
Abstract
Background
Breast Augmentation
Breast implants were first introduced in the 1960s and have long been used for reconstructive and cosmetic surgery.1–4 However, implant-based breast procedures carry risks of complications, including capsular contracture, breast animation, implant failure, breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), breast implant illness, and possible consequences to psychological well-being.4–6
Autologous fat grafting (AFG), otherwise known as fat transfer, lipoagumentation, liposculpture, or lipomodeling, is an alternative for breast augmentation and reconstruction.4,7 Since 2000, fat grafting accounted for a 29% increase in breast reconstruction and a 25% increase in cosmetic breast surgery. 1 This procedure is best suited to patients who want a moderate increase in their breast volume, typically seen in patients who underwent significant weight loss, post-pregnancy, or in reconstructive patients such as in post-mastectomy reconstructive surgery.
Patient-Reported Outcome Measures
In cosmetic and reconstructive patients, it is important to assess a patient's perception of their quality of life (QoL) to determine the impact on a patient's appearance, functional status, and mental health. 8 By assessing QoL in a valid, systematic, and reliable way, it can help influence future decision-making for patients and physicians. 9 However, when using the patient's perspective on their QoL and outcomes, it is subjected to many biases and can be heavily influenced by motivation, health, age, and socioeconomic status. 10
For the breast, there are three prominent patient-reported outcome measures (PROMs), and assessment strategies, including BREAST-Q, Breast Evaluation Questionnaire (BEQ), and Breast Reduction Assessed Severity Scale Questionnaire (BRASSQ). 11 BREAST-Q is currently the most well-validated breast-specific PROM instrument available, with the added benefit of having a pre-operative and post-operative components. 11
BREAST-Q
The BREAST-Q questionnaire was developed in 2009 and can be used for augmentation, reduction, and for reconstructive patients. It aims to investigate topics known as modules such as psychosocial, physical, sexual well-being, satisfaction of care, and satisfaction of breasts.8,9,12 BREAST-Q has since become the gold standard for assessing QoL and patient satisfaction for patients undergoing breast surgery. 12
This article aims to provide an updated review of the literature and PROMs for two common methods of breast augmentation surgeries. PROMs provide a valuable objective and standardized scale of patient satisfaction, and trends in this data can help surgeons identify areas of potential improvement. This systematic review and meta-analysis aimed to compare patients’ QoL outcomes using BREAST-Q to assess the satisfaction of patients who undergo fat grafting compared to implant-based primary breast augmentation.
Methods
Search Strategy
The methodology was then designed and registered in the PROSPERO database (CRD42022297860). The preferred reporting items for systematic reviews and meta-analysis (PRISMA) guideline was used (Figure 1). The search strategy included search terms related to primary breast augmentation, the two methods of interest, and terms related to the primary outcome, BREAST-Q.
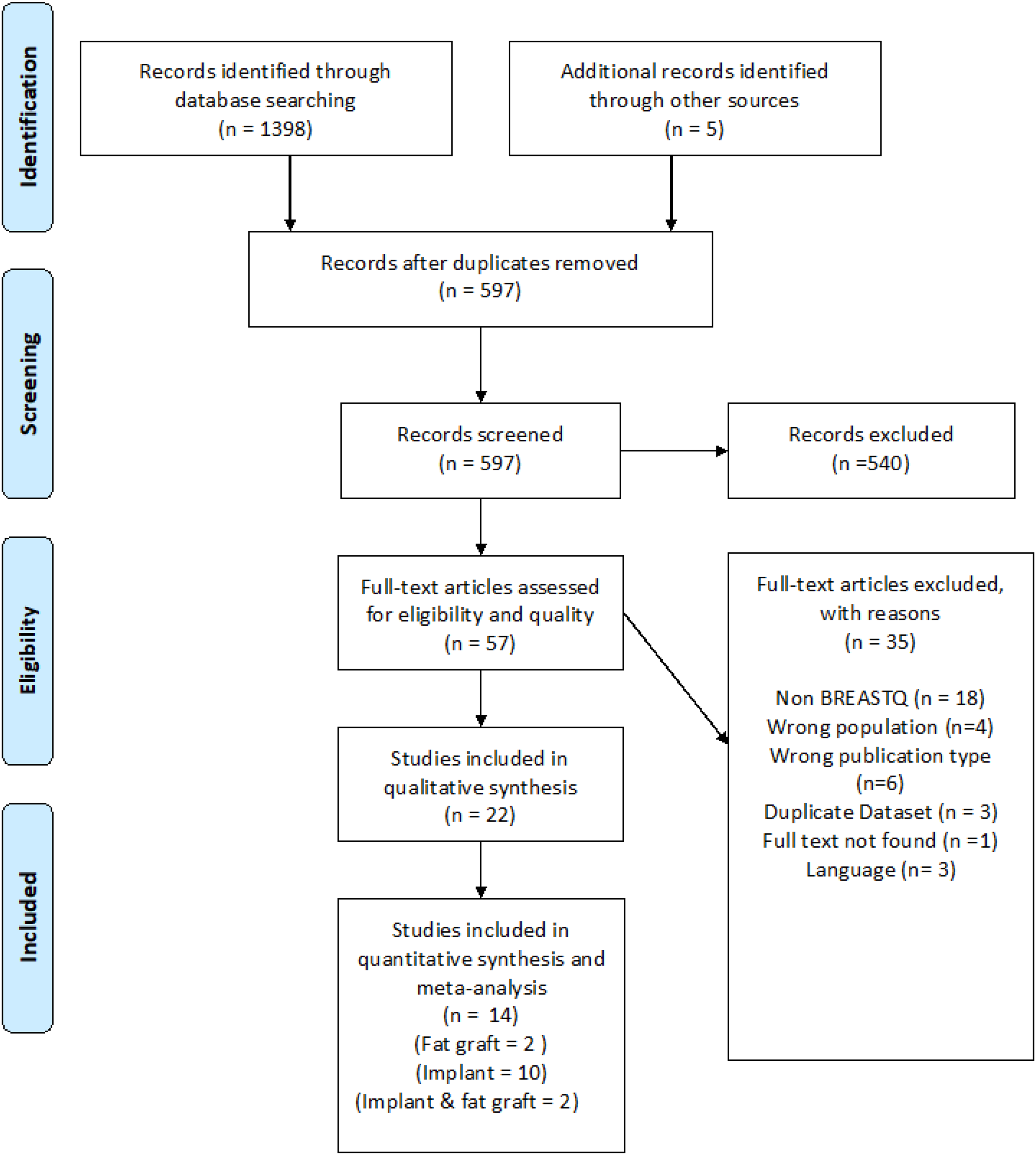
PRISMA diagram for records screened, and final papers included in data extraction and analysis.
Five bibliographic databases were searched on November 4, 2021: PubMed®, Cochrane Library®, EMBASE®, MEDLINE®, and Scopus®. References were manually screened from relevant review articles to identify if there were any studies that were not captured in the initial search. However, no additional sources were identified in this process.
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria were determined a priori. We included prospective studies, retrospective studies, and randomized controlled trials written in English or French and published in peer-reviewed journals over the past ten years from the date of the search. Only studies that included patients who underwent primary breast augmentation using either implants or fat grafting for aesthetic purposes were included. Studies reporting on augmentation with a combination of implant and fat grafting or breast reconstruction were excluded. Patients who have had a previous mastectomy, gender-affirming surgery, massive weight loss, or multiple fat grafting sessions were excluded due to the multifactorial nature of their cases. All studies must report, at minimum, post-operative BREAST-Q data as a study outcome to be included. Single case reports, reviews, animal studies, conference proceedings, abstracts, inaccessible manuscripts, and editorials were excluded.
Study Selection
Studies extracted were analyzed, and duplicates were eliminated and underwent screening by two independent reviewers using Rayyaan platform (Rayyaan Systems Inc., Cambridge, MA, USA). For the primary screen, titles and abstracts were reviewed. Selected articles underwent full-text review for the secondary screening. The principal investigator functioned as an independent arbitrator. The methodological index for non-randomized studies (MINORS) score was used to assess the quality of all articles selected for the review and meta-analysis. Papers that failed to achieve a benchmark score of 60% or higher were excluded.
Data Extraction
The two independent reviewers extracted data using the Google Sheet platform (Google, Mountain View, CA, USA). Study type, number of patients, average age, BMI, type of augmentation, augmentation characteristics, surgical technique, pre- and post-operative BREAST-Q data, and common complication rates were extracted. Attempts were made to contact the authors of any study with incomplete BREAST-Q data.
