
Abstract
Introduction
Abdominoplasty is the sixth most commonly performed aesthetic surgical procedure in the world, with the main objective being to reshape the abdominal region by excising redundant skin and fat tissue. 1 Abdominoplasty is typically performed under general anesthesia (GA) with endotracheal intubation. 2 This is an aerosol-generating medical procedure, which requires additional personal protective measures in the context of the COVID-19 pandemic. 3
Surgery under GA leads to long periods of immobilization, which increases the risk of serious systemic complications, such as deep vein thrombosis (DVT) or pulmonary embolism (PE), collectively known as venous thromboembolism (VTE). Previously reported incidences of VTE arising from abdominoplasty range from 0.3% to 2%.1,4 The risk of VTEs increases for patients who undergo abdominoplasty with additional procedures, are over 40 years of age, and have risk factors such as prior VTEs or hypercoagulable states. 5 Moreover, VTE prophylaxis is a controversial issue, with varying recommendations on preoperative actions that can be taken to reduce risk. 6
There has been increasing interest in employing local and/or regional anesthetic for surgical procedures. These techniques, such as tumescent solution and epidural blocks, have been linked to potential advantages, such as lower reported incidence of postoperative complications and earlier ambulation time for patients. 7 Furthermore, local and regional anesthetics can be performed in outpatient settings and are nonaerosol-generating procedures, increasing flexibility for the surgeon. To date, there has been no literature review investigating the safety profile and outcomes of abdominoplasty under conscious sedation, regional anesthesia, and/or local anesthesia.
To better inform clinical practice, we conducted a scoping review of all available literature reporting on the safety and postoperative outcomes of abdominoplasty performed without GA.
For safety, our primary objective was to synthesize data regarding the incidence rate of VTEs. Our secondary objective was to synthesize other relevant adverse event data, including local surgical site complications, unplanned hospitalizations, and the rate of conversion of the procedure to GA. For postoperative outcomes, our primary objective was to summarize postoperative pain scores and patient satisfaction.
Methods
This scoping review was conducted following the PRISMA-ScR protocol for scoping reviews. 8 The PRISMA Extension for Scoping Reviews was used as the reporting guideline for the scoping review manuscript. The protocol has been previously registered on Open Science Framework (OSF: https://osf.io/n5s49).
Eligibility Criteria
Inclusion criteria consisted of (1) any published studies that reported on abdominoplasty procedures with or without liposuction; (2) surgery was conducted under any anesthesia method other than GA. Anesthesia methods included conscious or intravenous sedation, regional anesthetic blocks (RAB: spinals and epidurals), or local anesthesia. Local anesthesia was deemed to be either direct local infiltration of anesthetic (including nerve blocks) or a field block. Any type of study design was included.
Studies were excluded if they (1) did not report on abdominoplasty outcomes or safety; (2) were not published in English; (3) were an abstract or conference proceeding; (4) only reported on postoperative anesthesia use.
Information Sources and Search Strategy
A search strategy was developed in conjunction with a health sciences librarian. The databases searched were MEDLINE, Embase, Web of Science, and CINAHL. The search strategy was based on 2 main concepts: abdominoplasty and non-GA. Relevant subject headings linked to the keywords were included, and the search was conducted on October 19, 2023. A sample search strategy for MEDLINE is provided in Supplemental Table S1.
Study Screening
Two independent reviewers conducted title, abstract, and full-text screening in-duplicate. Screening conflicts were discussed until a consensus was reached. A third reviewer acted as a third opinion if screening discrepancies could not be resolved.
Data Extraction
Data from eligible studies were extracted to an Excel spreadsheet by 2 independent reviewers in-duplicate. Then, both reviewers met to come to a consensus on the extracted data. Any discrepancies were resolved through discussion with a third reviewer. The original data extraction sheet can be found on OSF (https://osf.io/ubveq/?view_only = 90e8f38b828342b2b64ece43a289317d).
Risk of Bias in Individual Studies
The evaluation of the risk of bias was conducted using “ROBINS-I” for nonrandomized studies and “RoB 2.0” for randomized trials.9,10 The outlined tools were employed by 2 separate reviewers (TZ and MH), and a consensus was reached for each domain and for the overall risk of bias. Any disagreements were resolved by a third reviewer (NH). Case reports and series were not evaluated given their inherent high risk of bias.
Synthesis of Results
Descriptive and quantitative analyses were performed when reporting on safety and postoperative outcomes. Safety was primarily defined as the incidence rates of VTEs. Safety also included local surgical site complications, conversion to GA, and unplanned hospitalizations. For postoperative outcomes, we focused on pain scores and patient satisfaction. Tabular methods were used to display study results.
