
Abstract
Introduction
Plastic surgery is a highly visual field, and reliance on visual data is paramount in the diagnosis, planning, treatment, and follow-up of patient outcomes. Despite this, there remain disparities in the representation of racial and ethnically diverse populations in plastic surgery materials. An analysis by Massie and colleagues of over 25,000 color images published across six plastic surgery journals and the New England Journal of Medicine reveals that only 22% of images were non-White. 1 This trend is very apparent in breast-related surgery literature, with non-White skin representing only 8% of images, 2 and in general medical textbooks, with overrepresentation of light skin tone as seen in 74.5% of images.2,3 Reports from the field of dermatology, which is similarly reliant on visual recognition for diagnoses, reveal few resources providing images of lesions on darker skin despite clinical differences in the presentation of pathology.4,5
The paucity of skin tone diversity in educational materials carries important implications for patient outcomes. Although melanoma is more prevalent in non-Hispanic White populations, survival in Black, Asian American/Native American/Pacific Islander, and Hispanic populations is significantly lower. 6 Racialized groups more commonly present with ulceration, advanced disease, distant disease, and thicker tumors.7,8 Factors leading to delayed diagnosis include differences in clinical presentation, paucity of educational materials, and a subsequent knowledge gap. 7 Research shows that having access to images of skin cancers in patients of darker Fitzpatrick skin types results in increased diagnostic confidence. 9 Residency training provides much of the exposure needed to make accurate clinical diagnoses; however, more than 30% of chief residents denied having didactic sessions focused on skin of color. 10
In addition to the importance of diversity in educational materials, there is also a need to improve racial and ethnic diversity in surgery trainees and faculty to optimize patient compliance, trust, and overall outcomes. While there has been an increase in some visible minority populations among trainees in plastic and reconstructive surgery, there is substantial underrepresentation of Black and Hispanic trainees and staff in the United States,11–13 even despite an increase in Black medical graduates and applicants. 14 Similar trends are seen among general surgery residents in Canada, with a recent survey revealing that 70% of residents did not identify as a visible minority. 15
The disparities in depicting diversity in medical education materials have sparked various global initiatives. In 2020, a clinical handbook called “Mind the Gap” was created to highlight clinical signs and symptoms in darker skin tones. 16 Recently, medical students at Queen's University have led efforts to improve the skin tone diversity of images shown by faculty in dermatology lectures. 17 Similar to dermatology, plastic surgery learning is heavily reliant on images and visual representations of various conditions.
Our project seeks to build upon this advocacy work by examining photographs from the current curriculum and associated seminars at a Canadian plastic surgery residency program. While we are focusing on skin tone diversity in this project, it is important to recognize the importance of other identifying characteristics such as ethnicity, gender, and the intersectionality of these features.
Methods
Image Collection
Images were selected from recorded lecture seminars from the plastic surgery resident education curriculum at a Canadian institution. At our center, the seminar lectures from the plastic surgery resident education curriculum comprised the primary modality of structured teaching delivered by faculty members and were thus used as source material. Associated seminar notes typically included pictorial (ie, drawing) but not photographic images, and therefore were not included in analysis. The study was approved by the research ethics board of a large tertiary care center, and we received permission from faculty education leads to use teaching images in this study. All images between May 2020 and December 2021 were screened for inclusion in the study by two investigators. The plastic surgery resident education curriculum is based on 3 years; therefore, a half cycle of lectures was selected for review in this study. All colored images from the presentation slides of each lecture were indexed for the purposes of this study. Exclusion criteria included nonhuman subjects, illustrations, radiological images, and identifiable individuals within the department. At the time of analysis, only images with visible skin were included. This ensured that there was broad initial inclusion of images, with further distillation prior to analysis to meet the inclusion and exclusion criteria.
