
Abstract
Introduction
The prevalence of cleft lip and/or palate in Canada is approximately 15.10 per 10,000 live births. 1 In Alberta, Canada, the prevalence of cleft lip and/or palate in Indigenous children is significantly higher than non-Indigenous children. 2
The diagnosis of cleft lip and/or palate can be difficult for families and caregivers as these patients require numerous surgical and non-surgical treatments throughout the course of their lives. 3 Care for these children is traditionally delivered in a multidisciplinary clinic setting, beginning just after birth and extending into adulthood. High-quality care is imperative to ensure optimal outcomes for speech, hearing, orthognathic function, appearance, and social integration. 4 As it relates to providing comprehensive care to patients with a cleft lip and/or palate, their cultural and faith backgrounds must be an important consideration. 5
Indigenous peoples have existed across North America since time immemorial and presently account for 5.1% of the population in Canada. 6 Colonization has led to the destruction of traditional ways of life following the implementation of colonial and genocidal practices that include residential schooling systems. Lasting effects can be seen broadly across healthcare today and include inaccessible healthcare services, poor care delivery and the evidenced experience of medical racism. 7 Compared to non-Indigenous Canadians, Indigenous people across Canada face shorter lifespan and are disproportionately affected by both physical and mental health burdens of disease, likely a legacy of colonization and subsequent impacts on social determinants of health. 8 Importantly, stereotyping and medical racism faced by Indigenous patients may lead to poorer quality of care and death. 9 While it is well recognized that both timely and safe access to surgical care remains vital to the overall health of a population, Indigenous peoples are more likely to experience higher rates of mortality and adverse events after surgery, as well as lower rates of surgical utilization in Canada.10–12
Currently, traditional Indigenous health and wellness practices are not routinely integrated within the healthcare system. 9 As it relates to the methodologies used in our study, the Blackfoot medicine wheel is composed of four quadrants that represent spiritual, mental, physical, and emotional domains of health. Emotional health refers to the ability to process and manage both negative and positive emotions. Physical health is the overall health of one's physical being. Spiritual health is our ability to relate to our cultural and spiritual practices, guided by our relation to the creator. Mental health is our ability to cope with stressful or difficult situations, allowing us to feel at ease. All aspects of the medicine wheel are interconnected and must be in harmony with one another to achieve optimal health. The Blackfoot medicine wheel is unique to the tribes belonging to the Blackfoot Confederacy of Treaty 7 within Alberta that include Kainai, Piikani, and Siksika. The medicine wheel as a cultural teaching and framework is used by some Indigenous groups across Canada with various meanings and interpretations based on region or cultural customs.13–15 It is important to consider cultural relevance to specific Nations for similar work in other parts of Canada and internationally.
Indigenous patients with cleft lip and/or palate in central and southern Alberta receive team care from the Alberta Children's Hospital cleft palate clinic in Calgary. Southern and central Alberta is home to the people of Treaty 7 that include the Blackfoot Confederacy, Stoney Nakoda, Tssu’Tina, and Métis Nation of Alberta Region 3.
To date, there have been no published studies demonstrating the experiences of Indigenous patients receiving cleft lip and/or palate care in Canada. This small-scale qualitative study explores the experiences of Indigenous patients and their families receiving care for cleft lip and/or palate in Southern Alberta. This work hopes to contribute to the foundational literature on this topic that can also inform future care in a way that is reflective and cognizant of Indigenous ways of life and lived experiences. This research was led and co-authored by two Indigenous people (HS and PR) to ensure ongoing commitments to both ethical and culturally guided research.