Results
A PRISMA flow diagram outlining study identification and screening is shown in Figure 1. A total of 28 studies satisfied the inclusion criteria. Of these studies, 5 were case reports/series,11–15 18 were retrospective cohort/chart studies,7,16–32 2 were prospective cohort studies,2,33 1 was a randomized prospective feasibility study, 34 1 was a survey, 35 and 1 was a methods paper. 36 The publication dates ranged from 1979 to 2021, with only 5 studies published in the last ten years (2014-2023).2,13,24,33,34 All patients undergoing abdominoplasty without GA were either ASA Class I or II. Studies employed a combination of monitored intravenous (IV) sedation, RAB, and local anesthesia.
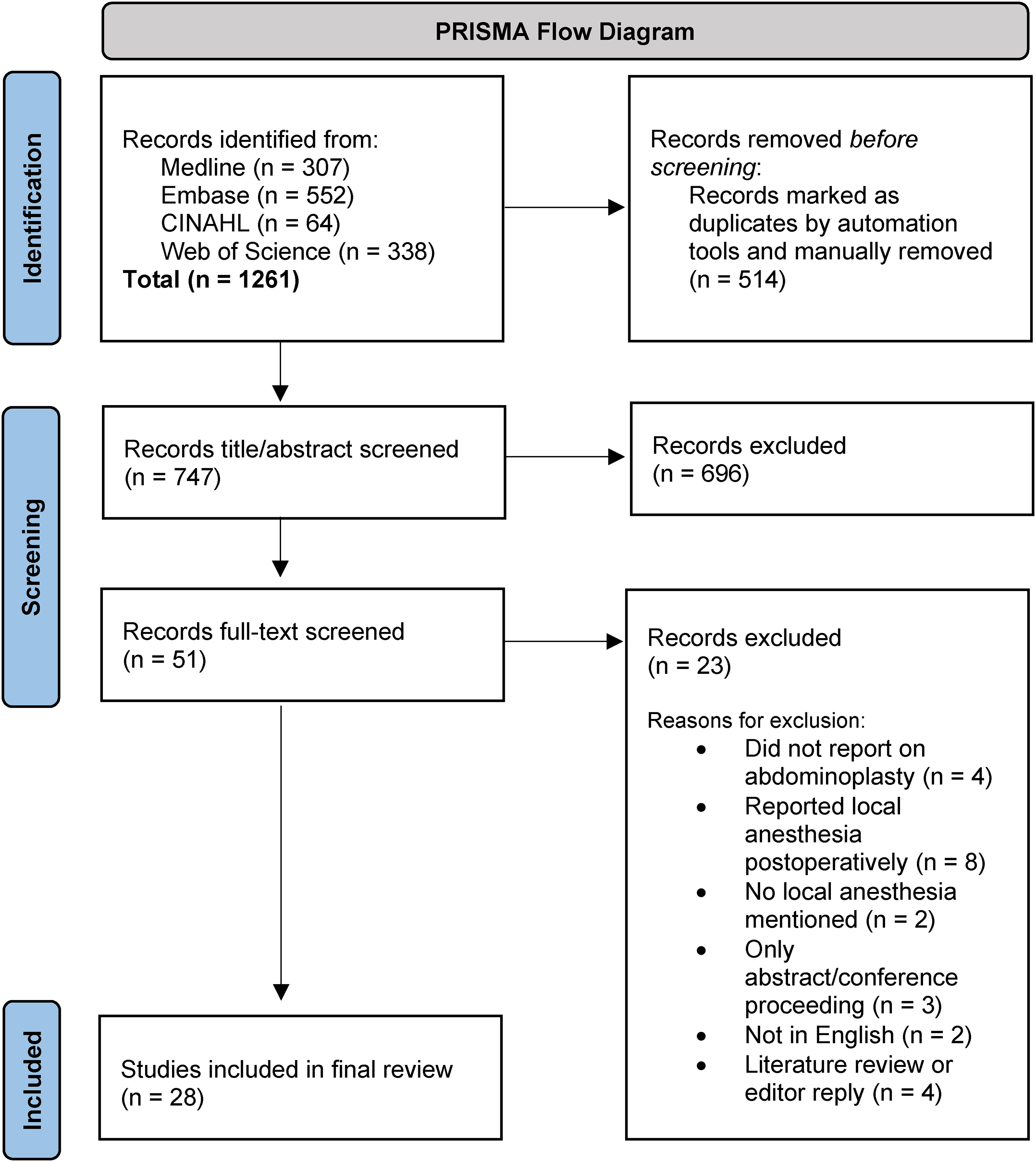
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
Safety Data for Abdominoplasty Without Liposuction
A total of 6 studies reported on abdominoplasty safety outcomes without liposuction.12,18,19,21,27,29 The anesthesia methods were IV sedation and local (n = 5, 83.3%),18,19,21,27,29 and a combination of IV sedation, RAB and local (n = 1, 16.7%). 12 In the 6 studies, a total of 634 patients were included. There were no incidences of any VTEs or other serious adverse events. A total of 45 local complications (7.1%) were reported, with the most common adverse events being seromas (n = 29, 4.6%), local minor tissue necrosis (n = 7, 1.1%), and wound dehiscence (n = 5, 0.8%). Only one study (n = 145 participants) reported on nonsurgical site-related adverse events, which were: postoperative nausea (n = 6, 4.1%), urine retention (n = 1, 0.7%), and hematuria (n = 1, 0.7%). 21 There were no reported conversions to GA, and all patients were discharged the same-day after surgery. Only one patient was hospitalized overnight after surgery, based on patient request for nonsurgical-related reasons. 19 See Table 1 for a summary of safety data.
