
Abstract
Introduction
Transgender and gender diverse (TGD) individuals are those who identify as a gender that differs from their sex assigned at birth. Stigma towards the transgender community has led to widespread prejudice, discrimination, and acts of violence.1–3 Recent decades have brought significant activism and resulted in the TGD community becoming more visible, vocal, and accepted within society. 1 This increased visibility and acceptance has brought forth improved awareness of the healthcare gaps faced by the TGD community with many provinces and territories working towards increasing their medical services and support systems for their transgender populations. However, as social acceptance has increased, so too has the number of transgender people seeking medical and surgical care to assist with their gender transition, resulting in an ongoing national problem with access to gender-affirming healthcare. 4
Access to gender-affirming surgeries (GAS) has been difficult for many TGD individuals in Canada. The primary barriers limiting access to GAS are a paucity of qualified surgeons and disparities in access and coverage of care between each province.5,6 Clinics that offer GAS are geographically limited to a few high-volume centres in urban areas. 6 The breadth of GAS procedures includes facial GAS, chest surgery, body contouring, and a spectrum of genital procedures. Due to the breadth of procedures and training requirements to perform them proficiently, very few clinics, even specialized centres are able to offer the full spectrum of surgical options. In order to navigate these challenges, it is critical for TGD patients to have easy-to-access resources that detail the location of clinics that offer GAS and to know which procedures specifically are available and covered under their regional insurance plans.
While there is an abundance of studies on the barriers to accessing GAS, there is no study that examines the current landscape of GAS care in Canada, including insurance coverage of procedures, and a list of services provided. The purpose of this study is to determine and provide an overview of what surgical interventions are covered under the insurance plan of each Canadian province. This will highlight ongoing gaps in insurance coverage and identify geographic regions where the development of specialized GAS programs should be prioritized.
Methodology
