
Abstract
Introduction
Flexor tendon repair is one of the most common pathologies of hand injury. For ideal outcomes, primary flexor tendon repair is to be performed in a timely manner after the injury 1 and, traditionally, in the controlled setting of an operating room (OR). Major complications observed following this surgery are rupture, infection, and adhesions. 2
Wide-awake local anesthesia no tourniquet (WALANT) surgery has demonstrated its value and popularity in hand surgery, 3 allowing surgeons to safely operate patients in different settings, without an anesthesia team, and sometimes outside of the main OR. Many cost-analysis studies demonstrate the advantage of this practice in hand surgery.4,5 Flexor tendon repair using WALANT has previously been described, 6 with good outcomes and complications profiles.7–9
In the wake of the COVID-19 pandemic, OR access became more limited, 10 prompting plastic surgeons at our university to operate flexor tendons in clinic-based procedure rooms (PRs). 11 This practice is not well described in the literature, and therefore the complication rates in such a setting are not known. 12
We conducted a retrospective study comparing 2 different surgical settings within a single medical center to answer the following guiding question: in patients undergoing primary flexor tendon repair, does the PR setting put patients at higher risk of complications when compared to patients operated in an OR? We hypothesize that the complication rate would not be different between the 2 settings. The goal of our team was to gain a better understanding of the impact of operative setting on complications in hand flexor tendon repair.
Methods
Patient Sample
This retrospective study done at a single-center university hospital was approved by our institutional review board. Inclusion criteria included patients who presented with a hand flexor tendon laceration between January 1st, 2018 and February 28th, 2023. Lesions of the following structures were considered: flexor pollicis longus (FPL), flexor digitorum profundus (FDP), flexor digitorum superficialis (FDS), palmaris longus (PL), flexor carpi radialis (FCR), and flexor carpi ulnaris (FCU). Patients with concomitant major hand trauma (amputation of a digit, vascular trauma, unstable soft tissue coverage, or gross contamination) and with less than 6 months of follow up were excluded. Patients were identified via billing codes for flexor tendon repair.
Data collection was realized through retrospective chart review. Patient characteristics variables included age, gender, tobacco use, and diabetes. Trauma details collected included zone of flexor tendon injury (I through V), tendon affected and repaired, type of anesthesia, time between diagnosis and surgery, any concomitant lesions (digital nerve or artery, metacarpal or phalangeal fracture), and operative setting (OR vs outpatient clinic). Procedural type of anesthesia was described as well, namely, general, regional, or WALANT. Study groups were formed based on operative setting.
All postoperative visit notes were examined to evaluate the presence of primary and secondary outcomes. The primary outcome was defined as presence of postoperative tendon rupture, which was identified by mention of tendon rupture at follow up and/or presence of secondary tendon repair surgery. Secondary outcomes included presence of infection (surgical site infection, abscess, or flexor tenosynovitis), presence of adhesions, need to reoperate (primary flexor tendon repair, secondary tendon reconstruction, or tenolysis) and, more broadly, presence of any complication. Antibiotic prescription at follow up was considered a proxy for infectious complication. Mention of adhesions in follow-up notes, or if flexor tenolysis was offered to a patient, were considered proxies for adhesions. All files were examined up to 1 year postinjury.
Postoperative care was done in collaboration with our occupational therapy team, with an early active motion protocol given to all patients. There was no distinction in the rehabilitation offered and received by patients on the basis of whether they were operated in a clinic-based PR or in OR.
Statistical Analysis
For comparison of study groups, chi-square (X2) and Mann–Whitney U tests were done for categorical variables and continuous variables, respectively. A logistic regression model was then employed to determine the association between complication rate and surgical setting. Results are reported with ORs and 95% confidence intervals. A P-value of less than .05 was considered significant.
Results
After chart review, a total of 174 patients were included in the study, with 93 patients in the PR group and 81 patients in the main OR group. All demographic data collected can be found in Table 1. The study population was comprised of 137 male patients and 37 female patients. The median age was 41 years.
Demographic Data.