Safety Data for Abdominoplasty Without General Anesthesia.
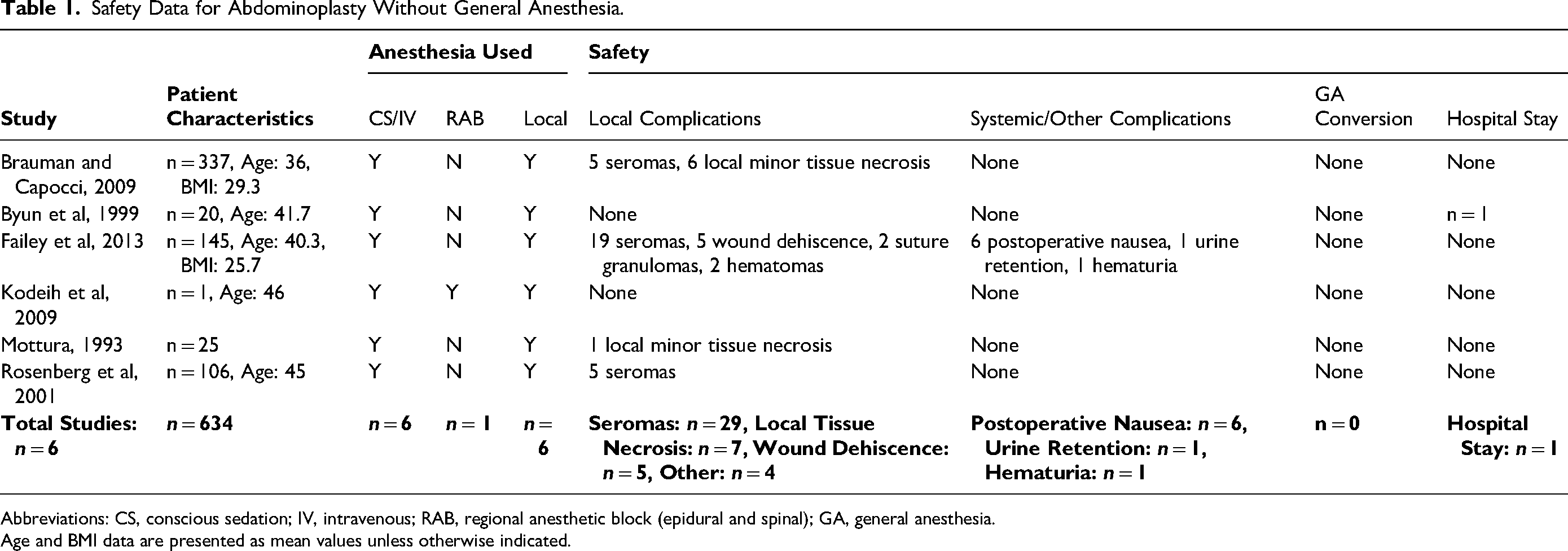
Abbreviations: CS, conscious sedation; IV, intravenous; RAB, regional anesthetic block (epidural and spinal); GA, general anesthesia.
Age and BMI data are presented as mean values unless otherwise indicated.
