstruction, resulting in an estimated 106 000 reconstructive surgeries in 2017.8,9 Another study by Yoon et al in 2018 indicated that of patients receiving breast reconstruction, 92% received IBR, and 8% received DBR, while by Kuhlefelt et al in 2023 observed 53% received IBR and 47% received DBR. 10
IBR has been shown to have improved self-reported patient satisfaction, body image, and quality of life. 11 It contributes positively to various aspects of recipient lives, such as physical, psychosocial, and sexual quality of life outcomes for recipients.11,12 Notably, patients receiving DBR exhibited better health-related quality of life outcomes (HRQoL) after 12 months, but recipients of IBR had better HRQoL after 24 months, with similar HRQoL outcomes among different IBR techniques. 13 Despite this, Kuhlefelt et al found that no difference in long-term follow-up on HRQoL, psychosocial well-being, and satisfaction with breast-related surgical outcomes when comparing IBR and DBR. 14
However, concerns over the adoption of IBR due to the associated risk of local recurrence (LR), denoting the reappearance of cancer in the breast, chest-wall, surgical scar, or overlying skin. 15 Joo et al, 2021 evaluated the pattern and location of LR, identifying the skin and subcutaneous tissue as the predominant sites of LR within the primary quadrant. 16 In 2009, Gerber et al observed that LR rate varies by types of mastectomy, with 10.4% for SSM and 11.7% for NSM (P = 0.974). 8 According van Mierlo et al (2013), the 5-year LR rate following SSM + IBR was 2.9% in 147 patients with invasive breast cancer. 17 Additionally, in 2021, Fujihara et al found an LR rate was 3.1% in a population that underwent implant-based breast reconstruction. 18 A systematic review by Bargon et al (2022) revealed comparable rates of LR between IBR and DBR groups, suggesting that oncological concern should not influence choices regarding reconstruction timings. 19
Furthermore, McCarthy et al reported comparable incidence of locoregional recurrence for patients undergoing immediate, tissue expander reconstruction compared to those without reconstruction. 20 Similarly, Huang et al observed no differences in LR incidence between patients with or without TRAM flap reconstruction. 21 A broader systematic review of LR rates post-mastectomy, with or without reconstruction, has not been conducted since Gieni et al (2012) found comparable rates of LR for patients with and without IBR; however, this review includes papers from the 1990s, which do not reflect recent surgical advances and guidelines.22,23
Multiple risk factors for LR have been reported, which can be broadly classified into patient, treatment, and tumor factors. Patient-related factors include elevated body mass index, smoking, steroid use, and age.18,22,24 Treatment factors linked to increased LR risk include rough-textured implants, raise concerns regarding both implant-associated anaplastic large cell lymphoma and LR. 25 Preservation of the skin overlying the initial tumor and the needle track site of a core needle biopsy have been linked with LR. 18 Tumor-related factors such as HER2 positivity, estrogen receptor (ER) negativity, and progesterone receptor (PR) negativity, tumor size, grade, location, and advanced disease stage heighten the odds of recurrence.18,26–28
Considering the lack of clinical consensus surrounding this debated topic, which holds significant implications for clinical decision-making, this systematic review and meta-analysis aim to investigate the impact of IBR on LR incidence and examine patient, tumor, and reconstructive factors associated with LR. This review will also address the oncological safety of IBR in the context of its benefits.
Methods
This systematic review and meta-analysis adhere to the guidelines recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 29 The protocol was registered on Open Science Framework and published in Protocol Exchange. 30
Search Strategy
A literature search was performed on MEDLINE (Ovid), Embase (Ovid), Web of Science, and European PubMed Central for observational studies and conference abstracts. The search terms utilized terms related to “breast cancer,” “mammoplasty,” and “local recurrence.” A detailed search strategy is outlined in the Supplementary Table 1.
Screening Strategy
Inclusion criteria were records written in English, published between 2000 and 2020, from any geographical location, reporting observational studies (cohort, case-control, or cross-sectional studies). Only studies on the adult population (≥18 years) of any gender/sex with a minimum follow-up of 1 year were included. Eligible studies specifically focused on patients with early-stage breast cancer (stage I or II) who underwent mastectomy, comparing those who received IBR (Mast + IBR) to those who underwent mastectomy without reconstruction (Mast − IBR) and reported LR for both groups. Studies were excluded if they focused on partial or completion mastectomy.