Methods
Indigenous research methodologies are critical when conducting research with Indigenous peoples. These methodologies are rooted in relational accountability, placing significant emphasis on who the researchers are accountable to and who they seek to build relations with by conducting this research. 16 By asking such questions Indigenous research methodologies strive to pursue knowledge while also fulfilling a relational obligation to the subjects whereby the researcher is seen as accountable, using gained knowledge for the betterment of the relationship. Storytelling and personal narratives such as those used in qualitative research embody these principles as often a relationship is built between the researcher and the participant. 16
This qualitative study used an Indigenist approach to qualitative research and was grounded in the worldview of the Indigenous project leads. 17 Participants were recruited via purposive and snowball sampling through community networks and public advertising in relevant healthcare spaces.
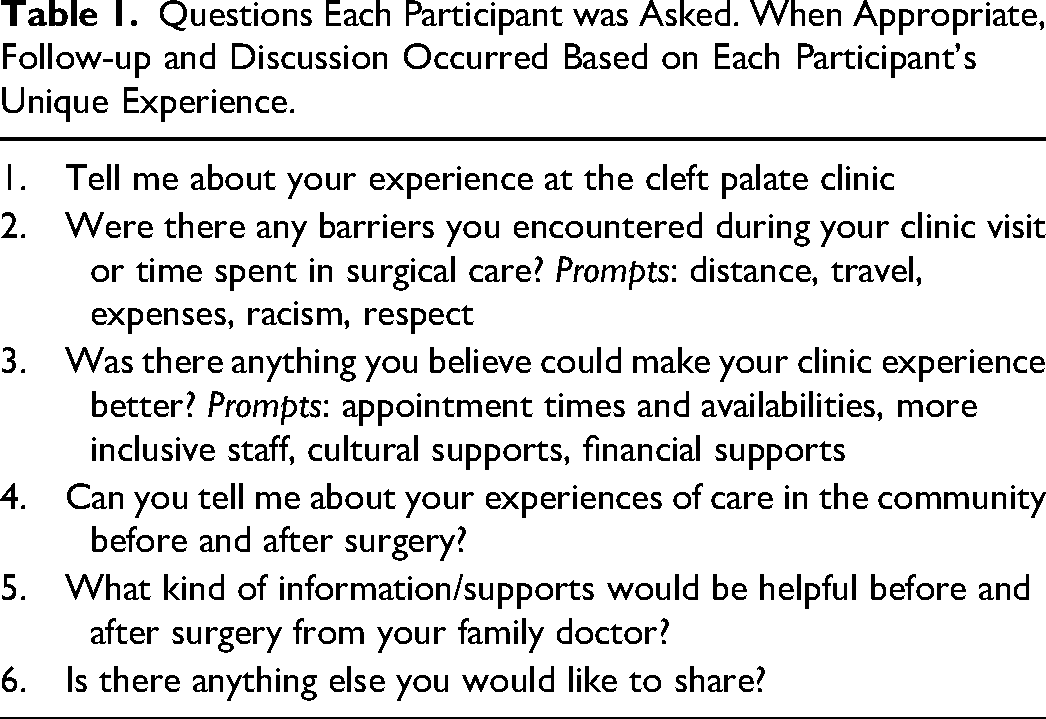
A semi-structured qualitative interview guide, included six open-ended questions, was developed by the research team which included content, methodological, and clinical experts, (Table 1). Interviews were conducted by the first author (HS). Participants were also invited to share additional experiences if they felt there was any information that was not covered by the interview guide. Interviews were conducted by telephone and online videoconferencing, at the preferences of the participants. Each interview was recorded using a digital voice recorder, anonymized, and professionally transcribed verbatim by an REB-approved third-party transcription service. Interview transcripts were then verified by the first author and analyzed using NVivo 12. Thematic analysis was completed by both Indigenous and non-Indigenous study team members. 18 Descriptive codes were created line by line and were reviewed by the study team to generate thematic analysis in alignment with the medicine wheel.
Questions Each Participant was Asked. When Appropriate, Follow-up and Discussion Occurred Based on Each Participant's Unique Experience.
The themes that were generated through the thematic analysis were further categorized in the context of the traditional Blackfoot medicine wheel (Figure 1). Traditional teachings of the medicine wheel were provided by a Blackfoot elder through the first author's traditional teachings received growing up in her community.