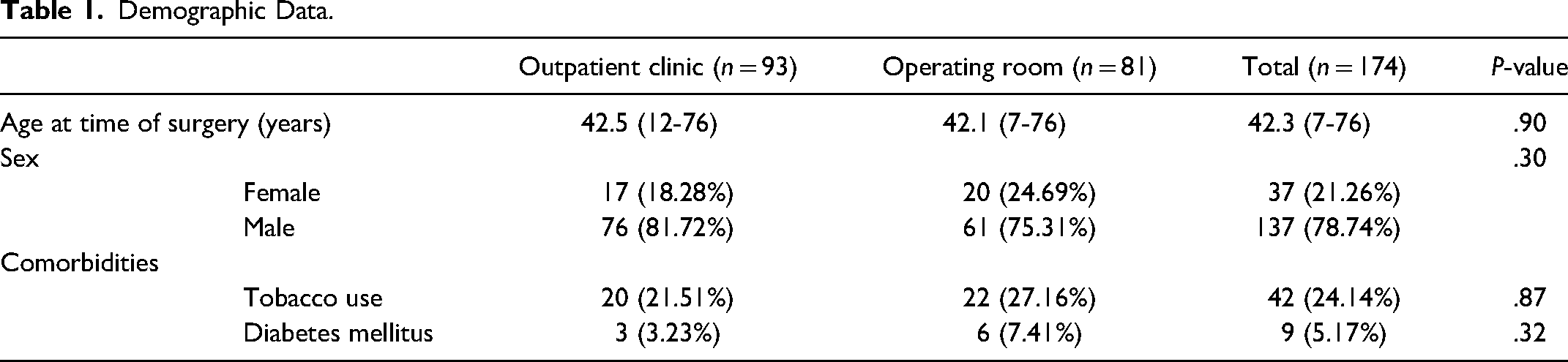
Table 2 summarizes the surgical characteristics of the 2 study groups. As for the anatomical distribution of the injuries, 58 (33.3%) patients had a lesion in flexor zone I, 73 (42.0%) in zone II, 13 (7.5%) in zone III, 2 (1.1%) in zone IV, and 28 (16.1%) in zone V. A total of 324 flexor tendon repairs were performed among the 174 patients (159 FDP, 91 FDS, 31 FPL, 16 FCR, 16 FCU, and 10 PL).
Surgical Data.
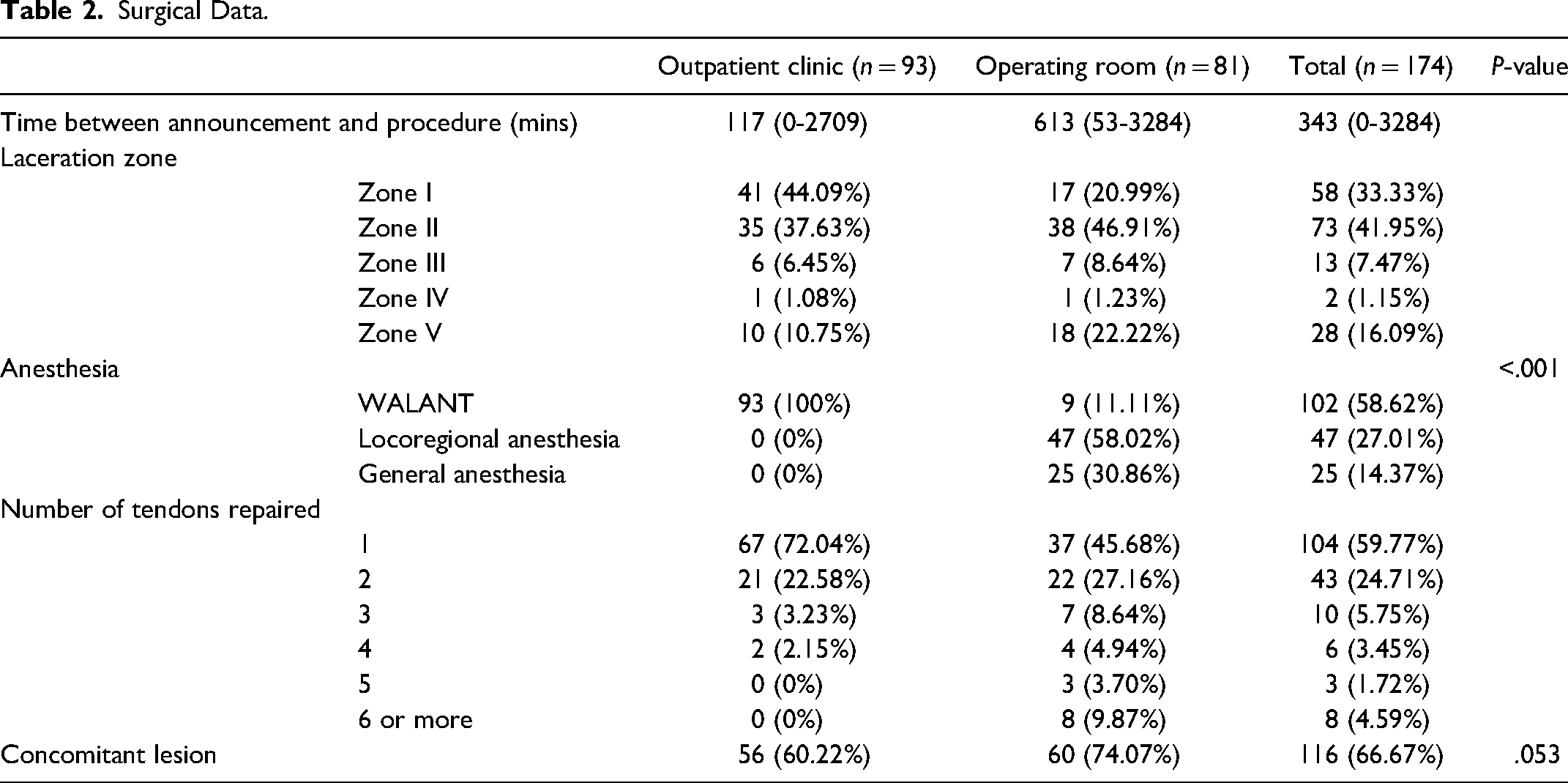
The 2 groups were largely similar across the studied variables. By design, there was a statistically significant difference between the type of anesthesia performed, with 93 (100%) of patients operated in clinic PRs undergoing a WALANT technique, in contrast to 9 (11.1%) undergoing WALANT in the OR (P < .0001). Although not statistically significant, a greater proportion of patients operated in an OR context had concomitant lesions (60 patients, 74.1%), as compared to 56 (60.2%) patients in the clinic-based PR group (P = .053).