A two-stage screening strategy was employed. Two reviewers independently screened the titles and abstracts of all potentially relevant records based on the inclusion and exclusion criteria. Disagreements were resolved through discussion, and if unresolved, a third reviewer made the final decision. Subsequently, two reviewers screened the full texts of potentially relevant records, following the same resolution process for any disagreements.
Data Extraction
For each included study, data were extracted on study factors, patient factors, patient factors, reconstructive factors, and outcome factors. Data was extracted independently by the reviewers. Any discrepancies were recorded and discussed until a resolution is reached. If a resolution was not reached, a third reviewer made the final decision.
Critical Appraisal
For each record marked as Included, two reviewers critically appraised the articles using the Johanna Briggs Institute (JBI) critical appraisal tool for cohort studies. 31 For each question on the critical appraisal tool, the reviewers responded with Yes, No, Unclear, or Not Applicable. Two reviewers independently reviewed the records. If there was any disagreement, the reviewers discussed until a resolution was reached. If the two reviewers were unable to agree on a resolution, a third reviewer made the final decision.
Data Analysis
To examine the comparative rates of LR between the groups, the odds ratios (ORs) and their 95% confidence intervals (CIs) were calculated for each included study. The pooled overall OR was calculated by a random-effect model. To identify univariate associations of selected factors to LR, an average of each selected factor in each study was calculated. Selected factors included age, follow-up time, cancer stage, post-mastectomy breast cancer radiation therapy (PMRT) status, ER status, PR status, and HER2 status. Random-effects meta-regression was used to examine the association between LR and IBR. Given the small number of studies (n = 10), the final meta-regression analysis was adjusted for age and follow-up time. Meta-regression analysis was completed with the R version 4.3.2 with statistical package rma.
Heterogeneity between studies was assessed using I2 statistic and a P-value. A funnel plot was used to visually investigate the heterogeneity. An Egger's test was performed to assess asymmetry in the funnel plot. Then, the heterogeneity was assessed using a sensitivity analysis to estimate the impact of large population studies on the pooled OR. Plots were created using statistical package ggplot2.
Grading Study Quality
Study quality was graded using the Grading of Recommendations Assessment, Development, and Evaluation framework (GRADE). 32 Two reviewers independently performed the grading. If there was any disagreement, the reviewers discussed until a resolution was reached. If the two reviewers were unable to agree on a resolution, a third reviewer made the final decision.