Data Analysis
A photogrammetric analysis was conducted on all eligible images by four independent reviewers including two plastic surgery residents and two senior medical students. The Fitzpatrick scale, a subjective skin tone classification, was used to assess each image with skin. 18 A Fitzpatrick number ranging from I (pale white skin) to VI (dark brown and black skin) was assigned to each image. 19 Data were then grouped into the following categories: Fitzpatrick I to III (light), IV to V (medium), and VI (dark). These categorizations were determined based on descriptions of white (Fitzpatrick I-III) and nonwhite (Fitzpatrick IV-VI) skin found on DermNet and previous similar research classifying skin tones1,2,20 with a further grouping of nonwhite skin tones into Fitzpatrick IV to V and Fitzpatrick VI. Discrepancies in the Fitzpatrick type between investigators were resolved through consensus. 21
Survey
A survey regarding perceptions of skin tone diversity in the resident curriculum was sent out to residents and faculty of the Division of Plastic, Reconstructive and Aesthetic Surgery (PRAS). Informed consent was obtained through a detailed document outlining the project's aims and the participant's role prior to the start of the survey. The survey was developed by the research team based on relevant literature. The study was then piloted to two faculty colleagues in Dermatology and two faculty colleagues in Plastic Surgery for expert feedback. The survey was developed on an online platform, Qualtrics XM V122021 (Utah, USA), and the wording of questions was modified slightly for resident and faculty versions to better capture relevant demographic information and assess differing perceptions. For example, the statement “I believe it is difficult for lecturers to find photographs of patients with darker skin tones” was provided to residents in the survey, whereas “I find it difficult to find photographs of patients with darker skin tones” was provided to faculty. Likert scale questions were developed to assess several statements regarding diversity in photographs in lectures, and overall equity, diversity, and inclusion (EDI) opportunities in the division of PRAS. Complimentary statement responses were matched between resident and faculty surveys based on what the statement sought to identify (ie, “The faculty is committed to providing EDI initiatives” (faculty survey) and “There is commitment to provide EDI opportunities for residents” (resident survey)).
Statistical Analysis and Interrater Reliability
Data were analyzed with SPSS V28.0. 22 The number of images in each category was counted and characterized according to the Fitzpatrick score as described above. Standard deviation was reported for each set of lectures. Nonparametric Mann–Whitney U test was used to calculate significant differences between the means of Fitzpatrick types I to III, IV to V, and VI across all lectures. Two-tailed t-test was used to calculate significant differences in photographic diversity in each lecture when compared to the aggregate. All tests were calculated with a significance value of P < .05.
Interrater reliability was determined using Fleiss’ kappa on the basis of Landis and Koch's cutoffs. 23 Twenty-two images which were deemed representative of the general content were randomly selected from the lecture slides, and each was used for categorization. Kappa scores were interpreted with Landis and Koch guidelines as follows: 0 to 0.2 slight agreement; 0.21 to 0.40 fair agreement; 0.41 to 0.60 moderate agreement; 0.61 to 0.80 substantial agreement; 0.81 to 1.0 almost perfect agreement.
Results
Image Analysis
A total of 96.25 h were analyzed across 30 lectures, resulting in 1990 images included for analysis. This represents images from all recorded seminars between May 2020 and December 2021, which comprise a half-cycle of lectures delivered in the plastic surgery education curriculum. Examples of lecture topics covered include thermal injury, skin and soft tissue, and craniofacial surgery.
Of the images included for analysis, 83.2% (1656 ± 47.5) were Fitzpatrick type I to III, 13.1% (260 ± 10.98) were Fitzpatrick type IV to V, and 3.7% (74 ± 6.48) were Fitzpatrick type VI (Supplemental Figure 1). Overall, there was a statistically significant difference between the number of images characterized as Fitzpatrick types I to III and Fitzpatrick types IV to V (P < .001), as well as Fitzpatrick types I to III and type VI (P < .001). In total, 26/30 (86.7%) lectures contained one or more Fitzpatrick type IV to V images, and 10/30 (25%) contained one or more Fitzpatrick type VI images. Fleiss’ Kappa score was calculated to be 0.896 between four interraters, representing almost perfect agreement.