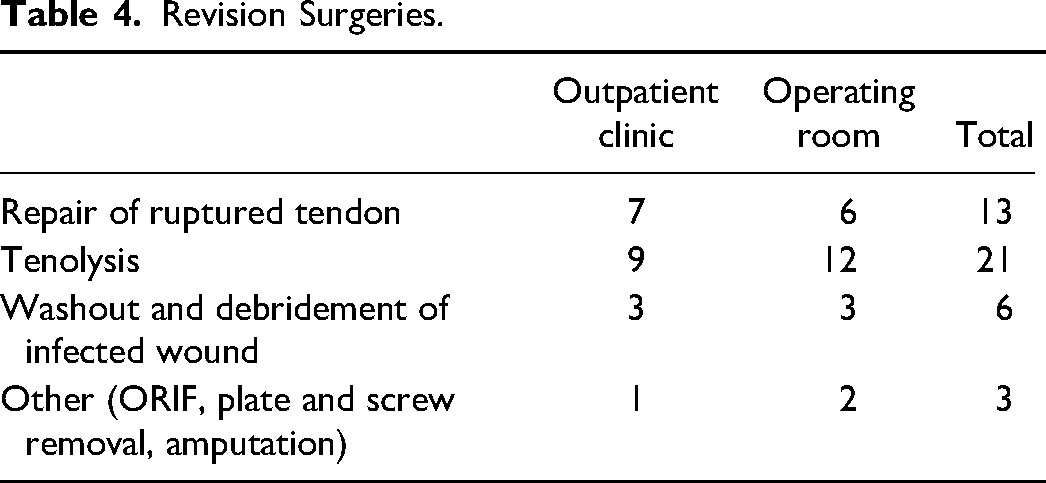
No association was observed between surgical setting and presence of postoperative tendon rupture, infectious complications, adhesions and need for a second intervention (see Table 3). A total of 5 ruptures (6.2%) occurred in the OR group and 6 in the PR group (6.5%) (OR = 1.05 [0.30-3.78]; P = .94). Infectious complications were noted in 6 cases (7.4%) in the OR group and 6 cases (6.5%) in the PR group (OR = 0.86 [0.26-2.86]; P = .800). The presence of adhesions in the postoperative follow-up period was seen in 19 (23.5%) cases in the OR group and 14 cases (15.1%) in the PR group (OR = 0.58 [0.26-1.2], P = .160). 19 patients (23.5%) in the OR group required a second intervention, in comparison with 15 patients (15.0%) in the PR group (OR = 0.064 [0.30-1.30]; P = .24) (Figure 1). Table 4 summarizes the cases needing reintervention.