Results
Literature Review
The literature search yielded 1136 records from MEDLINE (Ovid), 701 from Embase (Ovid), 81 from Web of Science, and none from expert networks, totaling 1918 records. A total of 443 duplicates records were removed, leaving 1475 unique records. During the title and abstract screening phase, 1434 records were excluded, leaving 41 records for full-text screening. Of these, 31 records were excluded during the full-text screening phase, resulting in 10 studies for inclusion, as shown in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram in Figure 1.
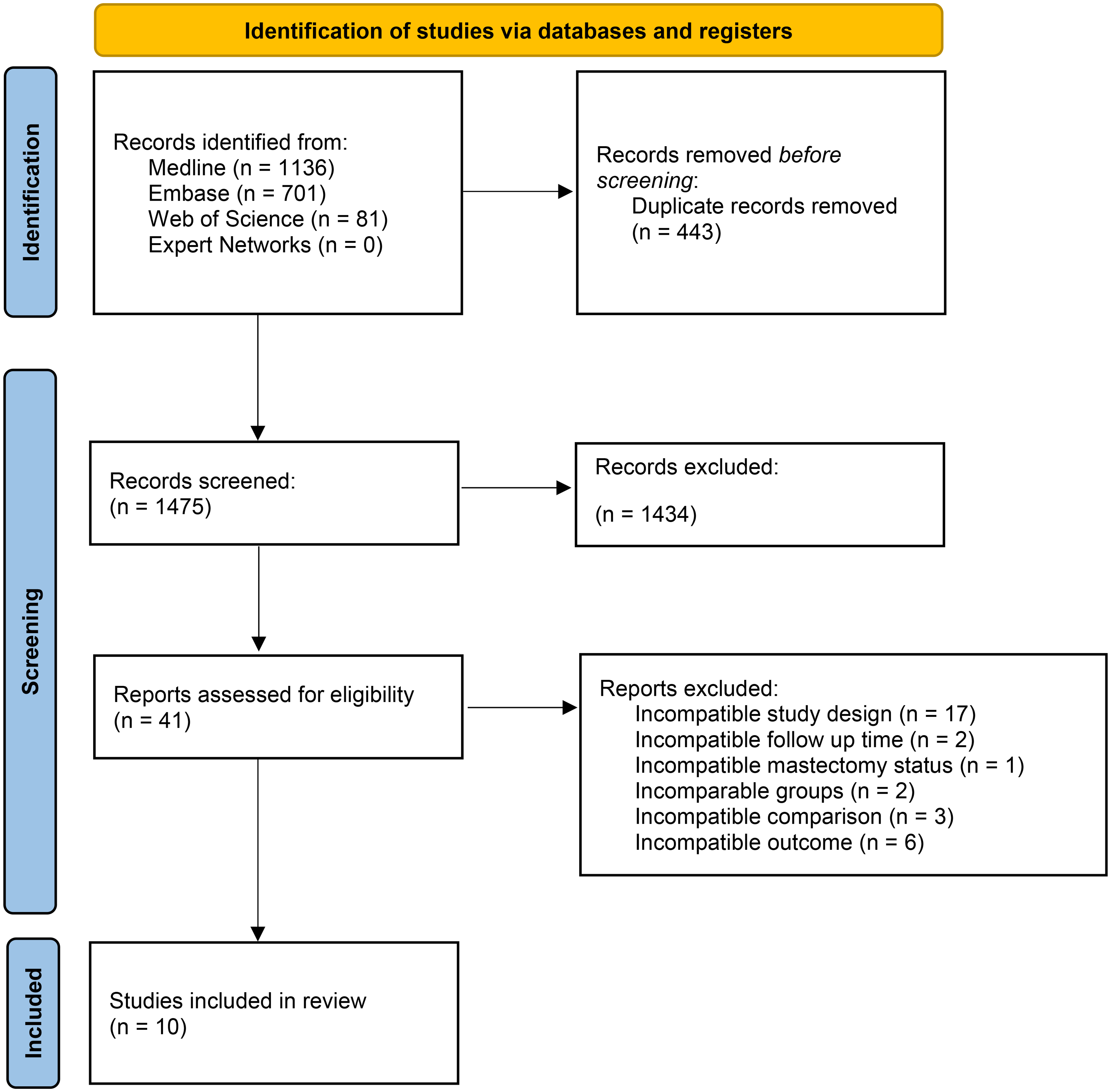
PRISMA flow diagram outling the study selection process for the sytematic review. Adapted from Page et al.29 PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Included Studies
Ten studies were included in this systematic review, amounting to 15 173 patients (3478 in Mast + IBR and 11 695 in Mast − IBR). Study sizes ranged from 191 to 6028 participants (median 623). Follow-up time ranged from 40 to 144 months, with a median of 70 months. Among the 10 studies, four were based in Korea, two from Sweden, as well as one each in China, Taiwan, the United States, and the United Kingdom. Characteristics of all included studies are detailed in Supplementary Table 2.
Critical Appraisal of Included Studies
Using the JBI checklist for cohort studies, 10 studies were included. For several included studies, we identified non-comparable population, which is consistent with our expectations due to observed variations in patient characteristics; notably, younger women are more likely to receive IBR. 33 Detailed results of the critical appraisal are presented in Supplementary Figure 1.
Comparative Analysis
Participants in the Mast + IBR group were younger with a median age of 46.5 years (interquartile range, [IQR] 42.7-48.0) than the patients in the Mast − IBR group with a median age of 49.6 (IQR 47.9-50.6). Only younger age was correlated with higher IBR rates (P < 0.05). The mean follow-up time for the Mast + IBR group was 72.9 months, whereas the mean for Mast − IBR group was 73.3 months. Of the 10 included studies, eight studies provided subgroup data on cancer stage (stage I-III), representing 12 886 patients. Of these, 3517 (27.29%) were in stage I, 6521 (50.61%) were in stage II, and 2848 (22.10%) were in stage III. Summary of study characteristics is outlined in Supplementary Table 3.
The LR rate per 1000, defined as the proportion of patients with LR in each group within a study multiplied by 1000, ranged from 7.8 to 88.8 in the IBR group, and 7.1 to 90 in the no IBR group. Median recurrence rate per 1000 in Mast + IBR group was 26.3 and 19.4 for the Mast − IBR group (Table 1).
Summary of findings table for local recurrence outcomes in patients with and without immediate breast reconstruction (IBR) after mastectomy.