Statistical Analysis
Statistical and meta-analyses were conducted by a contracted statistician. Cohen's kappa coefficient was calculated to assess inter-rater reliability for article selection, with values 0.41-0.60, 0.61-0.80, and 0.81-1.00 representing moderate agreement, substantial agreement and perfect agreement, respectively. Studies that reported multiple patient groups using the same augmentation technique were pooled to create a single summary for that study.
Mean scores from the BREAST-Q instruments were meta-analyzed using random-effects models with the empirical Bayes between-study variance estimator. 13 As pre-operative scores were not consistently available, the primary outcome measure was the post-operative mean BREAST-Q score and whether the pooled average was different between breast augmentation methods, either using implants or fat grafting. Therefore, post-operative mean scores were stratified by the surgical method as the main factor of interest. Inferences about the differences in pooled subgroup means were performed using meta-regression. In addition, reported demographics in the pre-operative period (eg, age, BMI) were used to explore possible sources of heterogeneity by meta-regression.
Between-group heterogeneity was characterized using the random-effects heterogeneity parameter (τ²) and I2, which describe the absolute or relative degree of between-study heterogeneity. For the meta-regression models, the adjusted R2 statistic was used to assess the proportion of variance between studies, which could be attributed to the covariates. Publication bias was assessed by funnel plots, as well as Egger's regression test. Finally, Galbraith plots with the same random-effects model were assessed to examine between-study heterogeneity and identify potential outlier studies.
Bivariate meta-regression of scores were used to corroborate whether and to what extent were potential differences in pooled estimates of post-op scores between surgical methods confounded by the few available pre-operative scores. These models included the surgical method as the only factor and were fit using a random-effects model, a restricted maximum likelihood estimator. A conservative value of 0.2 was assumed for the within-study correlation between pre-op and post-op scores. All analyses were performed in Stata 17 (StataCorp LLC, College Station, TX, USA).
Results
Study Characteristics
The search strategy identified a total of 1398 articles, and an additional five were added from relevant reviews discovered in the search. After duplicates were removed, a total of 597 articles were screened using titles and abstracts. A total of 57 articles were selected for full-text review, and 22 fit the inclusion criteria and were deemed suitable by both reviewers and independent arbitrators for data extraction. The Cohen's Kappa scores were 0.87 for the primary screen and 0.88 for the secondary screen. All studies included received a MINORS score of 60% or higher. Of these 22 studies, 14 included data that could be pooled for a meta-analysis, including two fat grafting studies, 10 implant studies, and 2 studies that included data from both methods. The total number of patients included in this study was 1616, with 81 in the fat grafting group and 1535 in the implant group.
Post-Operative Satisfaction Score
Two small studies (Brault and Tenna) reported on both fat grafting and implant augmentation methods (Table 1). The mean satisfaction score for implants was 12.9 points greater than with fat grafting (95% CI: −0.6, 26.5, P = .061; Figure 2), with only moderate heterogeneity (Q = 2.68, P = .11).
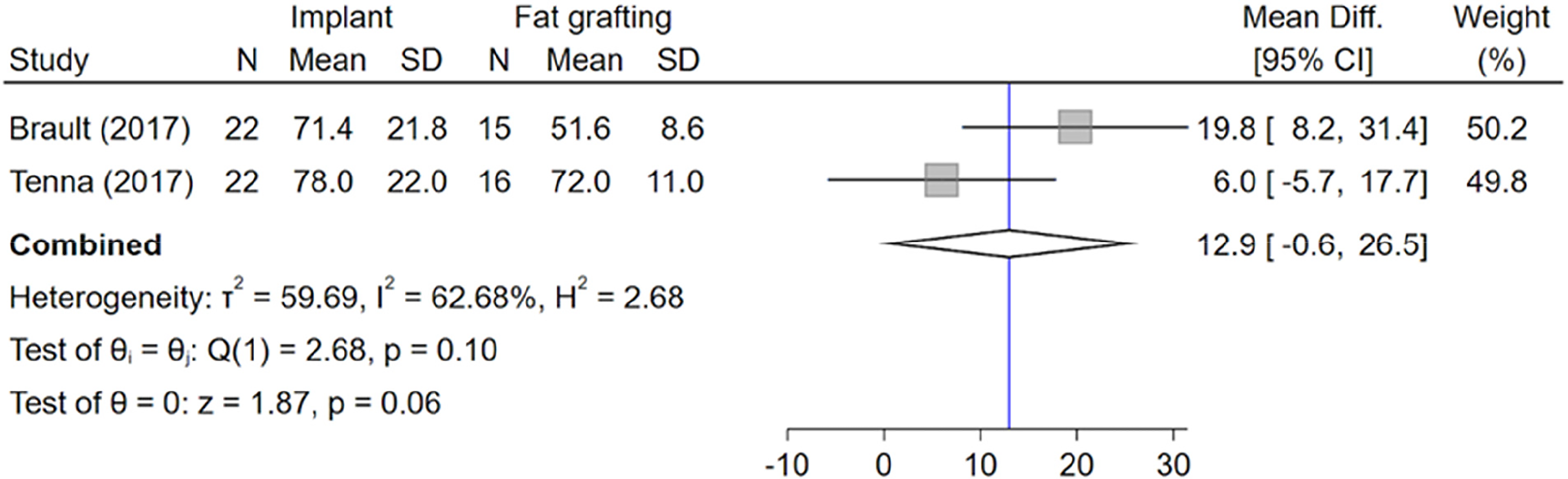
Forest plot of mean difference in post-op satisfaction score between augmentation methods.
Studies Comparing Satisfaction Scores for Both Augmentation Methods (N = 2).
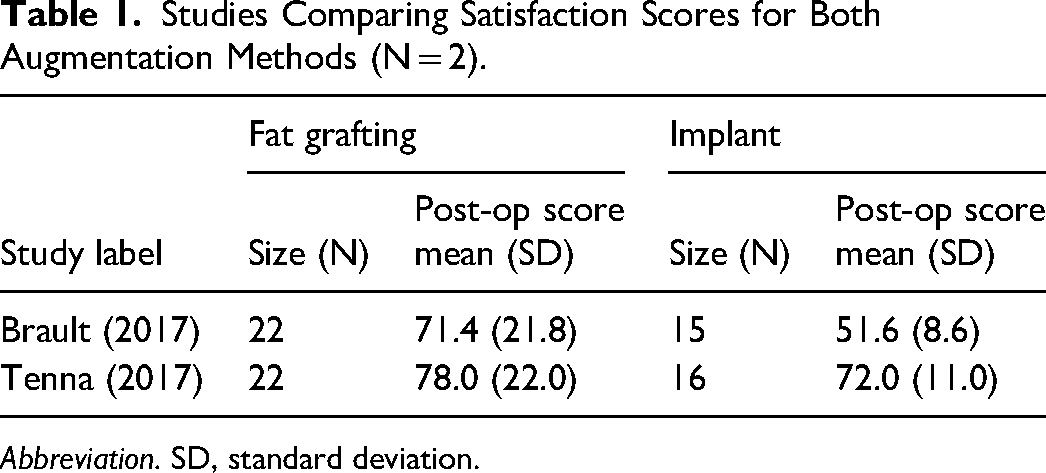
Abbreviation. SD, standard deviation.