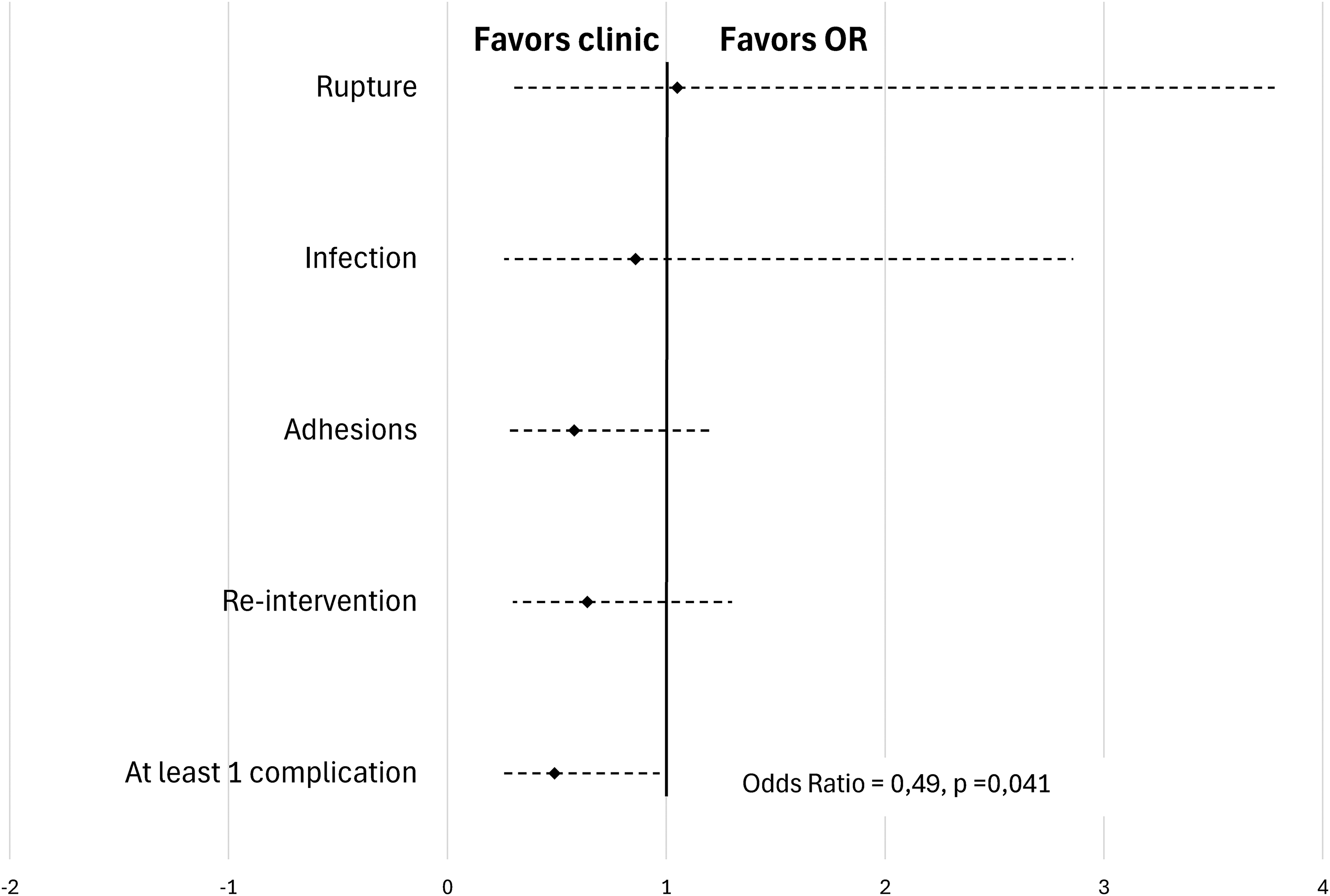
Primary flexor tendon repair rate of complications in single center study population.