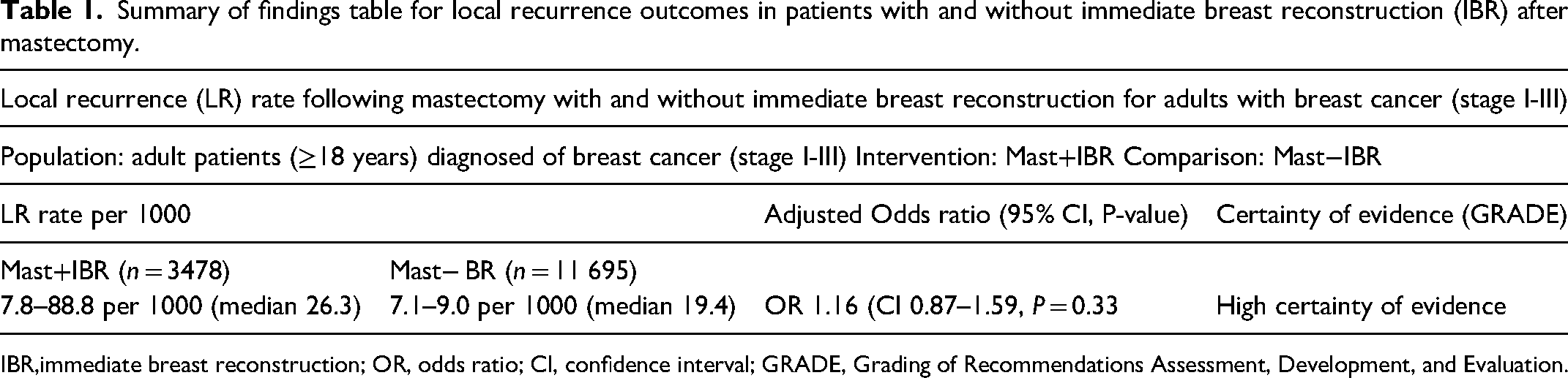
immediate breast reconstruction; OR, odds ratio; CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development, and Evaluation.
Univariate Meta-Regression
The univariate meta-regression did not demonstrate an association between LR and pre-selected factors, including age, follow-up time, cancer stage, ER status, PR status, and HER2 status (P > 0.05) (Table 2). This is also true of PMRT, with no observed increased odds of association to LR (OR: 0.99, CI 0.99-1.00, P = 0.033).
Univariate meta-regression examining the effect of study-level covariates on odds of local recurrence.
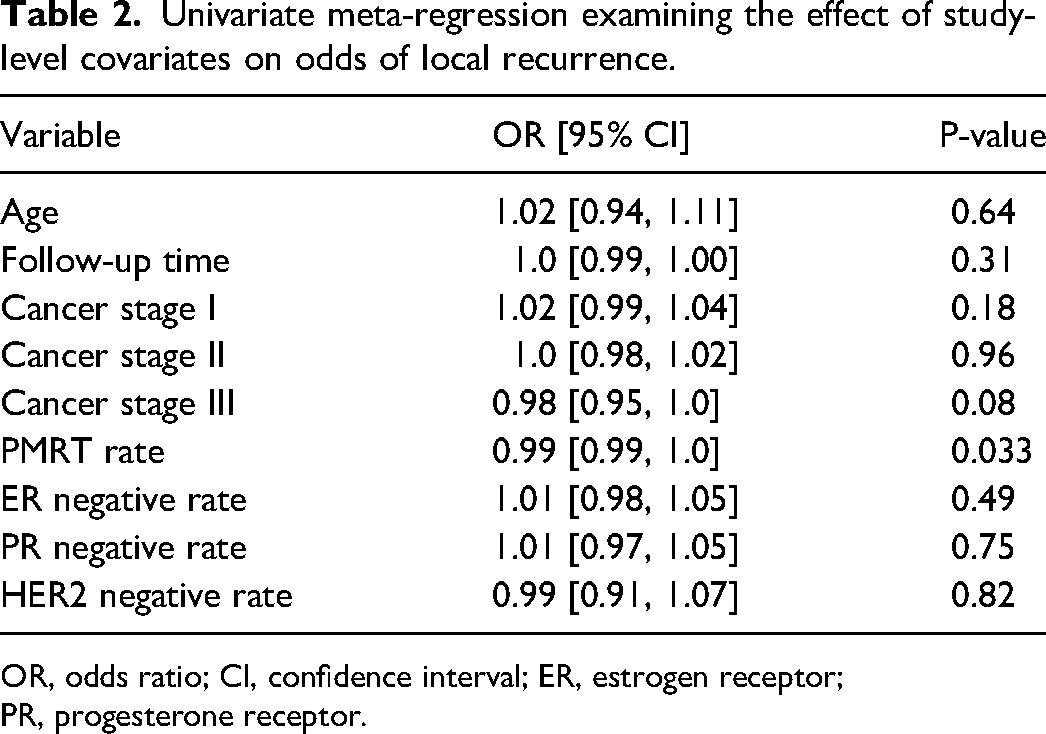
OR, odds ratio; CI, confidence interval; ER, estrogen receptor; PR, progesterone receptor.