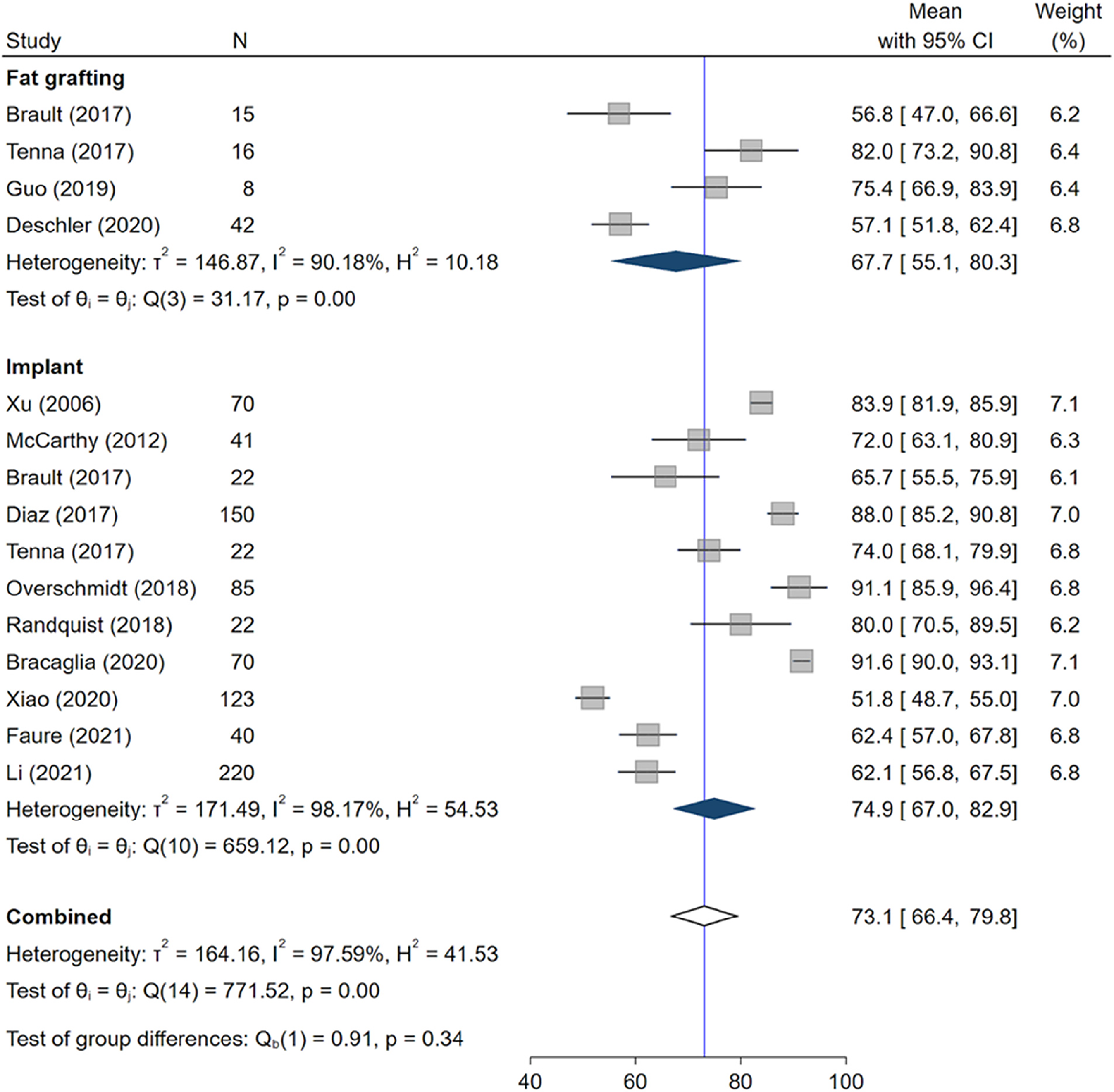
There were 14 studies that reported post-operative satisfaction scores and infrequently reported pre-operative scores (Table 2). Mean post-operative scores were pooled for each method of augmentation, and overall (Figure 3), there was no evidence of publication or small study bias, but the relative heterogeneity within augmentation groups was high.
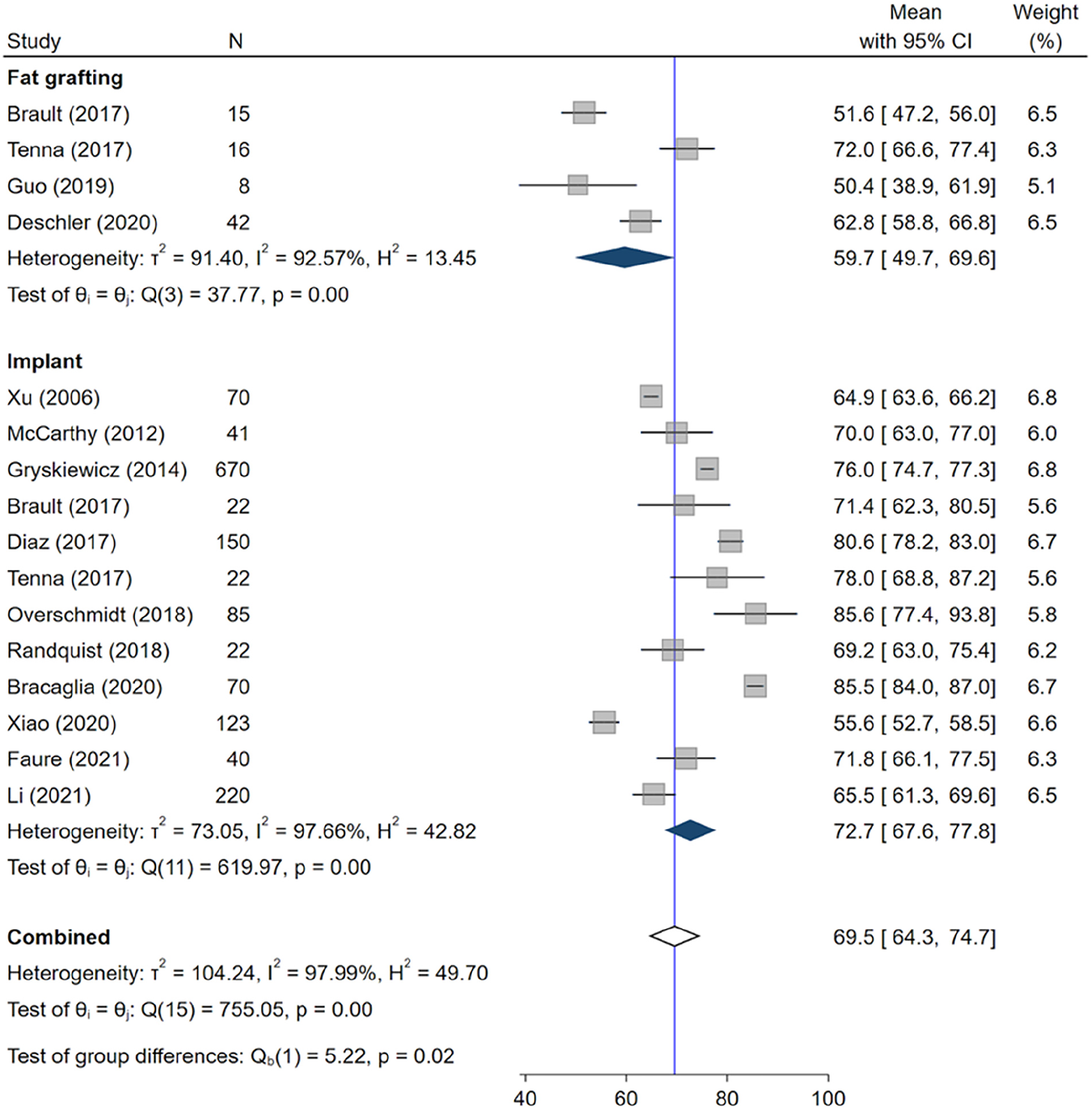
Forest plot of post-op satisfaction scores, stratified by augmentation method (raw mean).
Reported Pre-Op and Post-Op Satisfaction Scores (N = 14 Studies).