Safety Data for Abdominoplasty With Liposuction
A total of 14 studies reported on abdominoplasty safety outcomes with liposuction.7,13–16,22,25,28,31–34 The anesthesia methods were IV sedation and local (n = 8, 57.1%),2,7,14,25,28,31–33 RAB and local (n = 3, 21.4%),16,22,34 IV sedation and RAB (n = 2, 14.3%),11,15 and all 3 techniques (n = 1, 7.1%). 13
One study outlined the feasibility and safety of performing abdominoplasties under IV sedation and local anesthesia by presenting data related to over 3000 cases performed by the senior author, but did not specify the number of patients. 7 The study reported no cases of VTEs, occasional postoperative nausea and vomiting, and a seroma rate of < 5%.
In the remaining 13 studies that reported on abdominoplasty with liposuction, a total of 1046 patients were included. There were no reported incidences of VTEs. There were 42 cases of local complications, with the most common adverse events being seromas (n = 22, 4.0%), scar revisions (n = 6, 0.6%), and surgical site infections (n = 4, 0.4%). In 2 of these studies, there were 24 patients who were converted to GA, with an incidence rate ranging from 4.8% to 6%, respectively.22,34 There were no overnight hospitalizations reported. Two studies (n = 160 participants) reported on nonsurgical site-related adverse events, which were: intraoperative nausea (n = 25, 15.6%), intraoperative vomiting (n = 13, 12.4%), postoperative nausea or vomiting (n = 11, 10.5%), and urinary retention (n = 15, 14.3%).2,34 See Table 2 for a summary of safety data.
Safety Data for Abdominoplasty and Liposuction Without General Anesthesia.
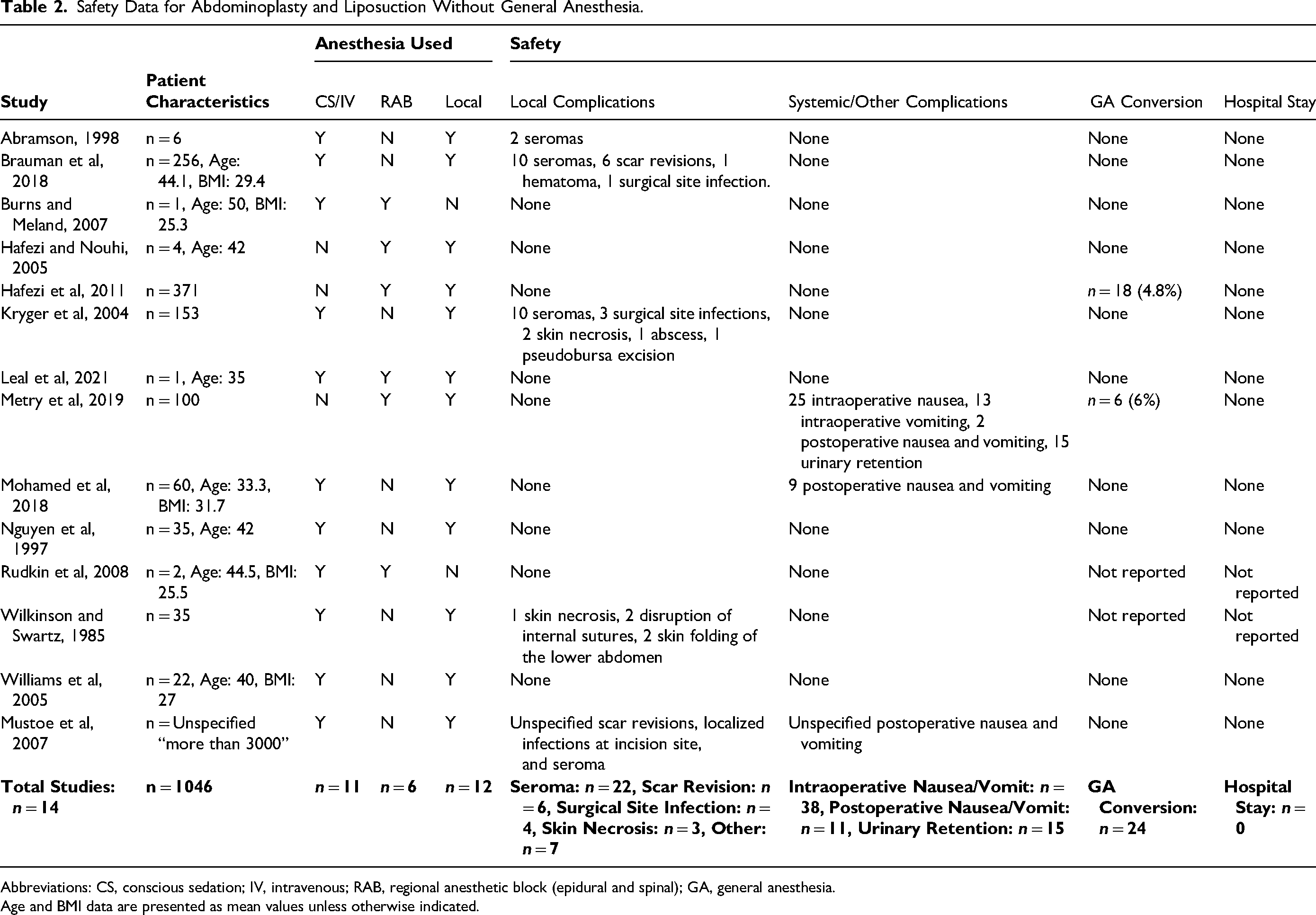
Abbreviations: CS, conscious sedation; IV, intravenous; RAB, regional anesthetic block (epidural and spinal); GA, general anesthesia.