Multivariate Meta-Regression
The unadjusted meta-analysis suggests comparable rates of LR with or without IBR (OR 1.27, CI 0.98-1.65, P = 0.067). Effect sizes of included studies are visualized in the Forrest Plot (Figure 2). When adjusted for age and follow-up time, there is no observed increased in odds of LR (OR 1.17, CI 0.86-1.59, P = 0.33). Overall, 111 (3.2%) participants in Mast + IBR experienced LR, compared to 245 (2.1%) participants in Mast − IBR experienced LR (Figure 2).
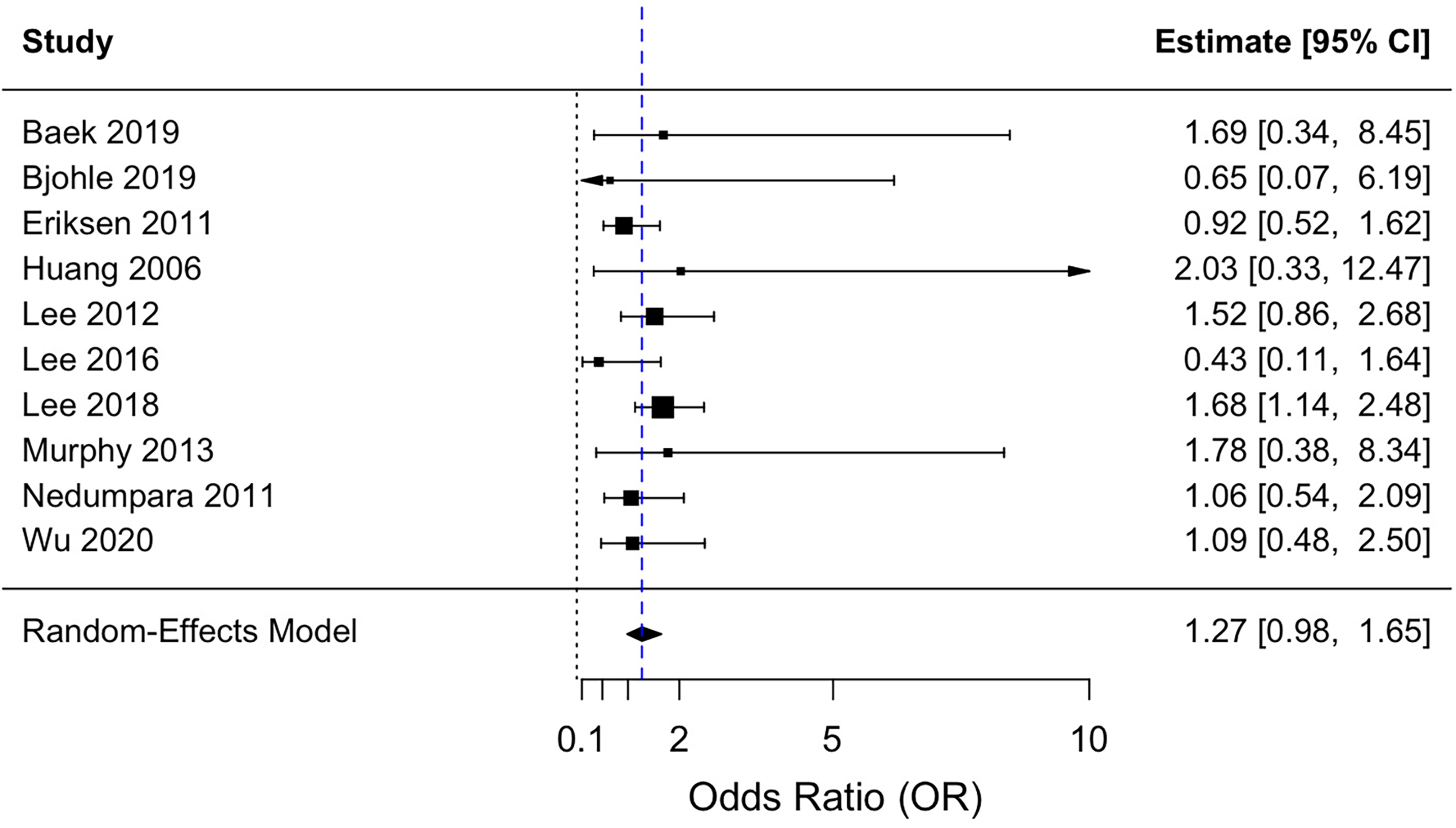
Forest plot comparing local recurrence rates in patients with and without immediate breast reconstruction. Error bars indicate 95% confidence intervals.