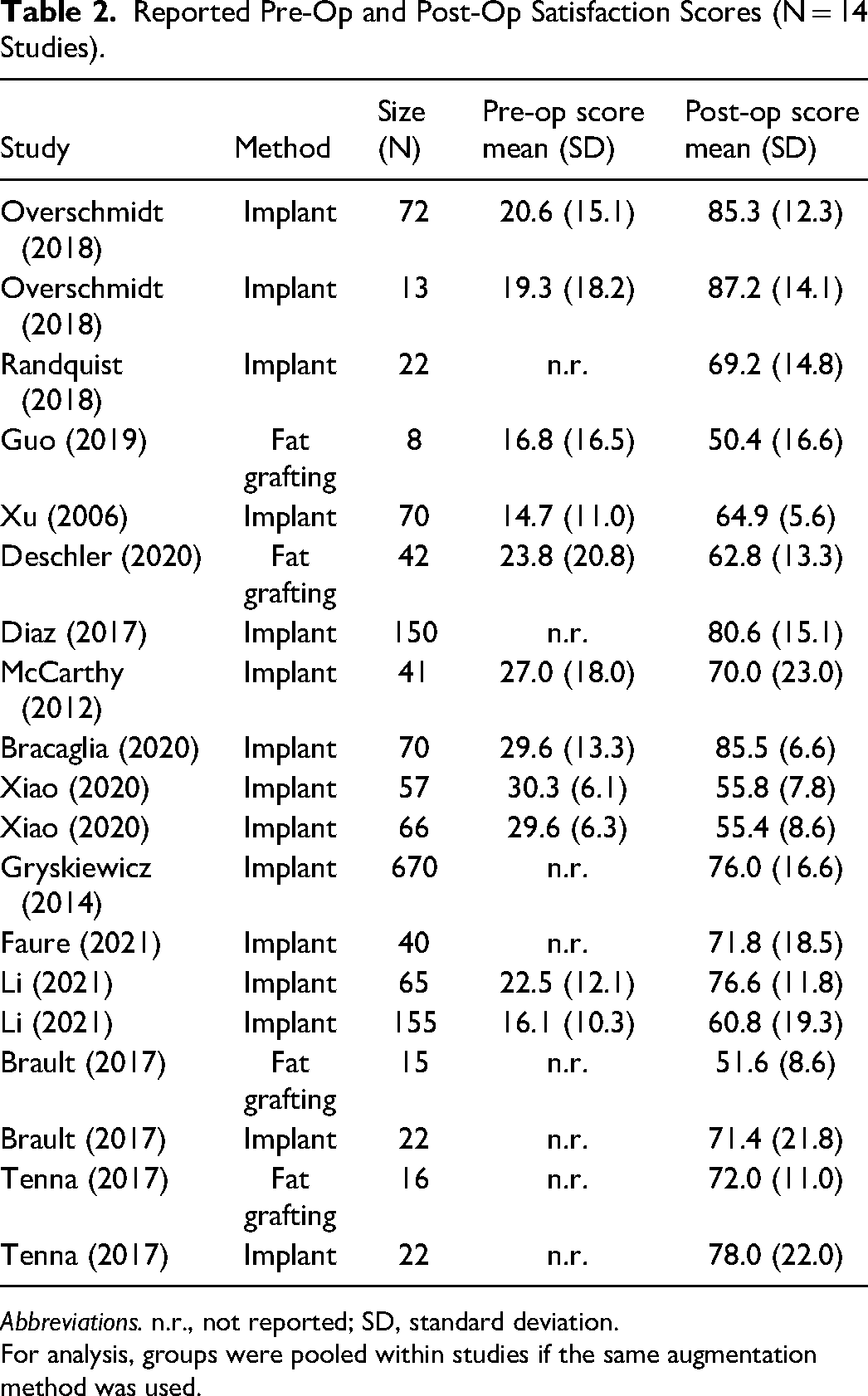
Abbreviations. n.r., not reported; SD, standard deviation.
For analysis, groups were pooled within studies if the same augmentation method was used.
The mean overall satisfaction score in the implant group was statistically greater than in the fat grafting group (Figure 3). Based on meta-regression, the estimated difference in mean post-op satisfaction scores is 13.0 (95% CI: 2.4-23.5; P = .016). The augmentation method explained 26.4% of observed variation.
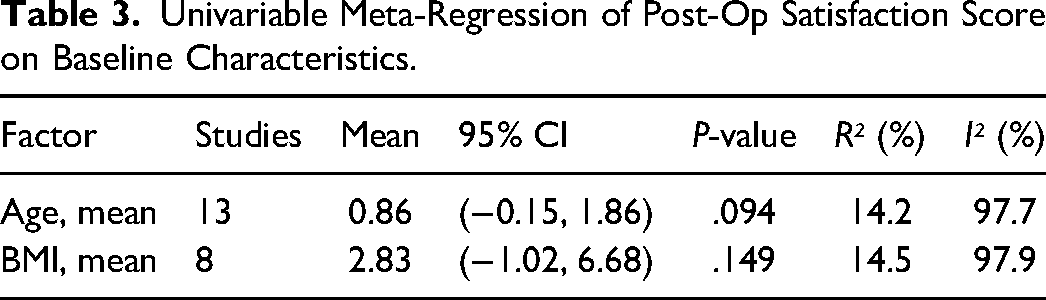
Table 3 shows a univariable meta-regression of post-operative satisfaction scores on mean post-op age and BMI. Despite some studies failing to report demographic details, both age and BMI were strongly associated with greater post-op satisfaction scores. Both factors explained about 20% of observed variation among the subset of reporting studies.
Univariable Meta-Regression of Post-Op Satisfaction Score on Baseline Characteristics.
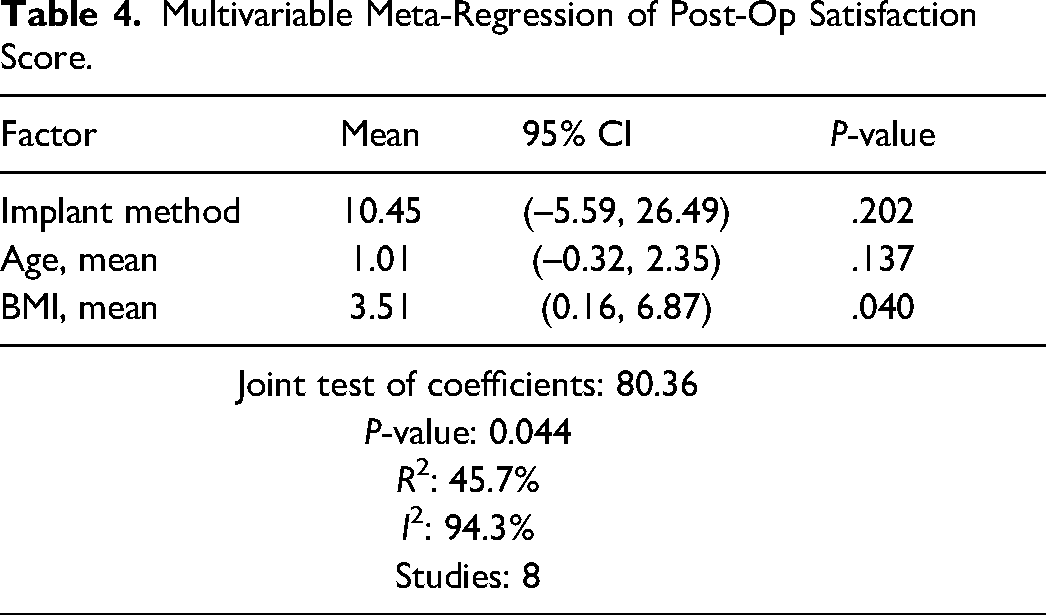
Meta-regression of post-operative scores on age, BMI and method substantially reduced the between-study heterogeneity parameter (τ²), reduced (I²), and increased the proportion of explained variance (R²). The implant method was still associated with a greater score than fat grafting after adjusting for age and BMI. Overall, these three factors appear to account for much of the between-study heterogeneity (Table 4).
Multivariable Meta-Regression of Post-Op Satisfaction Score.
To support the claim that differences in post-operative mean scores between methods are not confounded by pre-operative scores, a bivariate meta-regression was conducted to account for pre-op scores, using method as the only covariate. Using bivariate meta-regression, the mean change in the implant group was greater in magnitude but not statistically significant from the change in the fat grafting group 12.4 (95% CI: −4.9 to 29.6; P = .160). That this difference was similar in magnitude corroborates that pre-op scores did not differ between groups. Following bivariate meta-analysis, heterogeneity was reduced in post-op scores (I² = 74.4%).
Post-Operative Sexual Well-Being Score
Two small studies reported on both fat grafting and implant augmentation methods. The mean sexual well-being score was similar in both implant and fat grafting groups (difference = -0.4, 95% CI: −16.9, 16.0, P = .96), with moderate heterogeneity (Q = 3.41, P = .06).