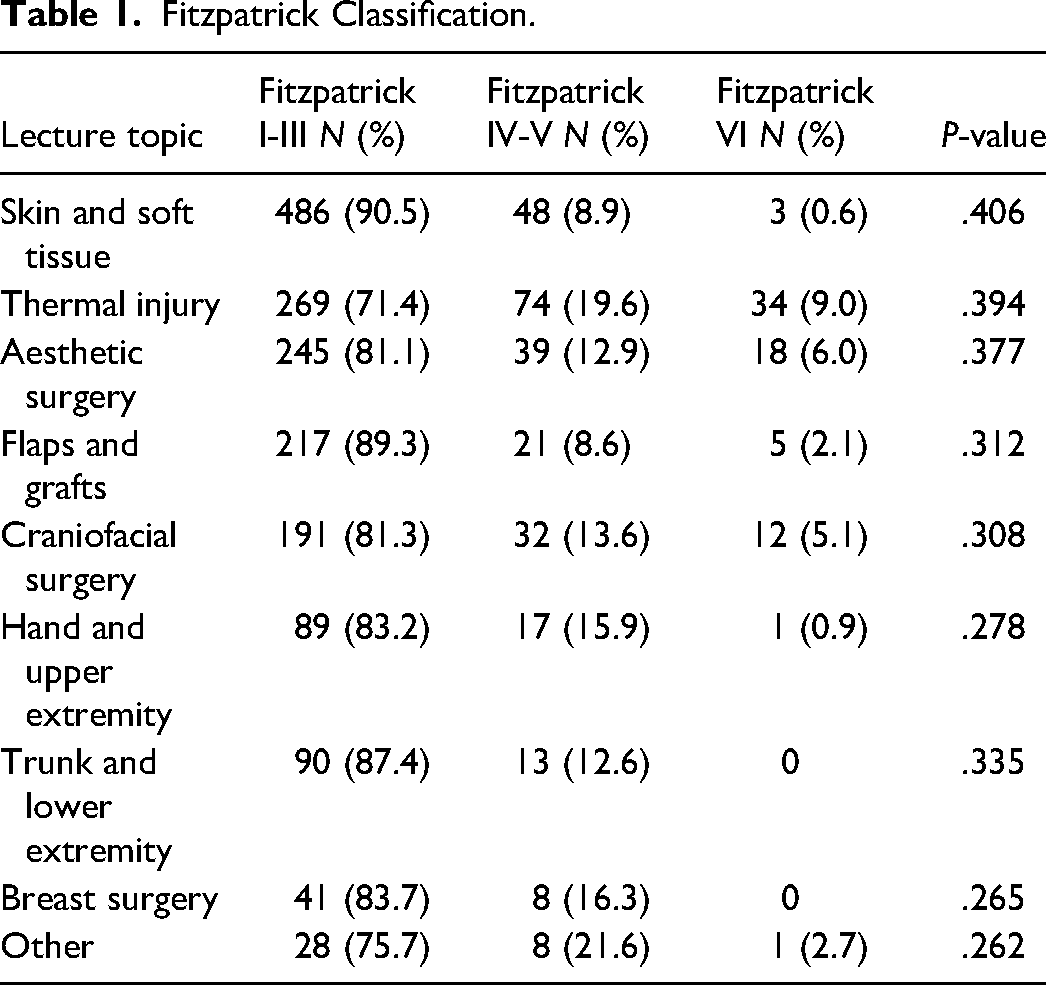
The lecture topics with the greatest proportion of Fitzpatrick IV to VI images included: thermal injury (28.6%), aesthetic surgery (18.9%), and craniofacial surgery (18.7%) (Table 1). Lecture topics with the greatest proportion of Fitzpatrick Type I to III images included: skin and soft tissue (90.5%), flaps and grafts (89.3%), and trunk and lower extremity (87.4%). There was no statistically significant difference between the proportion of Fitzpatrick I to III, IV to I, or VI images in these lectures compared to the aggregate sample (see Table 1). Further exploration of the significance of these findings is outlined in the discussion below.
Fitzpatrick Classification.