Sensitivity Analysis
The unadjusted sensitivity analysis revealed that the ORs were robust to unmeasured confounding factors on the causal relationship of the study (Supplementary Table 4). When unadjusted, all crude ORs are statistically significant (P < 0.05), except for Lee 2012 and Lee 2018 (P > 0.05) with the largest sample sizes.34,35
Heterogeneity Assessments
The I2 statistic (I2 = 7.37, P = 0.60) indicates low heterogeneity in the unadjusted meta-analysis, suggesting that variation arises from random sampling error rather than inherent differences among the studies. The funnel plot and Egger's test (t = −1.00, P = 0.34) are concordant, indicating a symmetric distribution around the log(pooled OR) with minor dispersion, indicating robustness to significant publication bias (Figure 3).
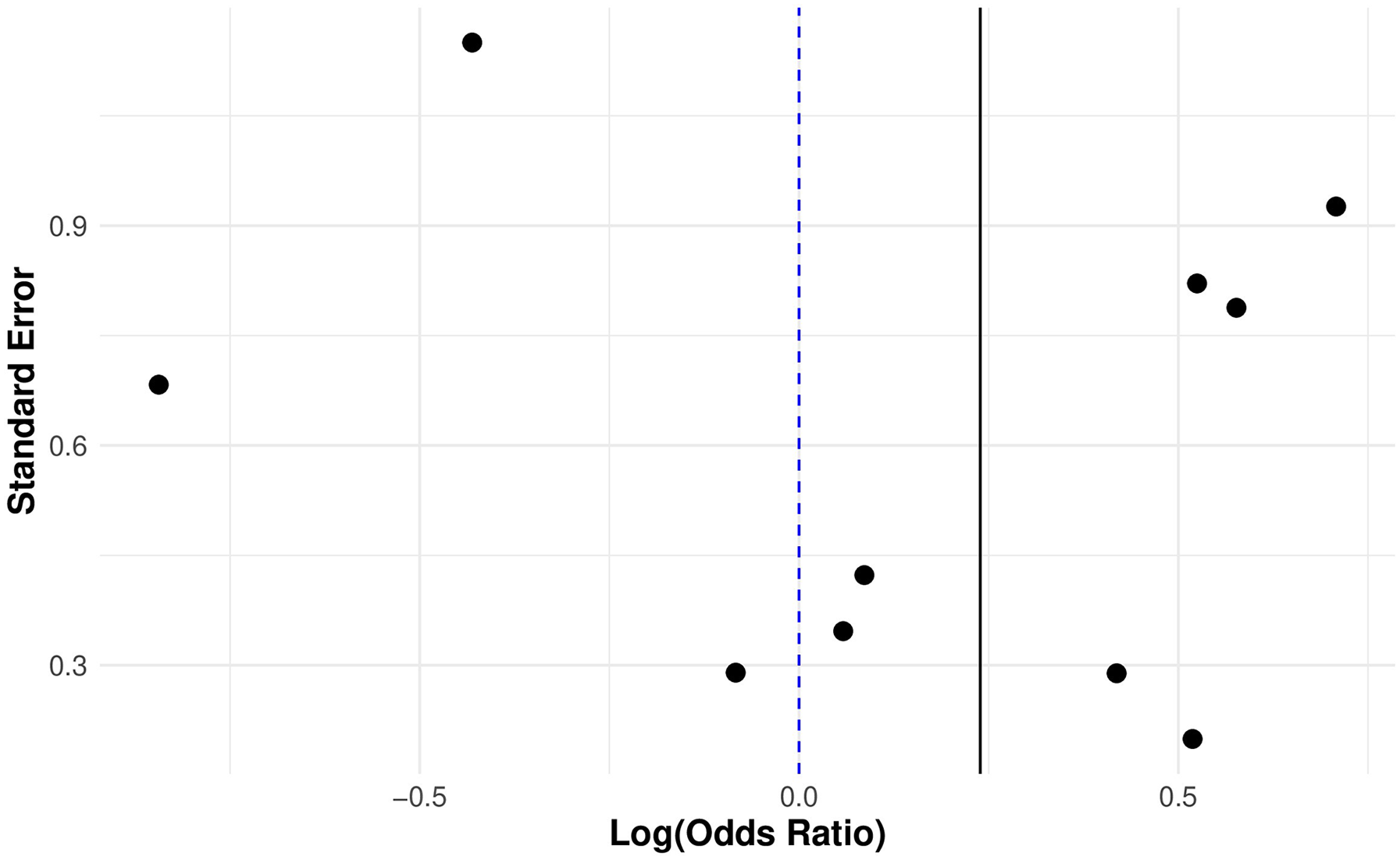
Funnel plot of included studies assessing local recurrence in patients with and without immiedate breast reconstruction.