Age and BMI data are presented as mean values unless otherwise indicated.
Safety Data for Abdominoplasty With and Without Liposuction
One study combined safety data for patients receiving abdominoplasty with and without liposuction. Keyes et al investigated the incidence and predictors of VTEs in patients undergoing abdominoplasty with GA compared to IV sedation. 24 A total of 235 274 abdominoplasties under GA and 46 699 cases under IV sedation were analyzed. A total of 201 patients (0.09%) undergoing GA and 30 patients (0.06%) undergoing IV sedation experienced a VTE. The study found no increased VTE risk by type of anesthesia.
Safety Data for Cosmetic Surgeries Performed Without General Anesthesia Including Abdominoplasty
In 5 studies, the authors presented safety information for various cosmetic surgeries conducted without GA, including abdominoplasty. However, the studies did not provide specific details on adverse events solely related to abdominoplasty.
Blake published a study reviewing 4800 patients who had undergone cosmetic surgical procedures performed in an office setting. 17 The anesthetic technique was IV sedation using propofol and ketamine, combined with a local anesthetic injection with intercostal nerve blocks in the cases of abdominoplasty. There were no reported incidences of VTEs, GA conversions, or hospitalizations.
Michaels and Eko 26 reported on 68 patients who underwent abdominoplasty, 29 of which were performed with a rib block and IV sedation. There were no reported incidences of VTEs, GA conversions, or hospitalizations.
Shestak 30 reported on 29 total abdominoplasties, 17 of which were performed with IV sedation and local anesthesia. There were no reported incidences of VTEs, GA conversions, or hospitalizations.
Ersek reviewed over 30 000 cosmetic surgical procedures performed under IV sedation and local anesthetic, including abdominoplasty. 20 There were no reported incidences of VTEs, GA conversions, or hospitalizations.
Hasen et al 23 reported on 169 patients receiving aesthetic procedures, including abdominoplasty, performed under IV sedation with either midazolam/fentanyl or propofol. There were no reported incidences of VTEs, GA conversions, or hospitalizations.
Other
Lewis 36 was a methods paper detailing a procedure labeled “midabdominoplasty,” which requires only local anesthetic. The paper reported that the study author had not yet experienced a complication at the time of publication.
Matarasso et al 35 was a survey investigating the types of anesthesia used by plastic surgeons while performing limited and full abdominoplasties. The study found that of the limited abdominoplasties performed (n = 2003), 11% were done under IV sedation administered by an anesthesiologist, 5% were done by IV sedation administered by the surgeon, and 1% were performed under local anesthesia alone. Of the 11 016 full abdominoplasties performed, 7% used IV sedation administered by an anesthesiologist, and 2% used IV sedation administered by the surgeon.
Abdominoplasty Outcomes
Of the 28 studies, a total of 11 studies reported abdominoplasty outcomes by either assessing patient satisfaction (n = 8),2,18,19,28,29,32–34 pain (n = 2),15,26 or both (n = 1). 23
Of the 8 studies that reported only on patient satisfaction, 5 collected data with either an unspecified satisfaction survey or an unspecified method.18,28,29,32,33 Three of these studies reported that their patients had “high levels” of satisfaction.18,32,33 One study stated that all patients were satisfied with their results, as aesthetics were within patients’ range of expectations. 28 Lastly, one study stated that patients were generally pleased with the results of surgery. 29
The remaining 3 studies outlined their patient satisfaction assessment method. Byun et al 19 administered a satisfaction survey with a 50% response rate (n = 10 participants), showing that all participants returned to normal activities after abdominoplasty under IV sedation within 3 weeks, and that all participants stated that they would be willing to undergo other procedures under IV sedation in the future. Mohamed et al 2 surveyed their patients (n = 60) using a 5-point satisfaction scale. They found that 40% of patients were highly satisfied, 30% were satisfied and would request it again if required, 26.7% had good satisfaction and may request it again if required, and 3.3% had bad satisfaction and would not undergo the procedure again. Lastly, Metry et al 34 compared 2 groups of patients undergoing abdominoplasty, either with GA or a spinal block. The study used an 11-point satisfaction scale, finding that the satisfaction score was higher in the spinal block group but with no statistical significance.