Complications*.
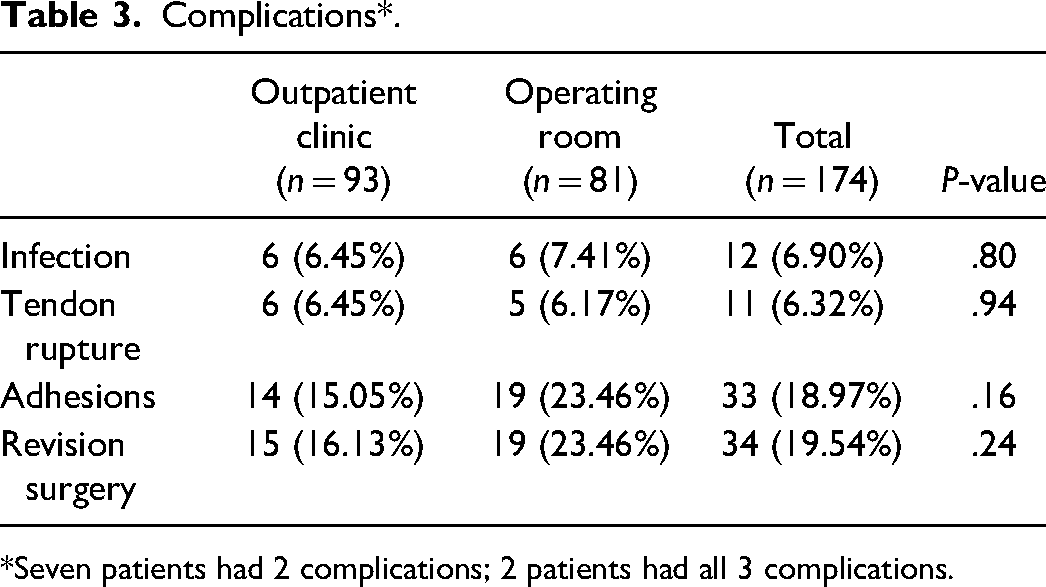
*Seven patients had 2 complications; 2 patients had all 3 complications.
Revision Surgeries.
In combining the complications (rupture, infection, and adhesions), being operated in a clinic-based PR reduces the chance of complicating by 51% in a statistically significant fashion (OR = 0.49 [0.24-0.97]; P = .041). Reintervention was not included in this calculation since it represents more of a proxy for a complication than a true complication in and of itself.
A subgroup analysis was then performed to specifically evaluate patients with injury to one finger alone in the absence of any devascularization injury. No association was observed between surgical setting and presence of rupture (OR = 0.32 [0.06-1.55]; P = .154), infection (OR = 0.55 [0.14-2.37]; P = .401), adhesion (OR = 0.69 [0.24-2.04]; P = .483) or need for reintervention (OR = 0.69 [0.24-2.04]; P = .483). In evaluating the presence of at least one complication (rupture, infection, and adhesions), the fact of being operating in an outpatient clinic PR versus OR lead to a statistically significant reduction in the chances of observing a complication by 61% (OR = 0.39 [0.16-0.96]; P = .039) (Figure 2).