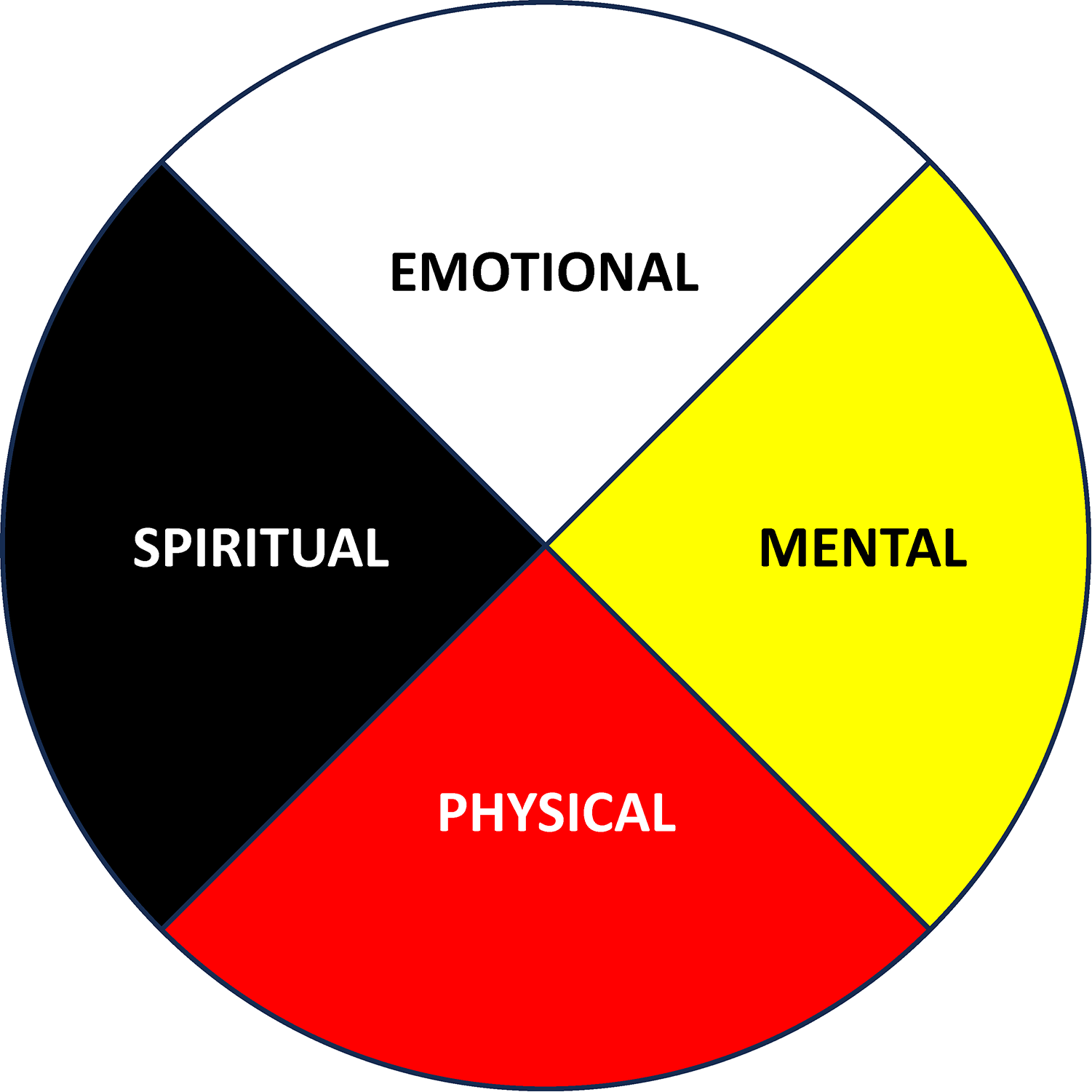
A typical rendition of the Blackfoot medicine wheel that represents a traditional and Blackfoot version of health.