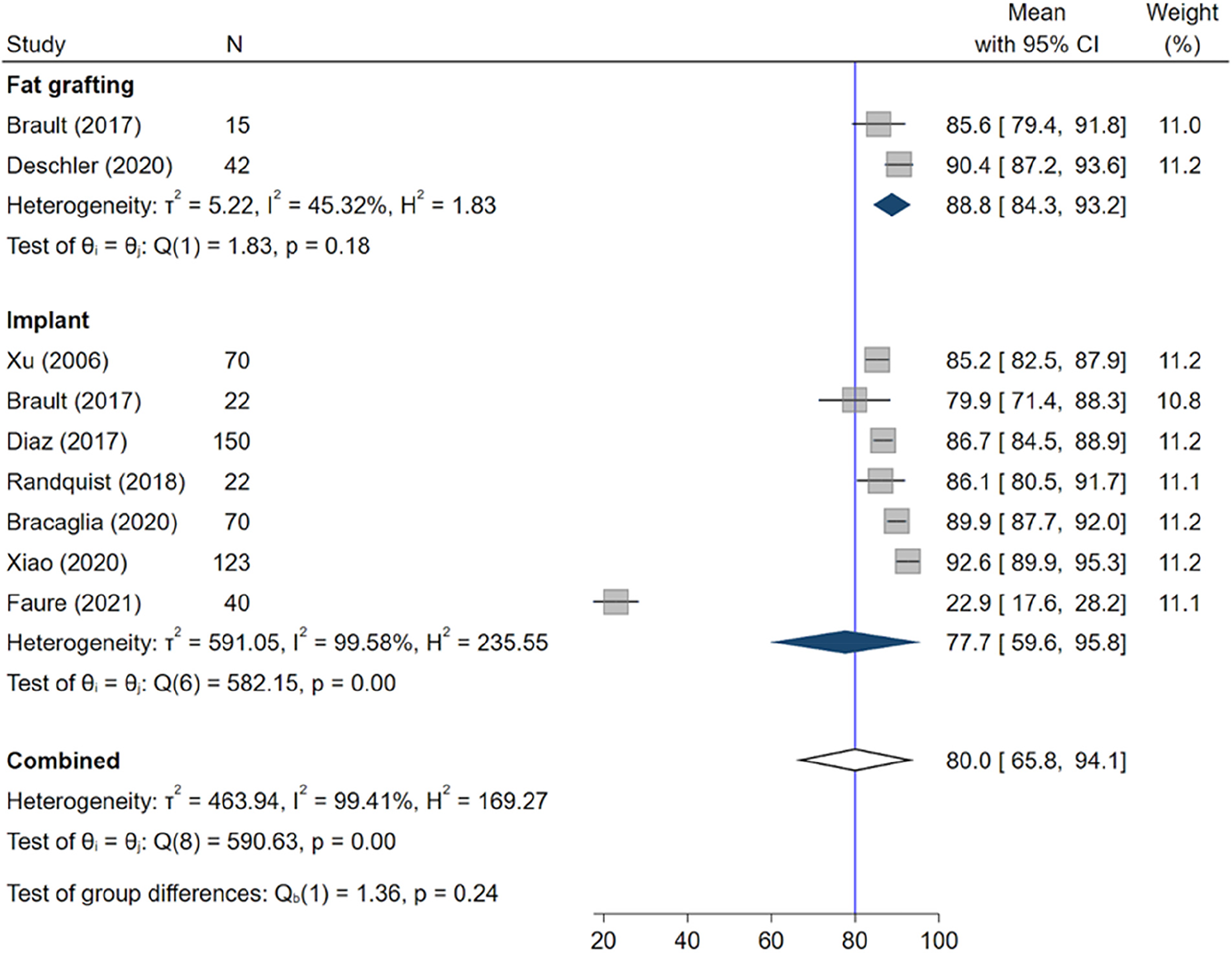
There were 13 studies that reported post-operative sexual well-being scores (Table 5). Mean post-op scores were pooled for each method of augmentation and overall (Figure 4). There was no evidence of publication or small study bias, but the relative heterogeneity within augmentation groups was high.
Forest plot of post-op sexual well-being scores, stratified by augmentation method (raw mean).
Reported Pre-Op and Post-Op Sexual Well-Being Scores (N = 13 Studies).
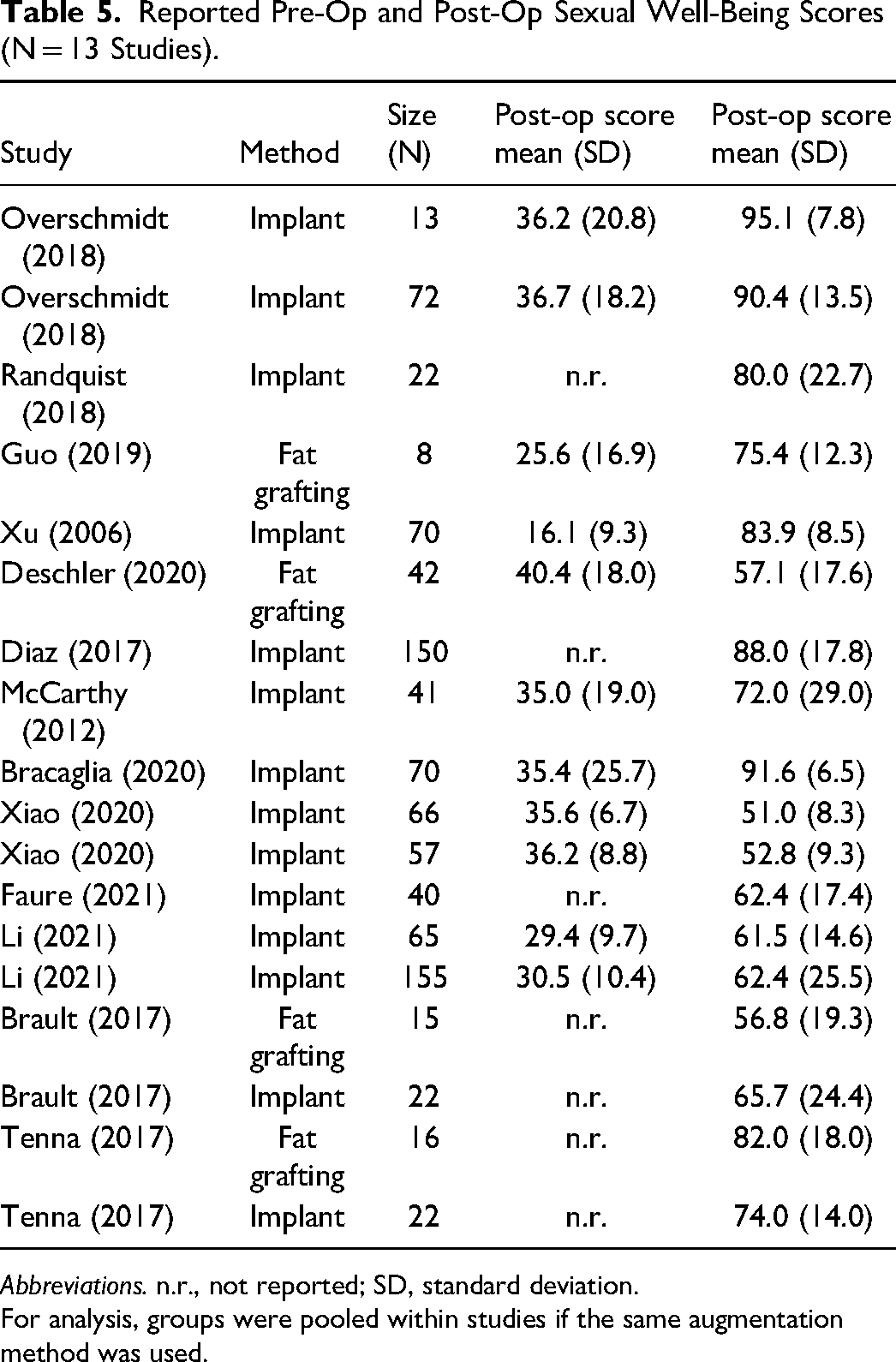
Abbreviations. n.r., not reported; SD, standard deviation.
For analysis, groups were pooled within studies if the same augmentation method was used.
Post-Operative Psychosocial Well-Being Score
Two small studies reported on both fat grafting and implant augmentation methods. The mean sexual well-being score was similar in both implant and fat grafting groups (difference = -2.8, 95% CI: −3.1, 8.6, P = .35), with no heterogeneity (Q = 0.96, P = .33).