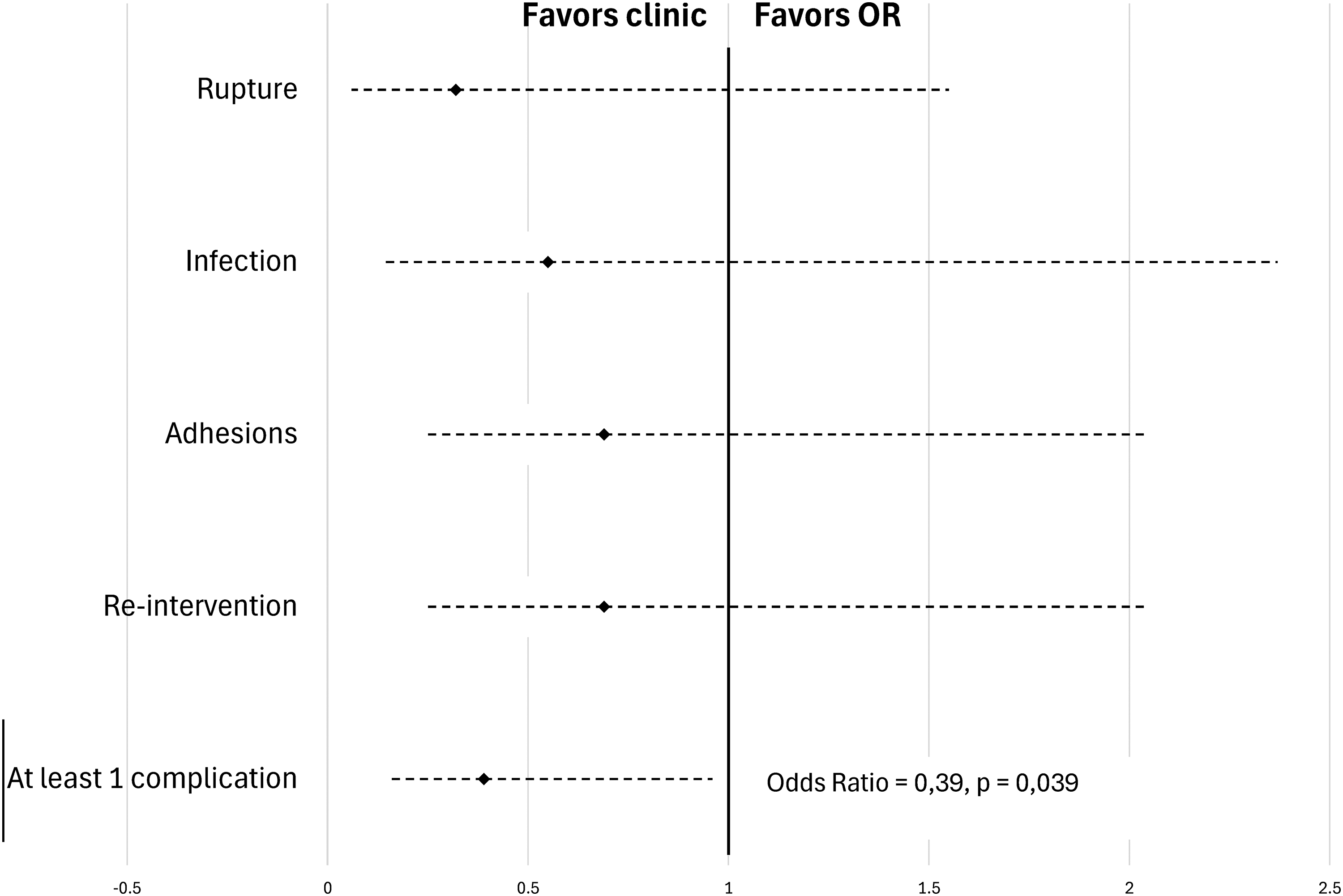
Rate of complications in single-digit subanalysis of flexor tendon repair.
Table 5 summarizes subgroup analysis by zone of injury. The only statistically significant difference was in zone II, where the PR setting was associated with a 59% reduction in the chance of observing a complication (P = .041), and less reintervention was observed as well (32.4% OR vs 11.8% PR; P = .049).
Injury Zone Comparison**.