Two studies reported postoperative pain outcomes after surgery. Michaels and Eko 26 compared 2 groups undergoing abdominoplasty, one with GA, and the other with IV sedation and a rib block. An 11-point visual analogue scale (VAS) for pain was employed, showing that the rib block group had statistically significantly less postoperative pain than the GA counterpart. Lastly, Rudkin et al 15 used an 11-point scale to show that both their patients that underwent abdominoplasty with a paravertebral block did not exceed 4/10 pain severity, at either rest or with movement.
One study assessed both postoperative pain and patient satisfaction. Hasen et al 23 compared 2 groups of patients that underwent aesthetic surgeries using IV sedation with either midazolam/fentanyl or propofol alone. The study used an 11-point numerical rating scale for pain, finding no difference between groups. A satisfaction survey was also administered, revealing that 91% to 96% of participants would choose to undergo IV sedation instead of GA for similar procedures in the future.
Risk of Bias Assessment
The results of the risk of bias assessment for included studies can be found in Tables 3 and 4. All nonrandomized studies demonstrated a “serious” or “critical” risk of bias. The one included a randomized controlled trial demonstrated “some” risk of bias. Overall, the risk of bias in analyzed studies is high.
Risk of Bias Assessment for Included Nonrandomized Studies (ROBINS-I).
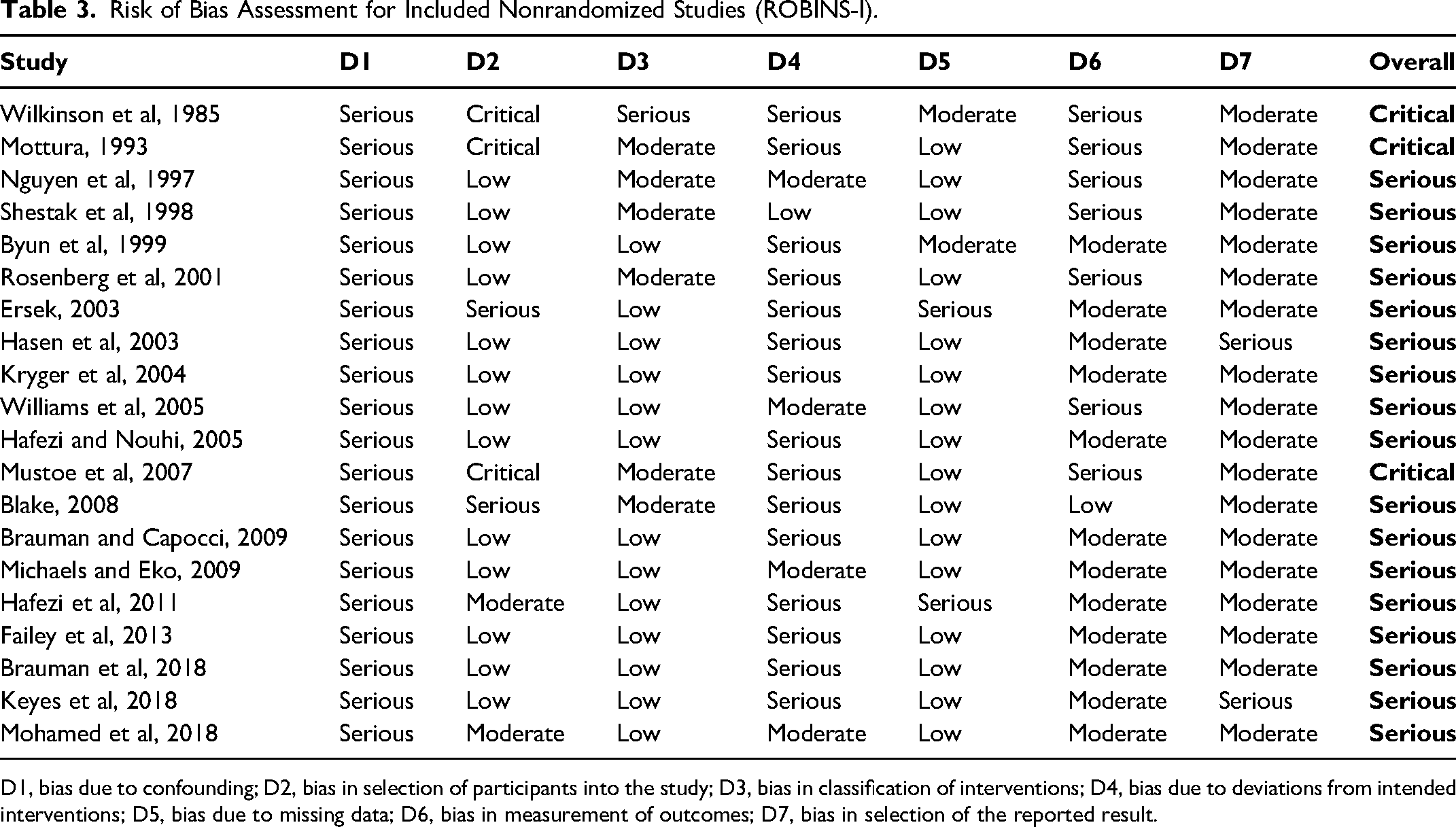
D1, bias due to confounding; D2, bias in selection of participants into the study; D3, bias in classification of interventions; D4, bias due to deviations from intended interventions; D5, bias due to missing data; D6, bias in measurement of outcomes; D7, bias in selection of the reported result.
Risk of Bias Assessment for Included Randomized Controlled Trials (RoB 2.0).
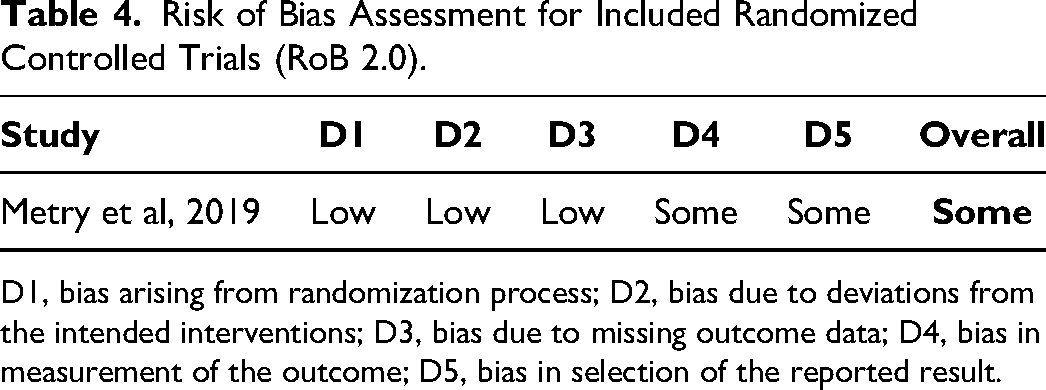
D1, bias arising from randomization process; D2, bias due to deviations from the intended interventions; D3, bias due to missing outcome data; D4, bias in measurement of the outcome; D5, bias in selection of the reported result.
Discussion