Survey Results
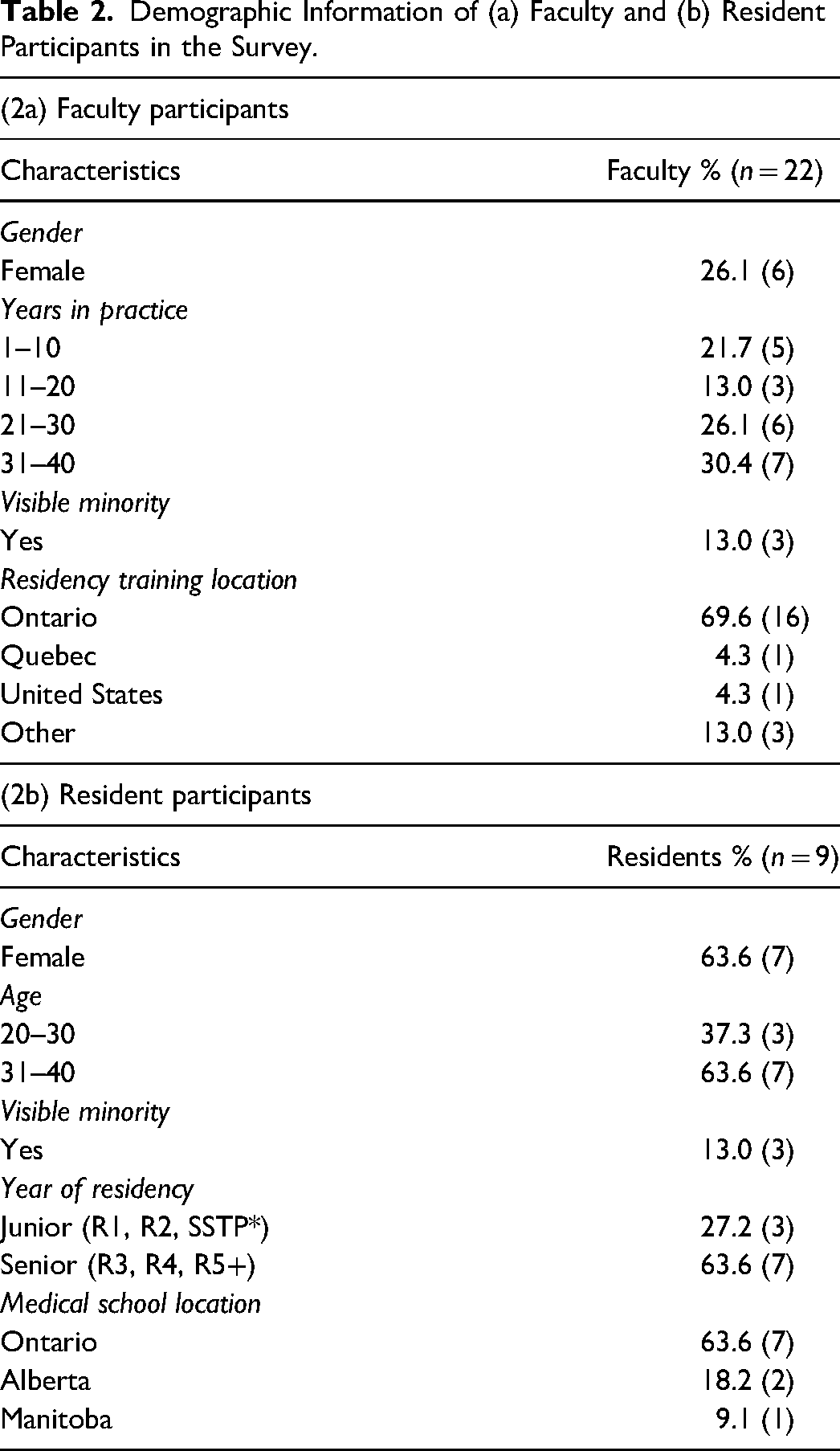
The survey was completed by 22 (22%) faculty members and 9 (35%) residents. The faculty survey was completed by 26% (n = 6) of female faculty and 13% (n = 3) of individuals that identify as a visible ethnic minority. Among residents completing the survey, 64% (n = 7) identified as female, and 36% (n = 4) identified as a visible minority. (Table 2). Sixty-one percent (n = 14) of faculty respondents believe they include diversity in their photographs that represent the population of their clinical practice, however, 46% (n = 5) of resident respondents would like to see more diversity in lecturers’ photographs. Residents do believe that it is difficult for lecturers to find photographs of patients with darker skin tones (64%, n = 7). Resident belief that there should be more opportunities to learn about EDI was significantly higher than faculty (P < .01). Finally, the majority of both residents and faculty (respectively 82%, n = 9; 61%, n = 14), believe that there is a commitment to provide more opportunities for EDI initiatives. There was no significant difference between faculty and resident beliefs that there is a commitment to provide more opportunities for EDI initiatives.
Demographic Information of (a) Faculty and (b) Resident Participants in the Survey.