The project was approved by the University of Calgary Conjoint Health Research Ethics Board, REB21-15884.
Results
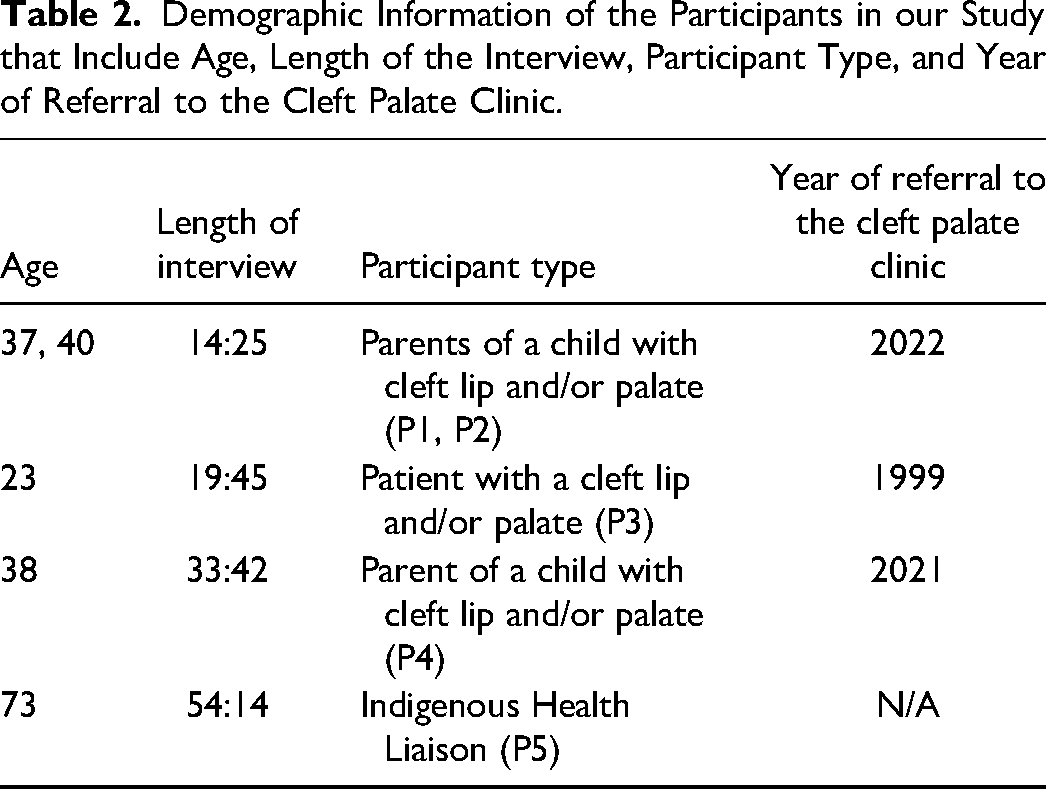
There were five participants interviewed in the study including: the parents of a child receiving cleft lip and/or palate care, patients, and Indigenous liaisons (Table 2).
Demographic Information of the Participants in our Study that Include Age, Length of the Interview, Participant Type, and Year of Referral to the Cleft Palate Clinic.
In general, participants highlighted a lack of attention to cultural and spiritual components of the cleft lip and palate care they have received. In particular, the traditions of smudging practices and support from Indigenous elders were not considered. Participants also shared the lack of access to or representation by Indigenous physicians and healthcare providers involved in their care teams. Themes are further characterized in the context of the medicine wheel, which as mentioned above requires wellness in all domains to achieve optimal health.