This cross-sectional study was conducted by visiting each provincial Health Ministry webpage in Canada on March 1, 2024. Specifically, data was extracted from the webpage that discussed provincial insurance coverage for GAS procedures. In addition, provincial health authorities and gender clinics were contacted via email or telephone to determine which gender-affirming procedures were offered within the province or referred out-of-province.
Data was extracted and added to an Excel (Microsoft Corp., Redmond, Washington) generated table (Table 1). Data regarding coverage was collected for GAS procedures listed in World Professional Association of Transgender Health (WPATH) guidelines (SOC 8). With the data collected, summary tables were constructed illustrating which procedures are covered under public health insurance in each province (Tables 1-3). Furthermore, the geographic distribution of where GAS is performed in Canada is shown in Table 4. The general categories of GAS are listed as available in-province, available out-of-province along with name of the province where the procedure is completed.
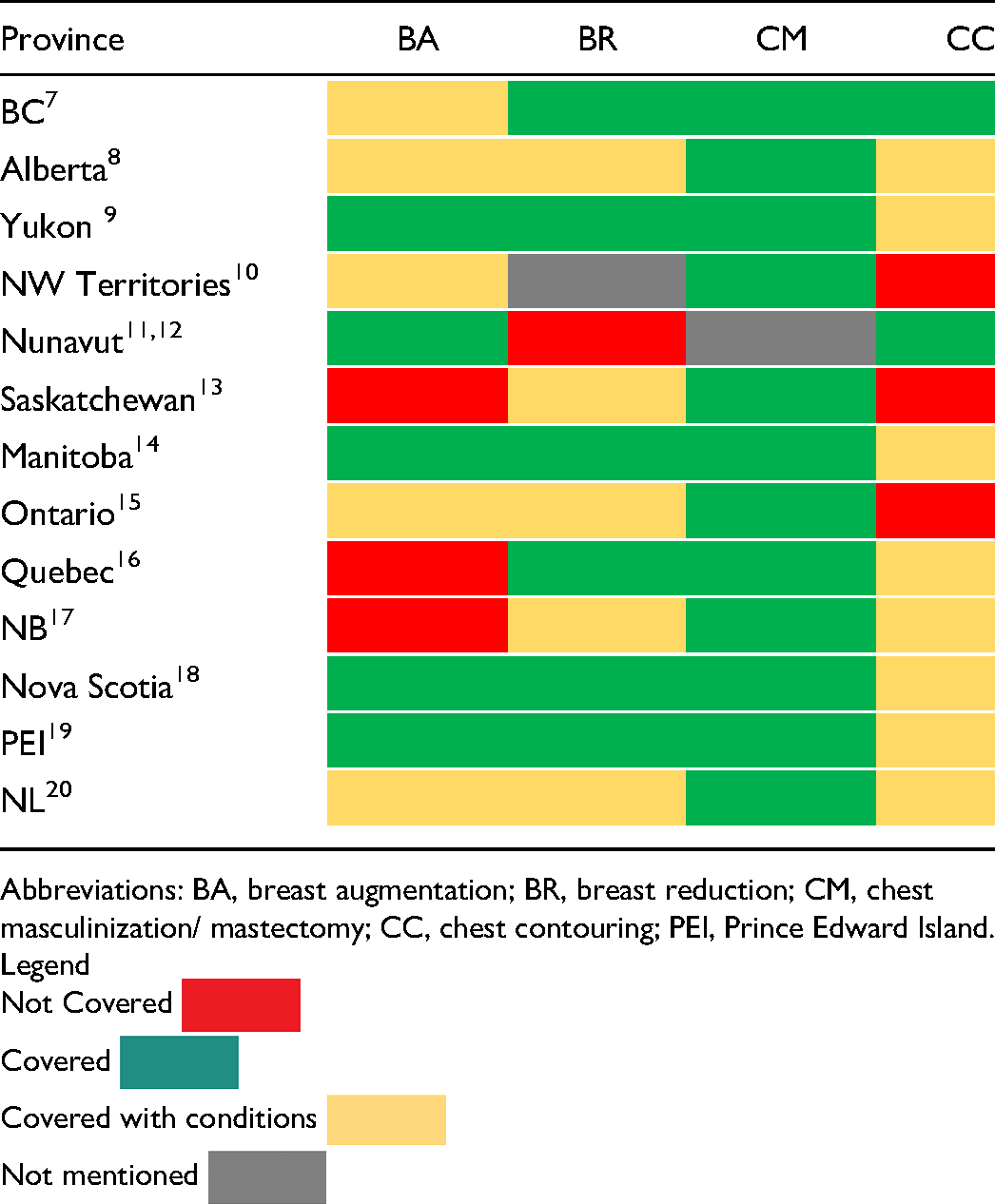
Coverage of Chest Gender-affirming Procedures by Province.
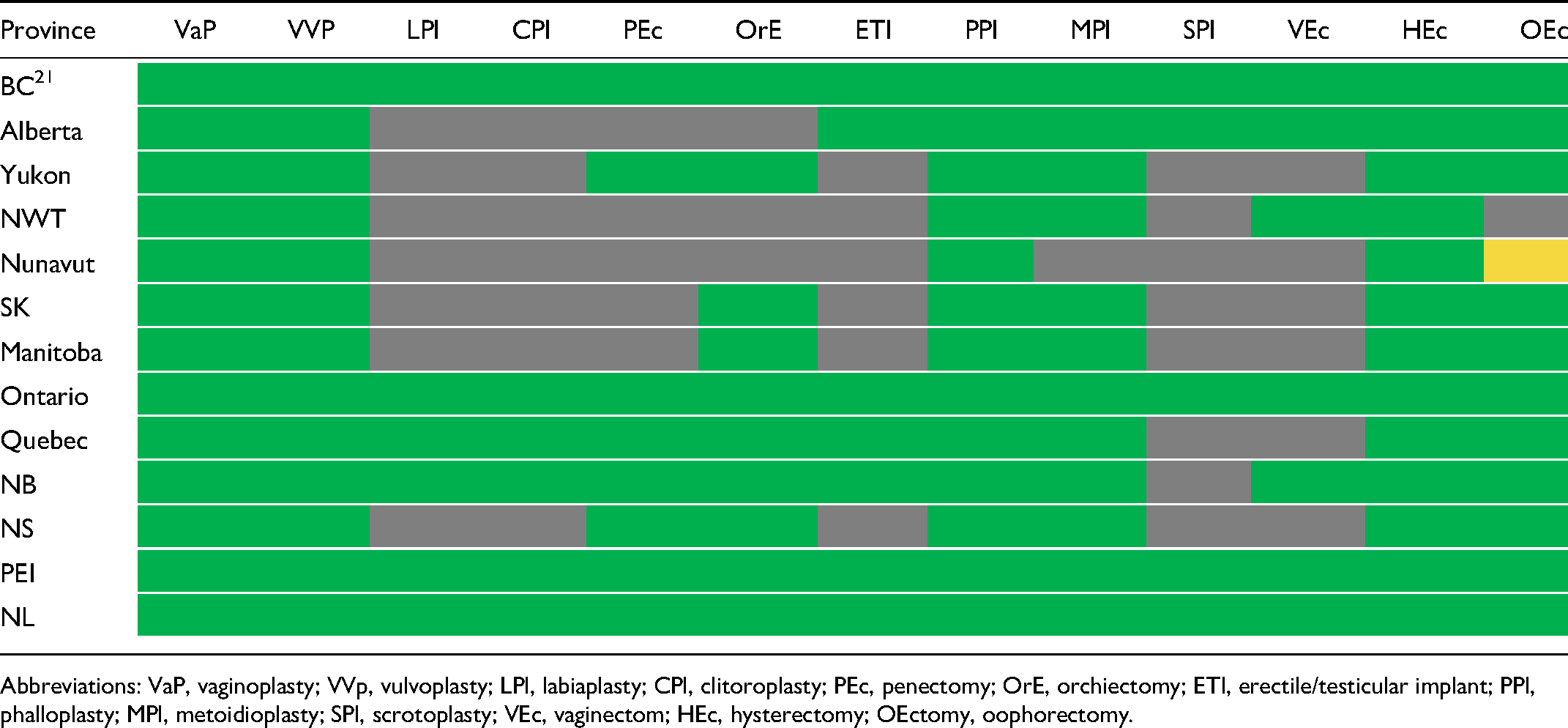
Coverage of Feminizing and Masculinizing Lower Body Surgeries by Province.