Discussion
Discussion of Findings
This systematic review and meta-analysis indicate that post-mastectomy IBR does not increase the risk of LR compared to mastectomy alone, after adjusting for age and follow-up time since age is a well-documented confounding factor associated with IBR. 24 Studies with a median follow-up time of under 1 year were excluded, given that LR is clinically detectable after this period, thus minimizing the association between follow-up time and LR. 36
Moreover, this review indicates that younger patients are more likely to receive IBR compared to older counterparts; this agrees with the literature, which demonstrated that surgeons are more likely to discuss IBR with patients that are educated, younger, and with large tumors. 33 While other reasons also underscore this phenomenon, including patient choice, physician bias, and/or clinical contraindications, research remains inconclusive. 33 Notably, older patients may prioritize minimizing disruptions to daily life more than younger patients, which may in part explain this bias. 33
Our univariate analysis found no association between follow-up time, age of diagnosis, cancer stage, ER status, PR status, HER2 status, and PMRT with LR. This result may appear unexpected as it is well established that HER2 positive status increases the risk of LR while PMRT does not increase LR risk. This discrepancy may result from underreported statuses in the included studies and the small sample size.37,38 Specifically, of the 10 included studies, five reported ER and PR statuses, four reported HER2, and eight reported PMRT.
Clinical Implications
This systematic review indicates that patients can undergo IBR without concern for LR. This result aligns with a systematic review by Bargon et al that indicated comparable LR outcomes between IBR and DBR. 39 Our review updates Gieni et al (2012) by focusing on studies from 2000 to 2020, thus reflecting more recent findings while avoiding COVID-19 impacts. 23 Unlike Gieni et al, we adjusted for age and follow-up time as confounders; however, Gieni's unadjusted and our adjusted and unadjusted meta-analyses all yielded non-significant pooled ORs. Additionally, Gieni et al included a higher proportion of studies from the United States, which may have influenced outcomes. Both reviews analyzed 10 cohort studies, but only Gieni's had sufficient data for subgroup analysis.
Recent trends in mastectomy surgery have focused on viability of the skin flaps by preserving more residual tissue for reconstruction, as reported by a systematic review by Lv et al in 2023. 40 A subgroup analysis performed by Woitek et al, 2018 indicated that rates of residual tissue in NSM were more than double that of SSM (50% vs 13%, P = 0.003). 41
Thicker flaps, especially those over 5-7 mm, have elevated rates of residual breast tissue in various quadrants of the breast, compared to those under 5 mm thickness. 40 Deutschmann et al 2023 found that the ratio of residual breast tissue to preoperative fibroglandular tissue was found to produce higher rates of LR. 42 As any residual breast tissue increases the risk of recurrence, this poses the potential for an increase reporting of LR in future years. Given this recent trend for thicker flaps and delayed potential increase in LR, there is a need for periodic re-review of this topic every 10-15 years.
Limitations
Our systematic review is limited by the nature of the 10 included studies. Despite the pooled OR having a narrow CI, four included studies exhibited wide CIs. Of these, while Baek 2019, Bjohle 2019, and Huang 2006 had sample sizes under 600, Murphy 2003 had over 1200, yet some smaller studies have narrower CIs, likely due to methodological differences and event rate variability.10,43–46 The small number of studies limited the statistical power of our meta-regression analysis, which may explain why key factors such as cancer stage, ER status, PR status, and HER2 status did not yield statistically significant results. Additionally, with only 10 studies, our ability to conduct subgroup analyses and assess potential effect modifiers was restricted, which may limit the generalizability of our findings.