Our review highlights preliminary evidence that suggests abdominoplasty without GA is safe and feasible. A total of 21 studies reported on abdominoplasty-specific safety data with and without liposuction for 48 379 patients. Of these cases, there were 30 reported cases of VTEs, and no hospitalizations due to excessive pain. There was a combined VTE incidence rate of 0.06%. This is lower than VTE incidence rates of abdominoplasty with GA reported by other reviews (0.3%-2%).1,4 The 11 studies that reported on postoperative pain and/or patient satisfaction showed that abdominoplasty with GA was well-tolerated, and that patients had a favorable opinion of surgeries performed without GA.
The low VTE incidence rate reported when performing abdominoplasty without GA parallels findings from other surgeries. Previous studies investigating procedures such as facelifts, blepharoplasties, and aesthetic breast surgeries performed without GA have demonstrated favorable safety profiles, with low VTE incidence rates, shorter operative times, and faster times to ambulation for patients.37–39 For example, a survey of VTE incidence rates following facelift surgery found that procedures performed under local anesthesia had shorter operative times and a lower VTE rate when compared to facelifts performed under GA. 40 Earlier ambulation and shorter length of surgery are both factors associated with decreased thrombosis risk, which may help to explain possible lower VTE incidence when surgeries are performed without GA. 41 Although the existing literature on the benefits of performing plastic surgery procedures without GA appear promising, data from other surgical specialties remains conflicting. Studies investigating procedures performed by orthopedic and general surgeons without GA have shown mixed data on whether surgeries done under local and/or regional anesthesia improve the safety profile.42–44 Our review highlights the safety of abdominoplasty without GA, demonstrated by a low overall VTE incidence rate (0.06%). However, it is difficult to delineate whether performing abdominoplasty without GA has an inferior, equivalent, or superior safety profile to abdominoplasty with GA due to the lack of comparative studies. Further research is required to validate our findings and to compare the safety profile of abdominoplasty under different anesthetic modalities.