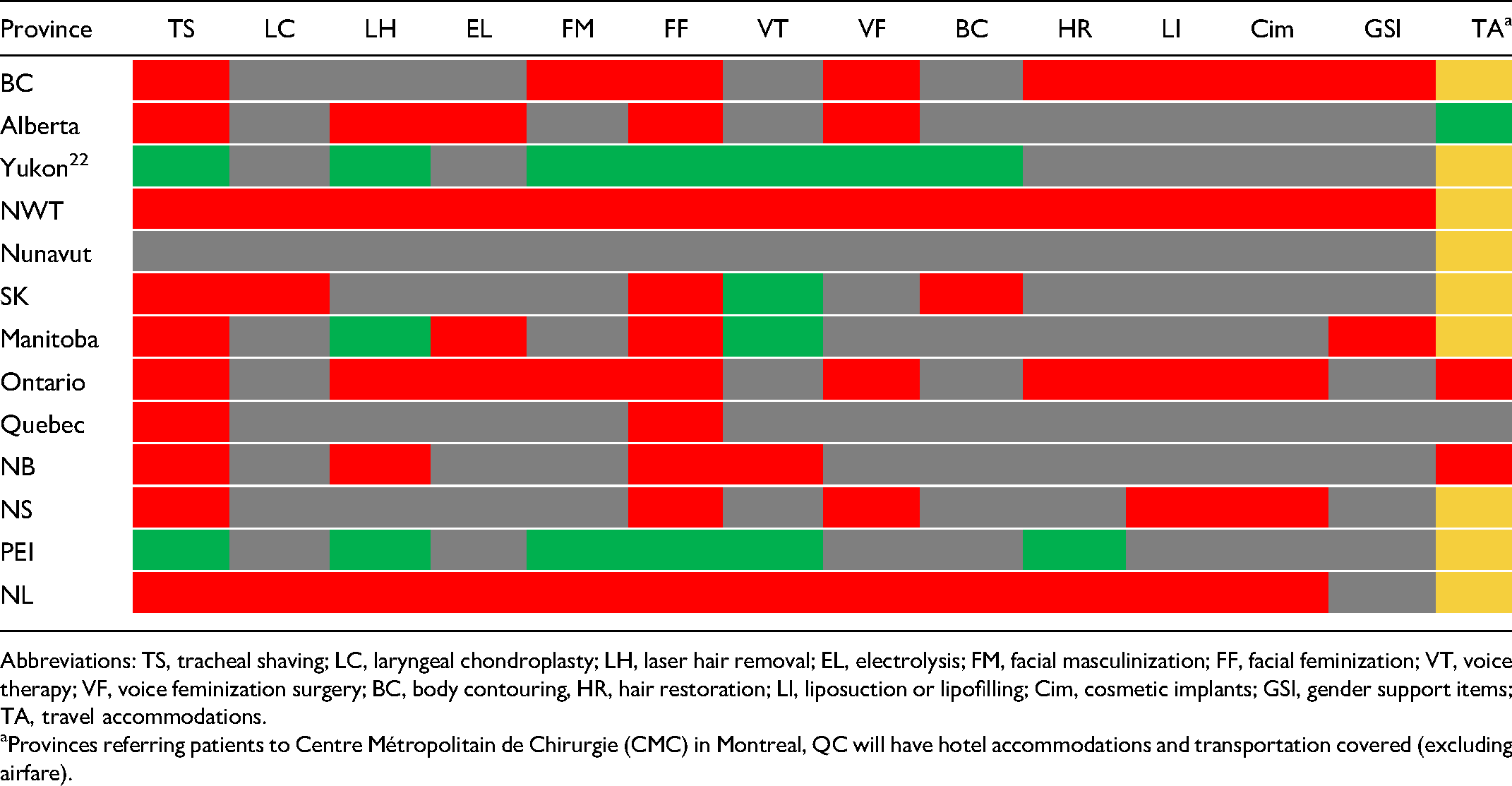
Coverage of Gender-affirming Facial and Additional Procedures and Accommodations by Province.
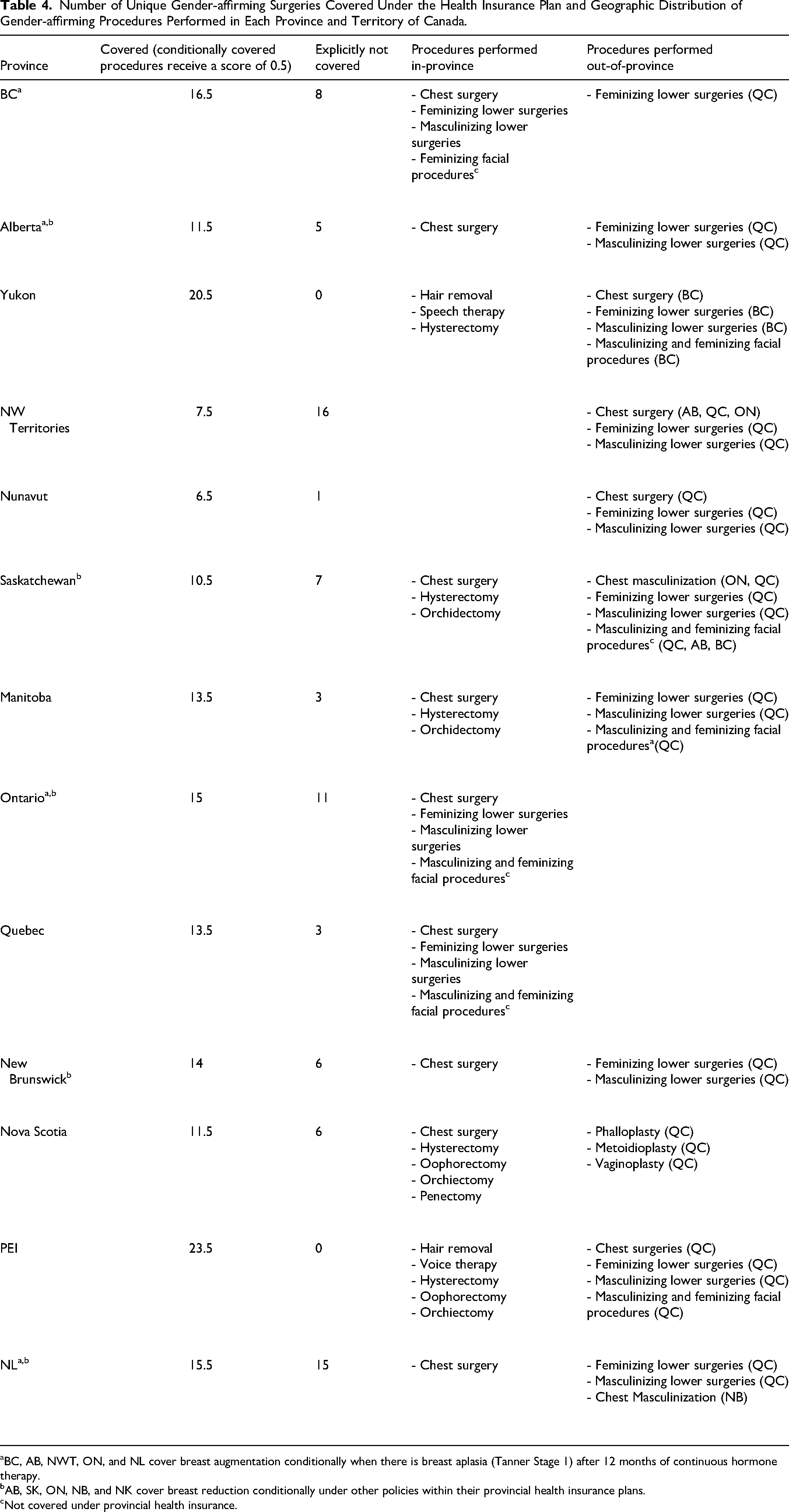
Number of Unique Gender-affirming Surgeries Covered Under the Health Insurance Plan and Geographic Distribution of Gender-affirming Procedures Performed in Each Province and Territory of Canada.
BC, AB, NWT, ON, and NL cover breast augmentation conditionally when there is breast aplasia (Tanner Stage 1) after 12 months of continuous hormone therapy.
AB, SK, ON, NB, and NK cover breast reduction conditionally under other policies within their provincial health insurance plans.
Not covered under provincial health insurance.
Results
Upon completion of data extraction, it was determined that all 13 Canadian provinces and territories have at least some insurance coverages of GAS, to varying degrees. Gender-affirming procedures were divided into several categories: (i) chest surgery, including breast augmentation, breast reduction, chest masculinization/mastectomy, and chest contouring; (ii) feminizing lower surgeries, such as vaginoplasty, labiaplasty, clitoroplasty, penectomy, and orchiectomy; (iii) masculinizing lower surgeries, such as erectile/testicular implant, phalloplasty, metoidioplasty, scrotoplasty, vaginectomy, hysterectomy, and oophorectomy; (iv) feminizing and masculinizing facial and additional procedures, such as tracheal shaving, laser hair removal, electrolysis, laryngeal chondroplasty, facial masculinization, facial feminization, voice therapy, voice feminization surgery, body contouring, hair restoration, liposuction or lipofilling, and cosmetic implants. Coverage of supporting items and travel accommodations were also examined.
For chest surgery (Table 1), breast augmentation procedures are publicly insured in 5/13 provinces. An additional five provinces cover breast augmentation conditionally when there is breast aplasia (defined as Tanner Stage 1) after 12 months of continuous hormone therapy. Breast reduction is covered in 11/13 provinces, with 6/13 provinces covering it under GAS policies and 5/13 provinces covering breast reduction conditionally on the basis of other medical conditions (eg, chronic back and shoulder pain). 12/13 provinces covered mastectomy while two provinces covered chest contouring explicitly and another eight provinces provided coverage for chest contouring conditionally as part of a mastectomy.