Despite the low I2 and insignificant Egger's test, indicating minimal statistical heterogeneity, sources of bias remain. The overrepresentation of high-income Asian countries in the included studies may introduce geographic bias, potentially limiting the generalizability of our findings to other populations. Additionally, publication bias in observational studies may favor significant LR outcomes, while survivor bias could affect populations with high loss to follow-up rates. Clinician bias may influence which patients are offered IBR, leading to variable treatment selection based on factors like age, health, or other characteristics. 22 These factors, along with differences in follow-up procedures, may introduce unmeasured heterogeneity that our meta-regression could not fully account for, limiting our ability to further explore effect modifiers.
Lastly, our review's focus on LR among early-stage breast cancer patients with adequate medical access limits its generalizability, potentially underestimating broader oncological risks and failing to reflect the increasing diversity of patient populations.
Conclusion
This systematic review and meta-analysis evaluated the long-term incidence of LR in 15 173 patients with breast cancer undergoing mastectomy with or without IBR. After a mean follow-up of 72.9 months for the Mast + IBR group and 73.3 months for the Mast − IBR group, LR occurred in 3.2% and 2.1% of patients, respectively. The OR was 1.17, (CI 0.86-1.59, P = 0.33), when adjusted for age and follow-up time. These findings indicate the oncological safety of post-mastectomy IBR, allowing patients to benefit from improved esthetics and quality of life without increased LR risk. Further research on specific mastectomy and reconstruction types is needed to explore factors influencing the oncological safety of post-mastectomy breast reconstruction.
Supplemental Material
sj-docx-1-psg-10.1177_22925503251363108 - Supplemental material for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-psg-10.1177_22925503251363108 for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis by Melissa Chao, Kellan Woo, David Long, Dana Toameh and Kathryn V. Isaac in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503251363108 - Supplemental material for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-psg-10.1177_22925503251363108 for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis by Melissa Chao, Kellan Woo, David Long, Dana Toameh and Kathryn V. Isaac in Plastic Surgery
Supplemental Material
sj-xlsx-3-psg-10.1177_22925503251363108 - Supplemental material for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis
Supplemental material, sj-xlsx-3-psg-10.1177_22925503251363108 for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis by Melissa Chao, Kellan Woo, David Long, Dana Toameh and Kathryn V. Isaac in Plastic Surgery
Supplemental Material
sj-docx-4-psg-10.1177_22925503251363108 - Supplemental material for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-psg-10.1177_22925503251363108 for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis by Melissa Chao, Kellan Woo, David Long, Dana Toameh and Kathryn V. Isaac in Plastic Surgery
Supplemental Material
sj-docx-5-psg-10.1177_22925503251363108 - Supplemental material for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis
Supplemental material, sj-docx-5-psg-10.1177_22925503251363108 for Breast Cancer Local Recurrence in Patients With and Without Post-Mastectomy Immediate Breast Reconstruction: Systematic Review and Meta-Analysis by Melissa Chao, Kellan Woo, David Long, Dana Toameh and Kathryn V. Isaac in Plastic Surgery
Footnotes
Acknowledgements
We would like to acknowledge Ursula Ellis, a librarian at the University of British Columbia, for her guidance in developing the search terms. As well, we would like to acknowledge Meijiao Guan, a statistician at the Centre for Health Evaluation and Outcome Sciences, for her work in designing the meta-analysis. Finally, we acknowledge Emma Nicholson and Raveena Gowda for their work as research coordinators at the University of British Columbia.
Dr Kathryn Isaac is holder of the Dr Patricia Clugston Chair in Breast Reconstruction Surgery at the University of British Columbia and would like to acknowledge the support of Vancouver General Hospital & University of British Columbia Hospital Foundation's donors and partners who made this Chair possible.
Author Contributions
MC was involved in concept generation, protocol preparation, literature review, record screening, data extraction, critical appraisal, data analysis, grading the review, figure preparation, and writing manuscript. KW was involved in data extraction, critical appraisal, data analysis, grading the review, and assisted with manuscript writing. DL was involved in concept generation, protocol preparation, literature review, screening, assisted with manuscript writing (Introduction only), and manuscript review. DT was involved in literature review, screening, and manuscript review. KVI was involved in concept generation and manuscript review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statements
Ethics not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Previous Study Related Presentations
Poster abstract presented in Ninth Annual Women's health Research Symposium, 2024 and Canadian Society of Plastic Surgeons Annual Meeting, 2024.
Study Registration Number,if Applicable
Protocol registered on Open Science Framework and published in Protocol Exchange (DOI: 10.21203/rs.3.pex-2529/v1).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.