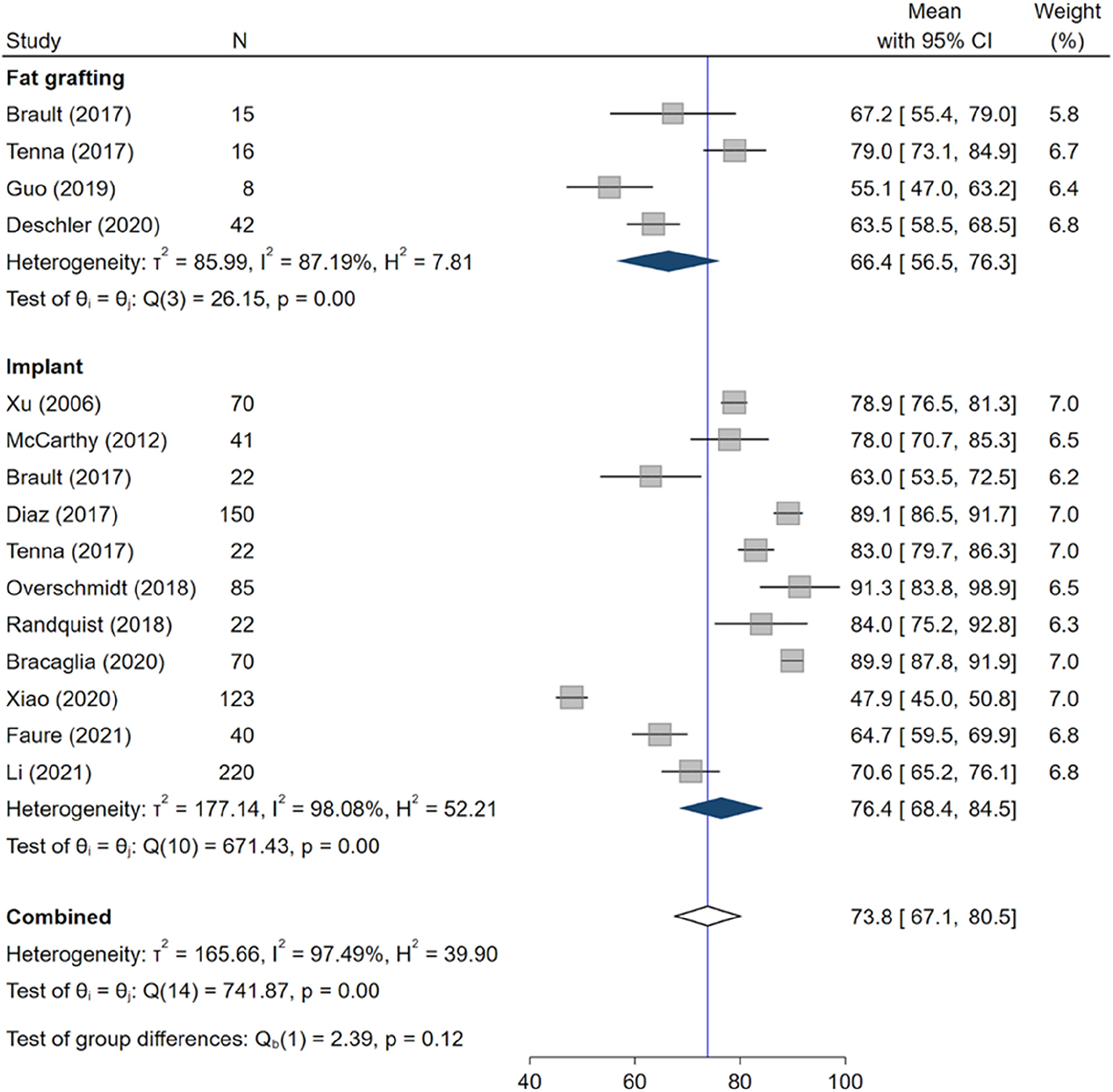
There were 13 studies that reported post-operative psychosocial well-being scores that could be pooled (Table 6). Mean post-operative scores were pooled for each method of augmentation and overall (Figure 5).
Forest plot of post-op psychosocial well-being scores, stratified by augmentation method (raw mean).
Reported Pre-Op and Post-Op Psychosocial Well-Being Scores (N = 13 Studies).
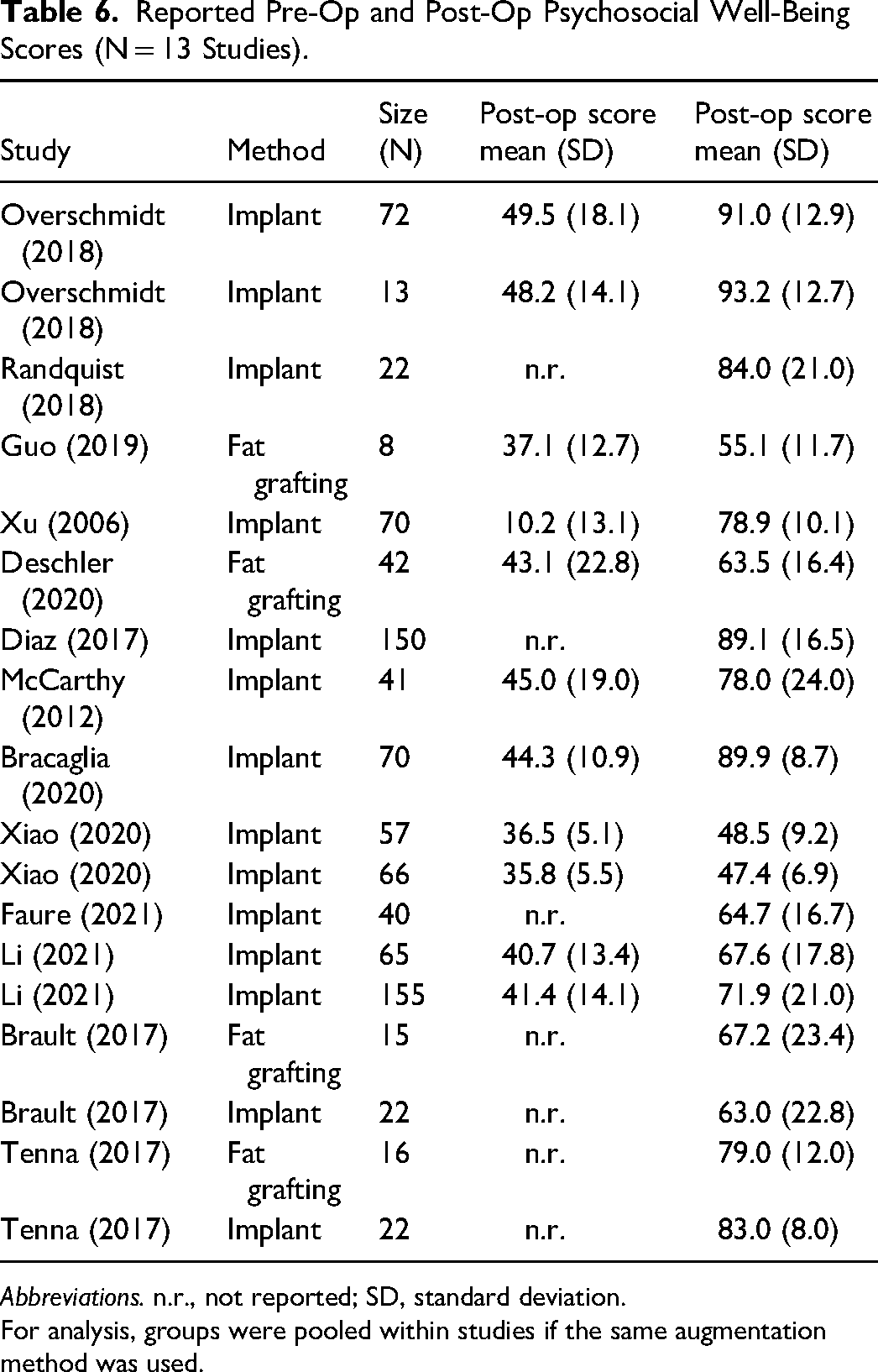
Abbreviations. n.r., not reported; SD, standard deviation.
For analysis, groups were pooled within studies if the same augmentation method was used.
The pooled mean in the implant group showed no statistically significant difference than in the fat grafting group (Figure 5). Based on meta-regression, the estimated difference in mean post-operative psychosocial well-being scores is 10.1 (95% CI: −4.8 to 25.1; P = .184). The augmentation method explained 5.4% of observed variation. The study by Xiao et al (2020) is an apparent outlier based on a Galbraith plot. Excluding this study resulted in a more precise estimate of the difference between methods, in which the average implant group had a significantly higher score than fat grafting by 13.1 (95% CI: 1.2-25.1; P = 0.031). The variation explained by the method also increased to 24.1%.
Despite some studies failing to report demographic details, a greater age and BMI were strongly associated with higher post-operative psychosocial well-being scores. Both factors explained about 20% of observed variation among the subset of reporting studies.