Emotional Health
Participants described a significant emotional toll associated with having a child born with cleft lip and palate as it relates to the medicine wheel concept of emotional health. One participant described feeling especially burdened by their perception that the journey of patients with cleft lip and/or palate is life long and impacting on nearly every facet of life. Participants also described difficulty in finding and implementing coping strategies for living with the diagnosis of cleft lip and/or palate The covid-19 pandemic further complicated these emotional challenges. “It was scary, and I was in there [in the clinic] alone, and there wasn’t much that could be done because it was covid”. (P4) “They [parents and patients] had a really hard time… having a child with cleft palate”. (P5) “(we) take it day-by-day, step-by-step.” (P1, P2)
Physical Health
Participants described a physical toll that cleft lip and/or palate has on both the patient and their families/caregivers. Like all patients and families, Indigenous patient and families were challenged with babies’ and children's associated difficulties with feeding, ear infections, hearing, speech and language development, and dental issues. Some patients’ family members or caregivers were also concurrently experiencing demands on their own physical health that added to the complexities of their child's journey. “I’d just had surgery… I had to go take him [to the hospital]. Only one parent was allowed. So, it was just me. Mom goes with the baby. And I was just in so much pain. He was barely eating. It was kind of scary.” (P4)
Spiritual Health
Participants highlighted both the lack of spiritual care received and the benefit that spiritual care have played in their family's cleft lip and/or palate journey. Among participants, spiritual care was considered vital to their overall well-being and health. Critical elements of spiritual care that were considered lacking included access to traditional smudging ceremonies and access to the advice and wisdom of elders. On the contrary, one participant shared that spiritual health was not a domain pertinent to their cleft lip and/or palate journey; this highlights that, as among non-Indigenous families, there may be variability among families’ feeling about the importance of formal spiritual practices in a healthcare setting. It was generally felt that spiritual needs should at least be asked about with both Indigenous and non-Indigenous families. “Elders would have definitely been helpful, [as] they just kind of keep focus on everything.” (P4) “We need more cultural supports. There wasn’t really any that I recall”. (P4) “Being more spiritual helps me to keep in tune with my intuition.” (P4) “… smudging and prayers… [and] Having elders come in (would be helpful)” (P1, P2) “I’m not really spiritual”. (P3)
Mental Health
All participants described a general feeling of being not completely comfortable in the cleft palate clinic setting. In particular, they felt that their culture and lived experience was not understood by the clinic staff, indeed mirroring the Indigenous experience in broader Canadian society in general. Some perceived bias and racism. All experienced feelings of lack of safety because of the presence of very few Indigenous healthcare staff associated with the clinic and difficulty in connecting with other cleft lip and/or palate families. All felt that the feeling of personal safety could have been increased in the setting with greater contact with Indigenous healthcare experts and other Indigenous families. “I would have been more at ease… knowing they actually did care… about my culture.” (P4) “I know I would feel safe if I was being helped by another Native doctor because they can be more understanding.” (P3) “[It is important to know] how racism affects a person, and what is racism? Sometimes we need to understand our own biases.” (P5) “…It would be beneficial to also meet other … native families that dealt with (cleft lip and palate) … because it is a big [issue]… you don’t think of it as but is a common thing in Native children.” (P1, P2)
Discussion
Having a cleft lip and/or palate is a complex and overwhelming situation for all patients and their families. Their care is complex, extends over many years and requires the expertise of a variety of healthcare professionals. Multidisciplinary cleft palate clinics exist in all major Canadian centers to help manage the burden of this condition by providing centralized and coordinated care for these children. While this is generally seen as the provision of optimal care for children with cleft lip and/or palate, the experience of Indigenous patients and their families in this model of care has not previously been considered. Currently at the Cleft Palate Clinic, a social worker meets with each patient's family/care providers upon their initial clinic visit and referral. The social workers role includes assisting each family/care provider with resources that include a referral to the existing Indigenous Liaison at the Alberta Children's Hospital. Indigenous liaison services are extended to all patients and their families/care providers at the Alberta Children's hospital. As such, resources may be stretched to meet patient needs.