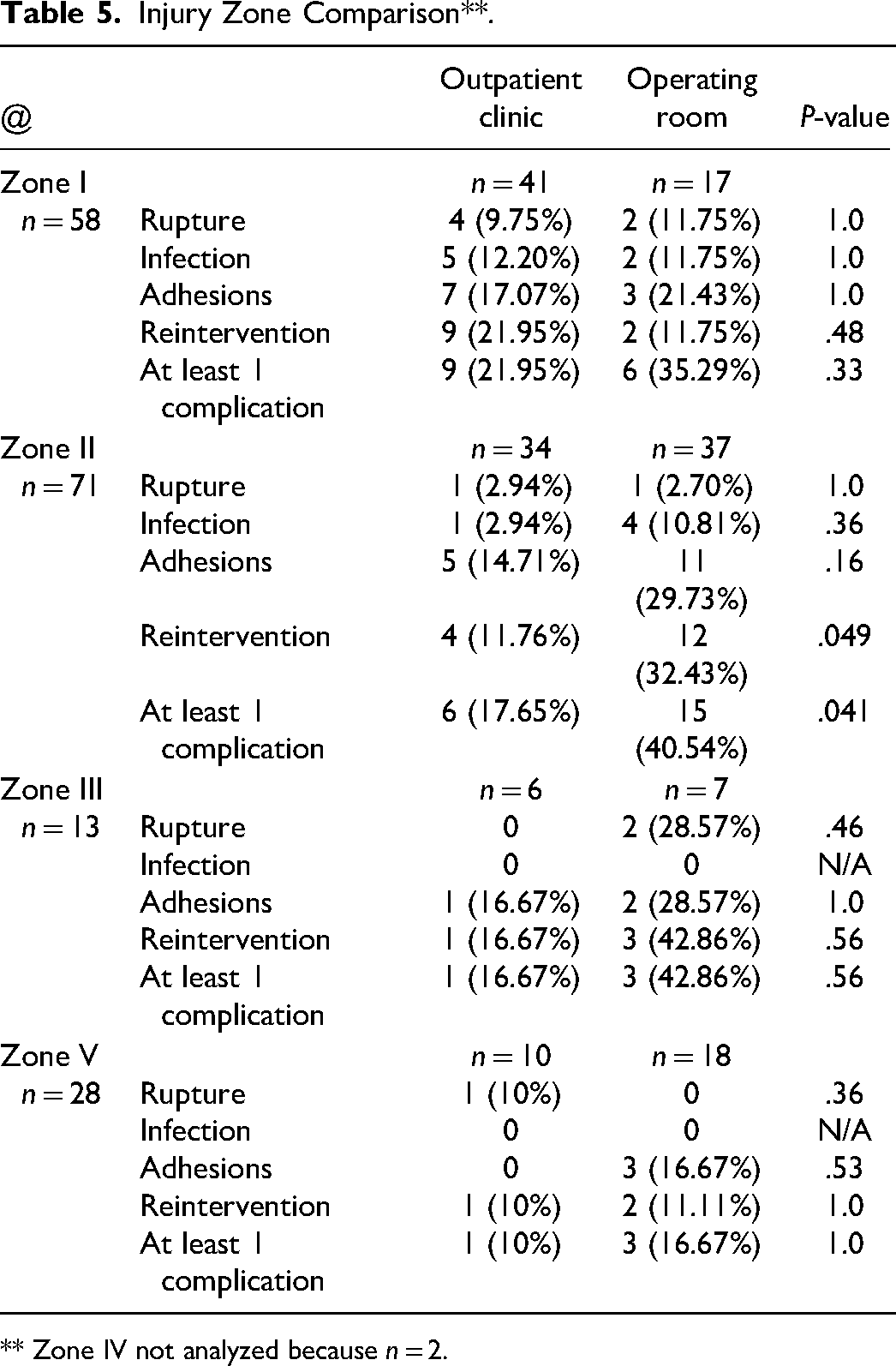
** Zone IV not analyzed because n = 2.
In the OR group, 25 of the 81 patients waited for more than 12 h for their surgery. Those operated in clinic-based PRs were not subjected to operative waiting times.
Discussion
The primary goal of this study was to evaluate whether performing primary flexor tendon repair in a PR puts patients at a higher risk of complications compared to patients operated in an OR. Our analysis found that the surgical setting of clinic-based PRs did not augment complication rates as compared to traditional main ORs.