Discussion
To our knowledge, this study is the first assessment of skin tone diversity in Canadian institution's postgraduate plastic surgery curriculum. This study found that white skin tones (Fitzpatrick I-III) were disproportionally overrepresented compared to darker skin tones (Fitzpatrick IV-VI). The methodology and findings are in keeping with the literature regarding diversity in plastic surgery educational material. A recent review by Smith et al. of the American Society of Plastic Surgeons Education Network Plastic Surgery Curriculum was conducted to assess the Fitzpatrick classification of all photographs within their teaching chapters. 24 Most images (81.6%) were classified as lighter tones (Fitzpatrick I-II), and only 6.6% of images were of dark skin as represented by Fitzpatrick V-VI. Additionally, only 0.6% of graphics or illustrations were Fitzpatrick V to VI. 24 Images in major North American and European journals regarding breast reconstruction and aesthetic surgery demonstrate predominantly white skin. 25 A notable exception is reporting of blepharoplasty, a procedure that is popular in Asian populations. 26 Finally, a study of social media platforms used to demonstrate surgical procedures for patient education concluded that there was a predominance of white skin (88.1%) in both reconstructive and aesthetic surgery images. 27
While an imperfect proxy, skin tone is one aspect of representation of racial and ethnic diversity, particularly within an educational field which is highly visual in nature. The study findings indicate that the photographic representation of patients in educational material does not necessarily represent the ethnic and racial diversity in the Greater Toronto Area. In 2016, 52% of Toronto's population identified as belonging to a visible minority group, whereas an average of 16.7% of images used in educational materials were representative of darker skin tones (Fitzpatrick types IV-VI). Increased diversity among skin tones seen in educational imaging is essential to develop a better proportional representation of patient populations. This in turn can act as a protective factor in preventing advanced disease and delayed diagnosis. 7
In our study, we observed a comparatively lower number of Fitzpatrick types I to III photographs in aesthetic surgery lectures, although this was not statistically significant when compared across lectures. This finding may align with previous studies that suggest increasing proportions of non-Caucasian patients undergoing cosmetic surgery.26,28 One study found non-Caucasian aesthetic patients in the United States grew from 23% in 2005% to 34% in 2020, and there are certain procedures (eg, blepharoplasty) which are predominantly performed in Asian populations. 26 Some literature exists of surgeons tailoring procedures, such as rhinoplasties and buttock contouring, to address cultural norms of non-Caucasian populations and non-Western societies.29,30 However, although this landscape is changing, the majority (66%) of cosmetic surgery patients remain Caucasian. 28 This disparity may contribute to decreased skin tone diversity in photographic representation for cosmetic procedures, which further leads to lower proportions of non-Caucasian patients seeking aesthetic surgery as images may not be reflective of diverse populations.
Our study also demonstrates that perceptions of skin tone diversity differ between residents and faculty. While residents believe there needs to be more photographic variety across the Fitzpatrick scale, faculty members believe there is enough inclusion of diverse photographs in their teaching material. Interestingly, there is no statistical difference in the belief that there is a commitment to provide more EDI opportunities within the curriculum. These findings suggest that both residents and faculty believe that EDI-informed educational reform is an ongoing area of improvement which may include increasing skin tone diversity among educational images. It is important to note that this research was conducted with the support of the faculty at our institution's Division of Plastic, Reconstructive, and Aesthetic Surgery. A key step in improving diversity and equity is prioritizing inclusive research and educational initiatives. Leadership support is key to the growth of any actionable initiative, particularly when there is limited literature highlighting formalized EDI education initiatives in plastic surgery.31,32
There are several limitations of this work. First, this study is a single-institution observational study with a limited time frame, and further work is required to investigate trends at other centers. As the Division moves to integrate EDI teaching into its curriculum, 32 we sought to examine lectures before full integration had taken place. While the study was limited to one site, this factor enabled our analysis to be more standardized and of higher quality. In a follow-up investigation, a multi-institutional study could be beneficial to understand how different curricula incorporate skin-tone diversity. Second, the evaluation of images is inherently dependent on the reviewers and is subject to reporter bias and one's interpretation of an image and its Fitzpatrick classification. Fortunately, our evaluation of interrater reliability showed almost perfect agreement across raters. The Fitzpatrick classification's initial intended use was for the evaluation of ultraviolet light exposure and damage, not skin tone diversity. 