For feminizing lower surgeries, vaginoplasties and vulvoplasties are covered by health insurance in every province (Table 2). Orchiectomies (10/13), penectomies (8/13), clitoroplasties (6/13), and labiaplasties (6/13) are mentioned explicitly in the GAS policies by most provinces. For masculinizing lower surgeries (Table 2), phalloplasties and hysterectomies were covered by all provinces. Oophorectomies (12.5/13) and metoidioplasties (12/13) are covered under the health plan policies of most provinces. Meanwhile, erectile/testicular implants (7/13), vaginectomies (7/13), and scrotoplasties (5/13) are mentioned by around half of the provinces in their coverage plans.
For feminizing and masculinizing facial and additional procedures, voice therapy (4/13), laser hair removal (3/13), facial masculinization (2/13), facial feminization (2/13), tracheal shaving (2/13), body contouring (1/13), voice feminization surgery (1/13), and hair restoration (1/13) are covered by a minority of provinces across Canada (Table 3). Electrolysis, laryngeal chondroplasty, liposuction or lipofilling, and cosmetic implants are not covered under any provincial insurance plan.
Gender supporting items such as chest binders, breast prosthetics, bras, and packing straps are not covered under any provincial health insurance plan. Travel accommodations are only covered in two provinces conditionally if the procedure occurs outside of the province or if patients are referred to Centre Métropolitain de Chirurgie (CMC) in Montreal, Quebec.
In total, there are 32 unique gender-affirming procedures or procedural components mentioned in the coverage plans of at least one Canadian province or territory, with an average coverage of 14/32 unique GAS procedures (Table 4). Prince Edward Island (PEI) covers the highest number of unique gender-affirming procedures. Nunavut covers the lowest number of unique gender-affirming procedures.
Table 4 also shows a list of general categories of procedures performed in-province versus out-of-province. In Canada, Quebec and Ontario offer the greatest number of in-province procedures, being the only provinces that offer feminizing and masculinizing lower surgeries and facial-affirming surgeries in province. Comprehensive program development in Ontario is recent and in early stages, including a new program in Ottawa offering consultations as of 2024. British Columbia offers both feminizing and masculinizing lower surgeries. While British Columbia also offers facial-feminizing procedures within the province, this is done through private cosmetic practices and is not covered publicly. 9/10 provinces offer chest surgeries within their province. In contrast, none of the three territories offer gender-affirming procedures in-province, except for hysterectomies performed in Yukon. Quebec receives the most referrals from out-of-province. These referrals include provinces that offer these procedures within their own province, but due to patient volume continue to send some patients out-of-province to better meet demand.
Discussion
This is the first study completed to survey the landscape of Canadian coverage of GAS procedures, as well as provide an overview of gender-affirming procedures performed in each Canadian province and territory. Coverage of GAS procedures in Canada varies greatly under individual provincial healthcare plans. Genital surgeries are covered most commonly, with all provinces covering vaginoplasty and phalloplasties. The high proportion of provincial coverage for genital surgeries may be explained by societal and medical association between assigned gender identity and the possession of specific genitalia. Although wide coverage exists for genital gender-affirming procedures, there is an overall lack of granularity regarding the extent of coverage. There is a need for additional clarity in this regard as many genital surgery patients will need secondary or staged procedures to achieve their functional and/or aesthetic goals.
At least one breast/chest surgical procedure is covered in all provinces. Chest masculinization/mastectomy is the most covered chest surgery procedure, covered in all provinces except Nunavut. Chest contouring is mentioned minimally, despite being a critical component of many gender-affirming chest surgeries. However, techniques of chest contouring/masculinization include mastectomy through various approaches depending on breast size, skin amount, and size of nipple-areolar complex. 23 This suggests that the coverage of chest contouring in Canada may be broader since it is often performed under the label of a mastectomy. It is also important to note that while there is less coverage nationally for breast reduction as compared to mastectomy under GAS policies, there are other policies under which breast reductions are covered within various provinces. For instance, Ontario Health Insurance Plan (OHIP) will cover breast reduction if the procedure is deemed medically necessary (eg, patients experience chronic pain in the neck, back, and shoulders, skin irritation, and hinderance of physical activity). Therefore, patients are able to get breast reduction covered through other policies in addition to GAS-specific policies.