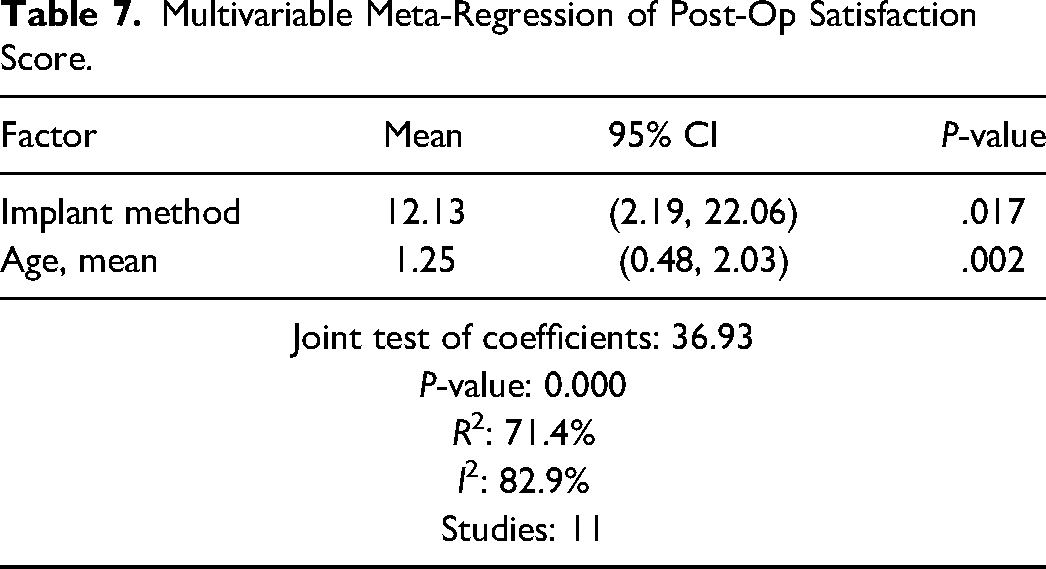
Meta-regression of post-operative scores on age and method substantially reduced the between-study heterogeneity parameter (τ²), reduced (I²), and increased the proportion of explained variance (R²). BMI was not associated with post-op score in univariate regression and was not included in this model. The implant method is still associated with a greater score than fat grafting after adjusting for age and excluding the single outlier study by Xiao (2020) (Table 7).
Multivariable Meta-Regression of Post-Op Satisfaction Score.
Post-Operative Physical Well-Being Score
No studies provided a direct comparison of the physical well-being scores. There were 8 studies that reported post-operative sexual well-being scores that could be pooled (Table 8). Mean post-op scores were pooled for each method of augmentation and overall (Figure 6).
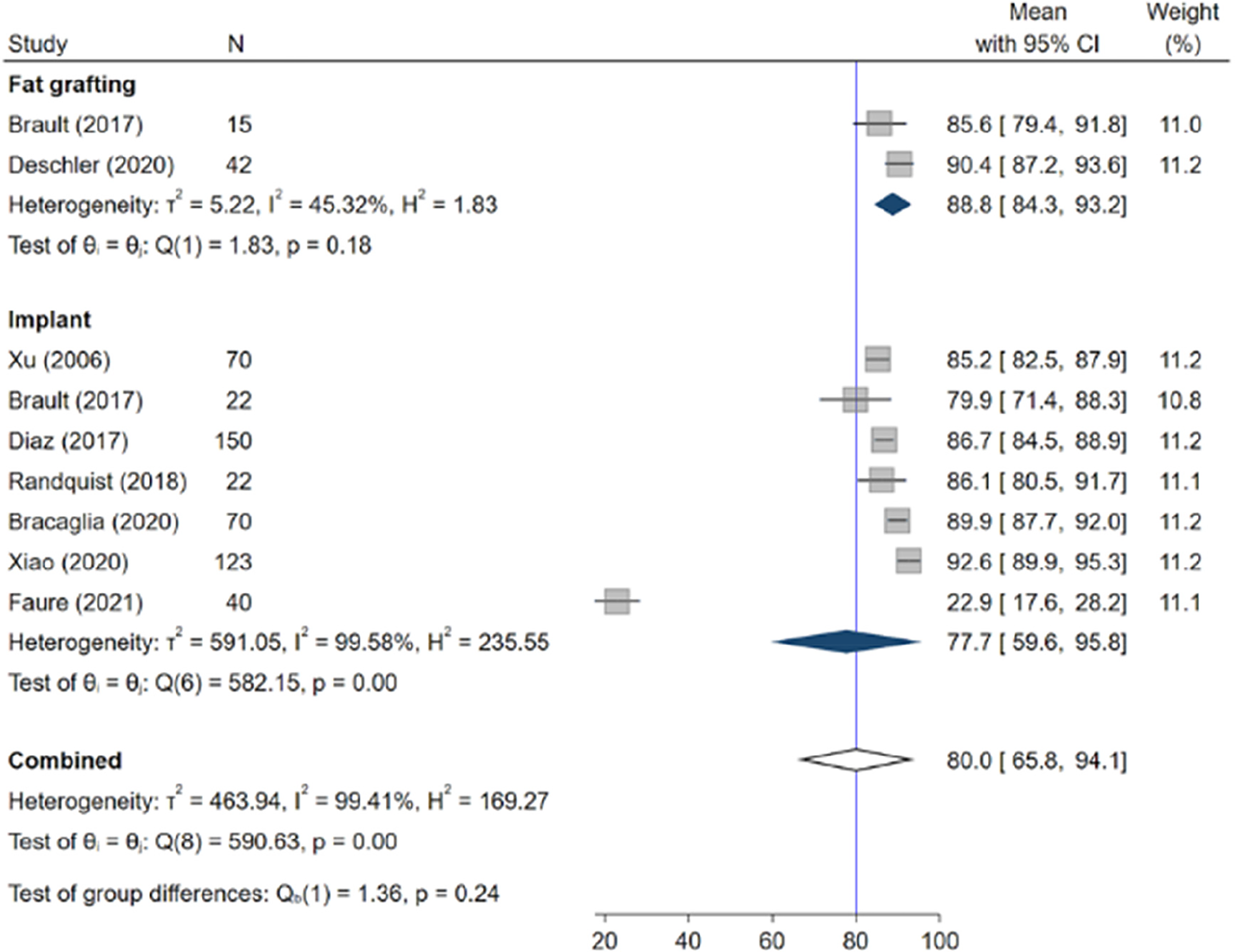
Forest plot of post-op physical well-being scores, stratified by augmentation method (raw mean).
Reported Pre-Op and Post-Op Physical Well-Being Scores (N = 8 Studies).
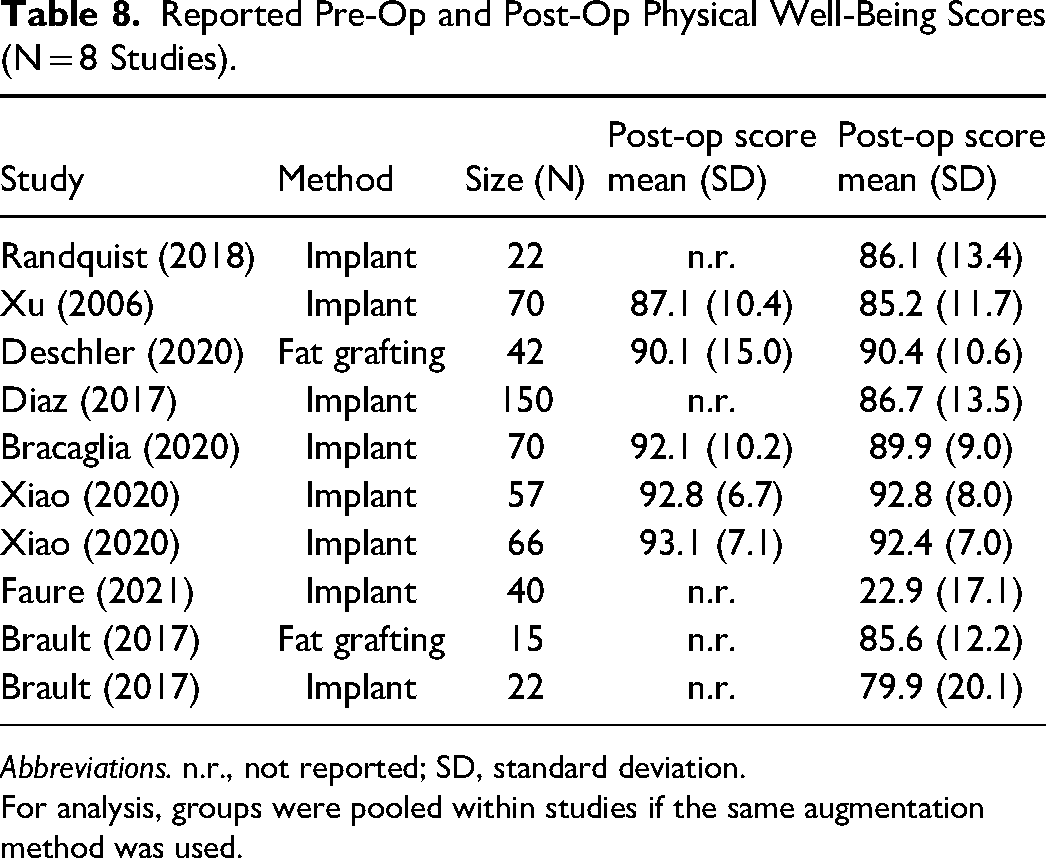
Abbreviations. n.r., not reported; SD, standard deviation.
For analysis, groups were pooled within studies if the same augmentation method was used.