In the 11 studies that reported on postoperative pain scores and patient satisfaction, abdominoplasty without GA was well-tolerated. Results reported by the studies generally showed high satisfaction with minimal postoperative pain. This finding bolsters existing evidence that plastic surgery procedures performed without GA have favorable patient satisfaction and an acceptable pain profile. Stahl et al performed aesthetic breast surgeries under sedation and local anesthetic, finding that the majority of patients were satisfied with their anesthesia and had well-controlled pain. 45 However, the methodology used for assessing postoperative outcomes among studies included in our review remains lacking. The majority of outcome data was not assessed using validated outcome measurement tools, and there was a paucity of information on outcome assessment methodology. 46 Only 44.4% (n = 4/9) of studies reporting on patient satisfaction specified the assessment method, and none of these studies employed validated outcome assessment tools. This increases the risk of bias and makes it difficult to synthesize postoperative outcome data between studies. To improve the quality of assessment methodology, the use of patient-reported outcome measures, such as the BODY-Q, should be employed when assessing abdominoplasty to ensure the collection of accurate, comprehensive data on clinically meaningful outcomes from a patient's perspective. 47 Our review suggests that abdominoplasty without GA is well-tolerated by patients and is feasible to perform. There is still a lack of robust data to comprehensively evaluate the procedure from a patient perspective and to compare outcomes between studies due to high heterogeneity in assessment methodology.
All included nonrandomized studies were found to be at “high” or “serious” risk of bias. Of the 28 studies analyzed by our review, there was only one randomized controlled feasibility study comparing abdominoplasty under GA to RAB and IV sedation. 34 This highlights a paucity of high-quality, prospective studies to draw conclusions from. Currently, available evidence suggests that abdominoplasty without GA is safe and has favorable postoperative outcomes. However, surgeons should consider that there remains minimal high-quality evidence to guide clinical practice when performing abdominoplasty without GA.
Our review highlights 3 key research areas requiring further improvement: (1) the lack of comparative studies on postoperative outcomes and safety for abdominoplasty with versus without GA; (2) the limited use of validated outcome assessment tools; and (3) the paucity of high-quality studies available to establish evidence-based recommendations. Future studies on abdominoplasty without GA should focus on addressing these gaps to improve the quality of research produced, to better inform practicing surgeons, and to optimize outcomes for patients undergoing abdominoplasty without GA.
Limitations
The lack of high-quality studies limited the quality of conclusions that could be drawn. There was high heterogeneity in postoperative outcome assessment methods, limiting the ability to synthesize data.
Conclusions
This review provides preliminary evidence that performing abdominoplasty without GA is safe, feasible, and well-tolerated by patients. Our review stresses the need for additional, well-designed comparative studies to further validate our findings. There is currently a paucity of high-quality evidence to base recommendations, and surgeons should employ their judgment and expertise when performing abdominoplasty without general anesthesia.
Supplemental Material
sj-docx-1-psg-10.1177_22925503241301711 - Supplemental material for Investigation of Abdominoplasty Without General Anesthesia: A Scoping Review
Supplemental material, sj-docx-1-psg-10.1177_22925503241301711 for Investigation of Abdominoplasty Without General Anesthesia: A Scoping Review by Ted Zhou, Madeline E. Hubbard and Nasimul S. Huq in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503241301711 - Supplemental material for Investigation of Abdominoplasty Without General Anesthesia: A Scoping Review
Supplemental material, sj-docx-2-psg-10.1177_22925503241301711 for Investigation of Abdominoplasty Without General Anesthesia: A Scoping Review by Ted Zhou, Madeline E. Hubbard and Nasimul S. Huq in Plastic Surgery
Footnotes
Acknowledgments
The authors would like to thank Seddiq Weera for providing guidance on the research protocol.
Author Contributions
All authors were involved in conceptualizing and designing the scoping review. TZ and MH conducted screening and analysis for the scoping review with interpretation from NH. TZ and MH drafted the manuscript and all authors revised it critically. The final manuscript was approved to be published by all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study is a scoping review consisting of previously peer-reviewed, published articles; therefore, no ethics approval was required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.