Our findings suggest that from the perspective of Indigenous patients and families, the condition impacts their well-being in all four domains of the traditional Indigenous medicine wheel. Understanding Indigenous patients’ experience of their own health journeys as it relates to their way of life is critical in providing patient-centered and culturally safe care. Regarding spiritual health, Indigenous patients should be offered access to spiritual health supports that include elder support smudging ceremonies. It is well known that elder support, when provided, can contribute to both equitable and culturally safe care. 19 In June 2023, Alberta Health Services enacted policy that explicitly protects Indigenous patients’ right to practice traditional ceremonies such as smudging at the bedside or in a ceremonial space. 20 Such policies are vital to ensuring that Indigenous patients have the ability to maintain and engage with spiritual and cultural practices while receiving healthcare and must be considered across Canada. It is critical that Indigenous patients have access to both their traditional Indigenous healing and western/biomedical medicine to achieve holistic healthcare. 21 As declared by the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP), Indigenous peoples have the right to access their traditional medicines in addition to maintaining their own health practices. 22 This study is an important benchmark of Indigenous patients’ experiences prior to such policy changes. Additionally, though the policy now exists, the operationalization and culture change that is required to appropriately enact this policy change may be slow and so an understanding of current experiences is critical.
Regarding mental, physical, and emotional health, it is clear that Indigenous patients with cleft lip and/or palate and their families face direct challenges to these aspects of their overall well-being and health. Due to the complex nature of cleft lip and/or palate care and the demands placed on all aspects of health, awareness regarding the challenges these patients and their families face is required. Future directions that can serve to enhance the care provided by the cleft palate clinic or other multidisciplinary cleft clinics across Canada include ensuring the patients have timely access to Indigenous health liaisons. It will also be important to undertake Indigenous-led work with additional families who have experienced care recently and in different geographic areas to align policy and health services changes with local cultural worldviews. Indigenous health liaisons can contribute advocacy and support, working in collaboration with cleft care teams to provide not only patient and family support but also to organize receiving financial support from sources such as Jordan's Principle funding, Non-Insured Health Benefits (NIHB) or Reserve/Band funding. Additionally, more Indigenous doctors should be trained in surgery to advocate for and provide culturally safe care to Indigenous patients with surgical conditions. The Truth and Reconciliation Call to Action 23 calls for more Indigenous peoples being trained as professionals in healthcare fields and is recognized as a national level priority.
Limitations of our study include the small sample size of participants. We recognize that given the legacy and past experiences of research involving Indigenous peoples, there may be hesitancy to participate in research. 23 This is an important consideration to ensure that future research involving Indigenous patients is both sensitive to this cultural context and ethically guided.
Finally, attention to wellness in the four domains of the traditional Indigenous medicine wheel could be extended to inform better care for all children and families (Indigenous and non-Indigenous) receiving care in pediatric multidisciplinary clinics in Canada.
Conclusion
It is imperative that Indigenous patients receiving cleft lip and/or palate care are provided care that is cognizant of both their cultural needs identified in our study but also reflective of the ways in which health may be conceptualized for Indigenous patients in order to improve experiences and outcomes for Indigenous children and their families.
Footnotes
Acknowledgements
We would like to thank all of the patients, families, and staff at the Alberta Children's Hospital for their important contributions to this project.
Author Contribution
Haley Shade: study analysis, background research, conducted participant interviews, obtained ethics approval, manuscript creation and revision. Robertson Harrop: study analysis, manuscript creation and revision, clinical expertise. Donald McPhalen: study analysis, manuscript creation and revision, clinical expertise. Pamela Roach: study analysis, background research, obtained ethics approval, manuscript creation and revision, Indigenous health, and research expertise.
Previous Presentation
Presented at the 76th Canadian Society of Plastic Surgery Annual Meeting in June of 2023 as a poster presentation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Indigenous Primary Health Care and Policy Research Network, (grant number Seed grant).
Ethics
University of Calgary Conjoint Health Research Ethics Board REB21-15884.