18 While it can serve as a reference range for skin-tone diversity, this does not always accurately correspond to one's self-reported race or ethnicity. 33 It is therefore not an optimal measure of race as it cannot perfectly identify white skin tones versus skin tones of some visible ethnic minorities. However, it appears to be the current standard in the literature to assess diversity in medical imaging, and its use as a proxy remains useful while we await the development of new assessment tools. 34 Along similar lines, it is possible that images may be distorted by photography settings and lighting differences, especially under operating room lighting. This may change the interpretation of skin tone by either lightening or darkening the appearance of the skin. Furthermore, only images were extracted from lectures, therefore it is possible the lack of additional context may omit discussions during lectures which promote EDI within the curricular content. Lastly, although the lectures were delivered between 2020 and 2021, it is possible that there is outdated content in the lectures which may not reflect the current Fitzpatrick representation of patients. However, our institution attempts to mitigate this by delivering lectures in cycles which are updated every 3 years by residents and faculty. In terms of the survey, nonresponse bias is also a possible limitation given unaccountable differences that may exist between those residents and faculty that completed the survey versus those that did not. Lastly, it is also important to note that while we discuss skin tone, race, and ethnicity in the context of diversity, they are not interchangeable. Race speaks to shared physical traits, such as skin tone, whereas ethnicity is indicative of shared cultural traditions, beliefs, and language. 35
Inequities in care on the basis of race, or racialized appearance, continue to be prevalent in the Canadian healthcare system.36,37 Recently, a call to action by Snell et al encouraged Canadian Plastic, Reconstructive, and Aesthetic colleagues to evaluate their programs in three domains: education, disparities in clinical settings and policies, and leadership. 32 Within the education domain, consciously curating an inclusive setting was suggested to attract the strongest future surgeons. Our study describes skin tone representation in the plastic surgery curriculum in one of Canada's most diverse, urban centers. We also present an opportunity to address gaps in visual representation by encouraging educators to diversify the images they include in their teaching. Such a change can be effectively accomplished by making small, intentional changes in lecture/seminar images by reflecting on current images and purposefully including a wider range of diverse images. 38 Using established resources, such as “Mind the Gap” or “visualDx,” when there is difficulty obtaining one's own case images may be of additional benefit.16,39 Future studies may analyze skin tone diversity educational image inclusion across multiple institutions and surgical programs (ie, across national plastic surgery programs and departments of surgery) and examine differences in measured skin tone image diversity after the implementation of EDI principles into education curricula. We also hope to explore perceptions of the current curricula, unpack explicit or implicit biases, and better understand efforts being made to improve racial and ethnic diversity within the curriculum.
Conclusion
This study highlights an underrepresentation of darker skin tones displayed in a Canadian plastic surgery resident education curriculum. Resident training is critical in the formation of future practicing plastic surgeons and providing a curriculum that represents a diverse population provides residents with a better understanding of their patients and how the same conditions may present on different skin tones. Integrating a curriculum that acknowledges EDI and implements it in training can help develop culturally competent surgeons who provide better care.
Supplemental Material
sj-docx-1-psg-10.1177_22925503231195023 - Supplemental material for Exploring Skin Tone Diversity in a Plastic Surgery Resident Education Curriculum
Supplemental material, sj-docx-1-psg-10.1177_22925503231195023 for Exploring Skin Tone Diversity in a Plastic Surgery Resident Education Curriculum by Jane Zhu, Raahulan Rathagirishnan, Chantal Valiquette, Alexander Adibfar and Laura Snell in Plastic Surgery
Footnotes
Author Contributions
CV and LS contributed to the conceptualization of the study. All authors contributed to the design of the study and the creation of the survey instrument. JZ and RR performed indexing of the photographs included. CV, AA, JZ, and RR independently recorded the classification of photographic images. RR and JZ performed data analysis and drafted the manuscript. All authors revised the manuscript.
Previous Presentations and Publications
Presented at the Canadian Society of Plastic Surgeons (CSPS) 2022. Presented at Canadian Conference for Surgical Education (C-CASE) 2022 Meeting.
Research Ethics and Patient Consent
Research ethics approval was granted by Sunnybrook REB Information System (SunRISE) Project ID 5130.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.