The pooled mean in the implant group showed no statistically significant difference compared to the fat grafting group (Figure 6). Based on meta-regression, the estimated difference in mean post-op physical well-being scores is −10.4 (95% CI: −46.0 to 25.3; P = .569).
The study by Faure et al (2021) was identified as an outlier based on Galbraith and funnel plots. Excluding this study resulted in making estimates of mean scores in each augmentation group more similar, with a difference in means of −1.0 (95% CI: −7.2 to 5.3; P = .762) (Figures 7 and 8).
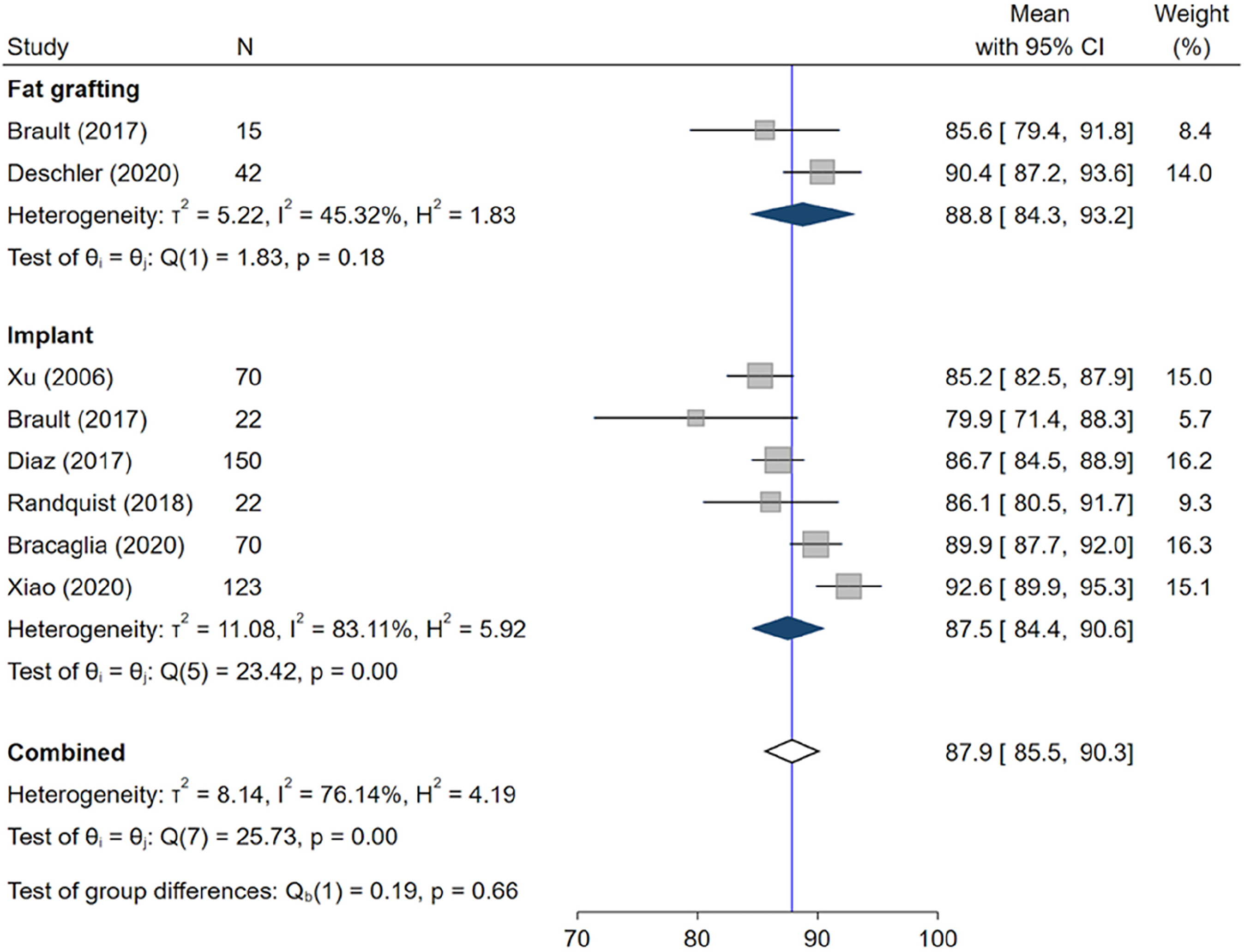
Forest plot of post-op physical well-being scores, stratified by augmentation method (raw mean), excluding outlier.
Forest plot of post-op physical well-being scores, stratified by augmentation method excluding outlier.
Discussion
BREAST-Q is a validated tool that can be used to evaluate patient-reported QoL in post-operative breast augmentation patients. 13 This meta-analysis investigated the QoL using BREAST-Q in patients who underwent primary breast augmentation with either fat grafting or breast implants. To our knowledge, there has been no other study that compared breast augmentation using exclusively breast implants or exclusively fat grafting for cosmetic breast augmentation.
Overall, the results demonstrated that patients who received implant-based breast augmentation reported a higher overall satisfaction scores than those who received fat grafting. The results show no difference among both groups in terms of sexual well-being, physical well-being, and psychosocial well-being scores in the BREAST-Q modules. Implant-based augmentation is one of the most common cosmetic procedures, and surgeons have developed standardized methods to give an overall more reliable and predictable result in the size and shape of the breasts, which could possibly explain increased patient satisfaction. 14 In comparison, fat grafting is a newer procedure that lacks standardized surgical methods. The major limitation of fat grafting is the limited volume increase that can be reliably achieved and the degree of fat resorption, which can be up to 60% of fat injected. 15 More long-term follow-up studies are needed to determine the satisfaction of patients over their lifetime post-augmentation.
In this study, there were two major outliers. One implant study reported lower physical well-being scores; this is likely because it was a tuberous breast study. 16 A possible explanation is that patients who undergo breast augmentation with tuberous breasts sometimes require several surgical procedures during their primary procedure and often suffer from more severe post-operative symptoms, including bruising and swelling, which may impact the patient's QoL. 17 The second outlier was in the psychosocial well-being scores with a study from the implant group. 18 This study was conducted in China and may demonstrate cultural differences in what different groups define as psychosocial well-being. BREAST-Q was originally written in English with standardized questions and has since been translated into many languages. This study, as an outlier, may be more reflective of the need to not only ensure adequate translation of the modules but also to ensure that the modules are adapted to account for cultural differences when being disseminated to patients outside of North America.
In the context of the current practice, most breast augmentation is implant-based augmentation, which explains why more studies are focused on breast implants. 6 Worldwide, there is also significant variability in terms of surgical techniques and types and shapes of implants used, leading to a lack of standardization when using studies from around the world. 19
In the future, it would be beneficial to investigate other ways to improve fat grafting techniques and improve outcomes for fat grafting patients. Additionally, larger studies comparing breast implant patients to fat grafting patients with matched cohort data would help draw more accurate conclusions on the true difference in QoL outcomes between the two groups.
Limitations
There was a lack of randomized control studies, likely due to the challenges with ethical and logistical concerns of patients receiving cosmetic breast augmentation. 20 Although this study aims to assess patient satisfaction with a similar goal, breast augmentation, the two surgical methods are incredibly different with different patient expectations and goals. The much smaller patient population in the fat grafting group was a major obstacle in this review. It is important to note that at baseline, patients who opt for breast augmentation with breast implants versus fat grafting are different. Patients who choose to have fat grafting accept a risk of unpredictable volume increase but allow for a subtle and natural augmentation, while those who chose breast implants are choosing a predictable volume increase. Therefore, depending on the information provided to the patients preoperatively, it could affect their expectations and, thus, some of their post-operative BREAST-Q scores. BREAST-Q is non-specific to breast augmentation; however, the data still represents deficiencies in fat grafting that need to be addressed. There was also not enough pre-operative data to measure the change in BREAST-Q scores across both groups accurately.
Furthermore, the time between surgery and the final BREAST-Q score typically ranged from 3 to 12 months postoperatively. Studies that reported early BREAST-Q scores may not represent the final results and post-operative satisfaction, particularly for the fat grafting group.
Conclusion
Overall, our study represents the first meta-analysis using BREAST-Q scores to compare patient satisfaction with implant versus fat grafting techniques for primary breast augmentation. We found that there was a mean 13-point higher mean satisfaction score in the implant group, although there was no statistically significant difference in the other QoL parameters evaluated by the BREAST-Q score. More research using standardized methodology and longer-term follow-up is needed to further characterize patient satisfaction with the augmentation method. However, currently, our review suggests that those who undergo implant augmentation are ‘happier’ with their results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
In accordance with ethical standards, ethical approval was not required for this review.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.