Breast augmentations are covered unconditionally in five provinces, while conditionally covered in five other provinces requiring the patient to be on at least 12 months of hormone therapy with evidence of breast aplasia and/or remaining at Tanner Stage 1. Compared to widespread provincial coverages of mastectomies, breast augmentations are covered considerably less by Canadian provinces. It is possible that breast augmentations may be less frequently covered due to their association with cosmetic surgery. However, a high percentage of transfeminine patients will experience insufficient breast development with hormone therapy, requiring augmentation to achieve their goals and relieve their chest dysphoria.
Another trend seen was that very few provinces covered non-genital and non-breast procedures such as facial-affirming surgeries and body contouring in their health insurance plans. As a result, patients must pay out-of-pocket for the additional expenses of facial-affirming procedures, tracheal shaving, hair removal, and body contouring. The reason for lack of coverage may be due to the overlap with cosmetic and aesthetic procedures for non-TGD people which are viewed as elective procedures. However, procedures such as facial surgery can profoundly affect how a transgender person moves through society and dramatically alter gender presentation, and aid in social transition. The medical necessity of facial-affirming surgery for many transgender people has been recognized with increased numbers of transgender patients receiving facial-affirming surgery despite the average cost of such procedures rising in the United States.24,25 Patients who underwent facial feminization surgery reported significant improvements in facial aesthetic satisfaction and other aspects of quality of life following surgery. 26 Furthermore, the newest standards of care from WPATH Guidelines (SOC 8) show literature backed evidence that highlights the importance of facial surgeries on patient well-being. 27
Overall, there is near complete coverage of genital surgeries and many chest procedures covered in the majority of Canadian provinces, while the coverage for facial surgery is lacking almost entirely. Yukon and PEI are the only two provinces to offer gender-affirming facial surgeries. On July 21, 2023, PEI expanded its coverage of gender-affirming procedures to become the province with the most comprehensive coverage of GAS care in Canada. 19 This is due to years of advocacy driving policy change by provincial leaders working with members of Health PEI and Gender Affirming Care PEI to expand coverage of GAS to support TGD patients using up-to-date peer-reviewed medical guidelines. Furthermore, the expansion of PEI's coverage is also driven by the need to decrease financial barriers to procedures important for gender expression such as voice therapy, facial-affirming surgeries, in line with WPATH guidelines.28,29
Despite broad coverage, there is a large disparity between coverage of genital procedures and in-province availability with most provinces sending patients to Quebec for genital surgery or other types of GAS. A well-established clinic operating for over 50 years, most provinces and territories refer their patients to GrS Montréal. The BC Gender Surgery Program at Vancouver General Hospital is the only program performing masculinizing and feminizing lower surgeries in Western Canada and receives referrals from in-province patients and out-of-province patients from Yukon. There are new GAS clinics emerging including at The Ottawa Hospital where a new clinic welcomed referrals including genital surgery starting January 2024, and a program in Toronto where vaginoplasty has been offered. Given the large population of Ontario, there is a need to grow and expand these programs to be able to meet provincial demands. There is currently no comprehensive GAS program located in the Prairie Provinces, territories, or the Maritimes. TGD patients in Northern Canada from all three territories have perhaps the most limited access to GAS in Canada. This is likely due to the paucity of specialists who can perform these procedures and a relative lack of availability of surgical care in general.
Importantly, this study captured the coverage of other expenses associated with surgical care such as travel and gender support items. Of the Canadian provinces or territories, only Alberta and Yukon explicitly provided funding for travel and accommodations for patients. 9 However, this was also conditional as coverage only applied to patients who were travelling outside the province for treatments. While seeming secondary to the surgical procedures, the importance of covering costs of travel is critically important due to the lack of access to many surgical procedures, particularly genital surgery in most Canadian provinces. The biggest barrier to GAS access identified in the literature was high financial costs. 30 As a result, financial aid for income compromised TGD individuals in Canada will be a crucial factor in improving access to GAS care until specialized gender surgery programs are available in every province.