Canadian plastic surgeon Dr Don Lalonde introduced and popularized the concept of WALANT for hand surgery.13,14 Numerous subsequent studies have testified to the efficacy and safety of WALANT, which is the injection of a local anesthetic agent, lidocaine, ensuring optimal pain control, with the use of epinephrine, a hemostatic agent, permitting good visualization during surgery and removing the need for a tourniquet. 15 Seeing as the WALANT technique is what allows for flexor tendon repairs to the performed in settings outside of a traditional OR, our investigation contributes to the existing body of the literature describing WALANT specifically for flexor tendon repair.16,17 As noted in similar studies, the advantages of WALANT in the setting of primary flexor tendon repair include the ability to evaluate the repair intraoperatively, for factors such as gliding and gapping. 18
While other papers stratified their study groups based on type of anesthesia,19–21 our study uses operative setting as our independent variable. In fact, 9 of the 81 cases performed in the operative room were done with WALANT as the anesthetic technique. Our findings therefore go a step further and demonstrate that the PR setting has advantages in and of itself. For one, performing flexor tendon repair in a setting outside of the OR also allows for a more judicious use of resources, including a considerable reduction of cost to the healthcare system, encompassing which include costs associated to the operating theater, staffing the anesthetist and nursing team, as well as the cost of hospitalization and the examinations and tests required before general anesthesia. 22 While a cost, profit and efficiency analysis comparing the 2 surgical settings for flexor tendon repair has not been undertaken, a 2011 study showed that performing open carpal tunnel surgery was 4 times more costly in the OR versus a clinic room. 23 A Pubmed search of the 2 words “WALANT cost” produced 70 publications that support the fact that WALANT is less expensive than traditional sedation/tourniquet surgery. 24
In theory, air requirements for ORs are greater in order to ensure aseptic conditions, which could imply that fewer air changes could lead to more surgical site infections. A total of 25 air changes per hour is the standard for the OR. Conversely, 6 changes per hour are required for PRs. Our study showed no difference in infection rates between the 2 groups despite the 4 times less air change in clinic-based PRs. The evidence that increased air change rates truly affect infection rates is slim at best. 25
Our study has several limitations, beginning with its retrospective design. There is a likely selection bias in that patients were not randomized to the different operative settings. Some important outcome factors, such as range of motion and patient-reported outcomes, were not evaluated. Moreover, confounding factors should be acknowledged. For example, it is possible that the reduction shown in the absolute likelihood of complication is attributable to lesser surgical delay rather than the surgical context in and of itself. A 2019 study by Reito et al observed that a surgical delay of 3 to 7 days was associated with an increased risk of complications. 1
We conducted a single digit analysis to control for the fact that concomitant lesions may have been favored for surgery in the OR. In accordance with the rest of our findings, our single digit analysis demonstrated no significant difference among each of the chosen complication outcomes between the 2 operative settings studied.
To our knowledge, our cohort study is the largest in the literature looking at flexor tendon repairs performed in non-OR PRs. While we were able to observe a decrease in the absolute likelihood of complication of the PR compared to the OR, our study was underpowered to observe significant differences across specific complications (rupture, infection, adhesion, and reoperation). A multicenter randomized study is needed to help investigate this issue more thoroughly.
Conclusion
Among patients undergoing flexor tendon repair of the hand, the PR setting did not put patients at higher risk of complications when compared to patients operated in an OR. These results reveal an opportunity to recognize the many advantages of opting for non-OR PR settings for hand surgery. Future research should focus on prospective studies in which patients are randomized to operative setting. A cost-benefit analysis and environmental impact study to understand and quantify the opportunity cost of PRs for primary flexor tendon repair would be of benefit.
Footnotes
Authors Contributions
Laurent Tessier: literature review, project conception, research protocol preparation, editing, and manuscript writing; Ariane Gélinas: literature review, data collection, and manuscript writing; Alexandra Speak: editing and manuscript preparation; Jacques Haddad: project conception, editing, and manuscript preparation; Donald Lalonde: editing, literature review, and manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
IRB Approval Statement
This retrospective study was approved by the institutional review board of CIUSSS de l’Estrie-CHUS, Comité d’Éthique à la Recherche, #2024-5144. Department of public health also accepted this project. Reference number is S-3002971.
Consent Statement
No consent was obtained directly from patients, since it was impossible to retrace patients with data collected. This was in accordance with IRB recommendations.
Helsinki Statement
This study was conducted respecting Helsinki Ethical Principles for Medical Research.