While this study offers a comprehensive view of the landscape of GAS in Canada, there are some limitations. Some procedures not mentioned on provincial GAS websites may be covered via another policy within the provincial health plan. For instance, breast reduction can be additionally covered in five other provinces when the procedure is determined to be ‘medically necessary’ by a surgeon. 31 Furthermore, the terminology and language surrounding GAS procedures and coverage can be ambiguous or poorly defined. There are specific GAS procedures in this study whose coverage is underestimated because they were not explicitly mentioned on provincial health websites. These procedures may instead be covered under the ‘umbrella procedure’ that encompasses the entire anatomical structure. For example, vulvoplasties are also known as zero-depth vaginoplasties. By definition, every province covering vaginoplasties would also cover vulvoplasties. Another example of this is chest contouring. While chest contouring may involve mastectomy, additional excision of fat and skin from the chest may be performed in addition to a mastectomy. Chest contouring may include additional add-ons such as chest liposuction and lateral chest work that some surgeons consider cosmetic and others treat as part of the mastectomy procedure. There is a need to clarify coverage of these chest contouring adjuncts. Due to the inconsistent use of language surrounding GAS procedures, some gender-affirming procedures covered in some provinces are underreported. This may lead to misinformation for patients attempting to determine whether their procedures are covered under their provincial health plan. Therefore, there is a need for greater transparency and standardization of terminology on provincial health websites so that it is clearer which procedures are truly covered by the GAS health plan of each province.
There are also plastic surgeons who perform GAS procedures (eg, breast augmentation and mastectomy) as part of their practice, many of whom are not working out of specialized academic or GAS programs. For other specialties like urology and gynaecology, this would include physicians performing orchiectomy and hysterectomy. Some of these surgeons may not have been captured within the limits of the study design. Nonetheless, this paper is the first to synthesize and compile the most up-to-date insurance coverage data of all the provinces and territories in Canada for GAS. While there are third-party websites that compile coverage and availabilities of GAS procedures, many are no longer up-to-date, or have inaccurate information regarding availability of procedures. 32 For instance, some surgeons listed as offering procedures often do not actually perform this procedure in practice (eg, phalloplasty). 32 The landscape of GAS coverage is changing rapidly in the recent years, with provinces across Canada providing more coverage for gender-affirming procedures. While some policy changes may occur following publication of this article, this piece is timely as it summarizes the current state of gender-affirming care at a crucial moment, when most provinces and territories are in active discussion and exploration of their coverage plans.
Additional studies will be needed in the future to track the progress of providing complete and accessible GAS care to transgender individuals across Canada.
Conclusion
Significant heterogeneity exists across Canada with respect to coverage for GAS procedures. Genital gender-affirming procedures are covered the most comprehensively across provinces and territories in Canada. Breast/chest surgeries are covered by most provinces and territories in Canada; however, there is a discrepancy regarding coverage for mastectomy versus breast augmentation and reduction, with less coverage available for augmentation and reduction. Despite their medically necessary status for the transgender population, facial-affirming surgeries, laser hair removal, and voice affirmation surgeries were not covered by any provinces and territories except for Yukon and PEI. Relative to coverage for many GAS procedures, there is a paucity of specialized GAS clinics across Canada, representing an urgent discordance between procedure coverage versus procedure availability. Many provinces cover a variety of GAS procedures that are not locally/regionally available, necessitating at best travel to access care with suboptimal follow-up, or at worst no actual access to a covered procedure. Physicians need to continue advocating for both wider coverage of GAS procedures and coordinate with provincial and national leadership to prioritize the targeted training, recruitment, and retention of surgeons specialized in GAS techniques. Access to this care should be in accordance with the WPATH guidelines which support facial, chest, and genital-affirming surgeries as medically necessary procedures that significantly increase patient well-being and quality of life.
Footnotes
Author Contributions
Alan Gou: contributed to study design, data acquisition, data extraction, analysis of results, drafting of the manuscript, final approval of the manuscript, and agrees to be held accountable for all aspects of the work. Michelle Bonapace-Potvin: contributed to study design, data acquisition, analysis of results, drafting of the manuscript, final approval of the manuscript, and agrees to be held accountable for all aspects of the work. Blair R. Peters: contributed to study design, drafting of the manuscript, final approval of the manuscript, and agrees to be held accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statements
This article does not contain any studies with human or animal subjects.