
Abstract
Allergic contact dermatitis (ACD) is a delayed-type hypersensitivity reaction that presents as a pruritic eczematous rash occurring 24 to 48 h after allergen exposure. It is a surgical complication that can impact people's quality of life after plastic surgeries. A 44-year-old female with right breast cancer presented with three recurrent episodes of severe pruritic cutaneous eczematous eruption over her right breast extending down to her trunk and vulva each time soon after her multiple breast surgeries. She was labeled as having allergies to several intravenous antibiotics received perioperatively. She was then patch tested with a positive reaction to bacitracin, a component of a modified double antibiotic solution used for pocket irrigation intraoperatively. It highlights the need for plastic surgeons to consider ACD to bacitracin in patients with dermatitis soon after having bacitracin for pocket irrigation or implant soaking during breast surgeries. Comprehensive patch testing can delineate the cause of surgery-related ACD.
Allergic contact dermatitis (ACD) is a T-cell mediated delayed-type hypersensitivity reaction that presents as a pruritic eczematous rash occurring 24 to 48 h at the site of exposure to the causative allergen. 1 Patients can develop secondary dermatitis (i.e., autoeczematization) at distant sites without exposure to the allergen. Medical products used during the surgery are possible allergens, including topical antibiotics, antiseptics, bandages, and tissue adhesives. 2
A 44-year-old female with prior right breast cancer presented to the emergency department with a pruritic eruption two days after her second right breast revision reconstruction with an exchange of implant for a tissue expander. One day after the surgery, she developed a red, pruritic rash that started over her right breast and then extended to her abdomen, back, and vulva the next day (Figure 1). She had a known allergy to amoxicillin (rash). She also reported two prior surgeries, including right mastectomy with immediate breast reconstruction with tissue expander followed by right breast second stage reconstruction. She had similar rashes one day after each surgery, which was attributed to possible allergies to perioperative cefazolin, clindamycin, and vancomycin. This time, she was treated with betamethasone valerate 0.1% ointment twice daily topically. The rash resolved over 1 month.
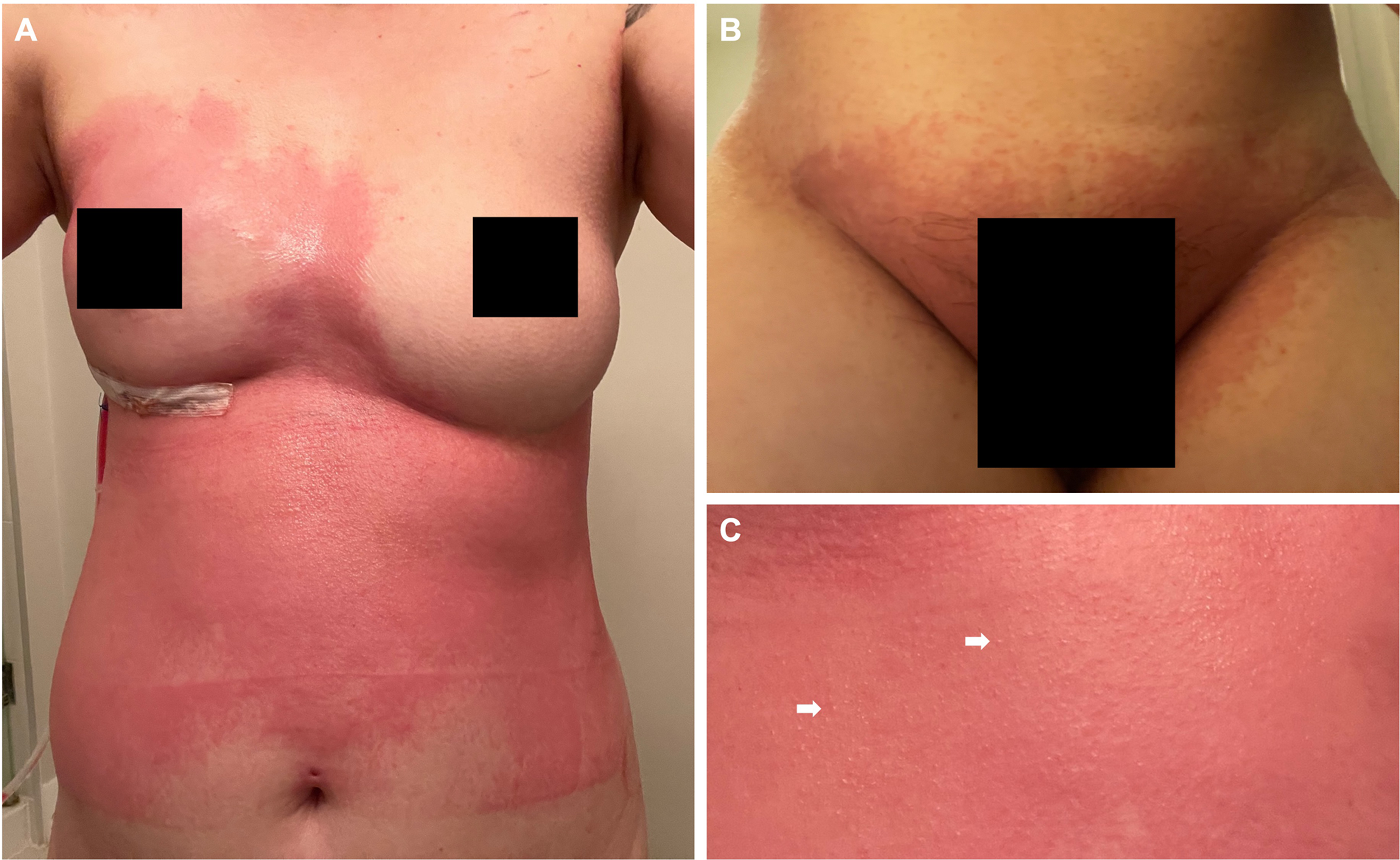
Extensive pruritic cutaneous eruption 2 days after right breast revision reconstruction with exchange of implant for tissue expander: (A) ill-defined confluent erythematous and eczematous plaques over the right breast extending down to the lower trunk; (B) rash extending to vulva region; (C) numerous tiny vesicles (arrows) scattered within the plaques.
She was later referred to the Contact Dermatitis Clinic and patched tested to the American Contact Dermatitis Society core allergen series (80 allergens), four antibiotics (including amoxicillin, cephalexin, clindamycin, and vancomycin), and peri-/post-operative materials (2% chlorhexidine solution, Betadine solution, 3 M SoluPrep sponge with 2% chlorhexidine, Steri-Strips, and Mepilex border dressing). She had a strongly positive reaction to bacitracin (Figure 2). Operative notes confirmed the use of a modified double antibiotic solution (80 mg tobramycin and 50,000 units of bacitracin in 500cc normal saline) for pocket irrigation and povidone-iodine for implant soaking. Therefore, a case of recurrent ACD to bacitracin was confirmed.
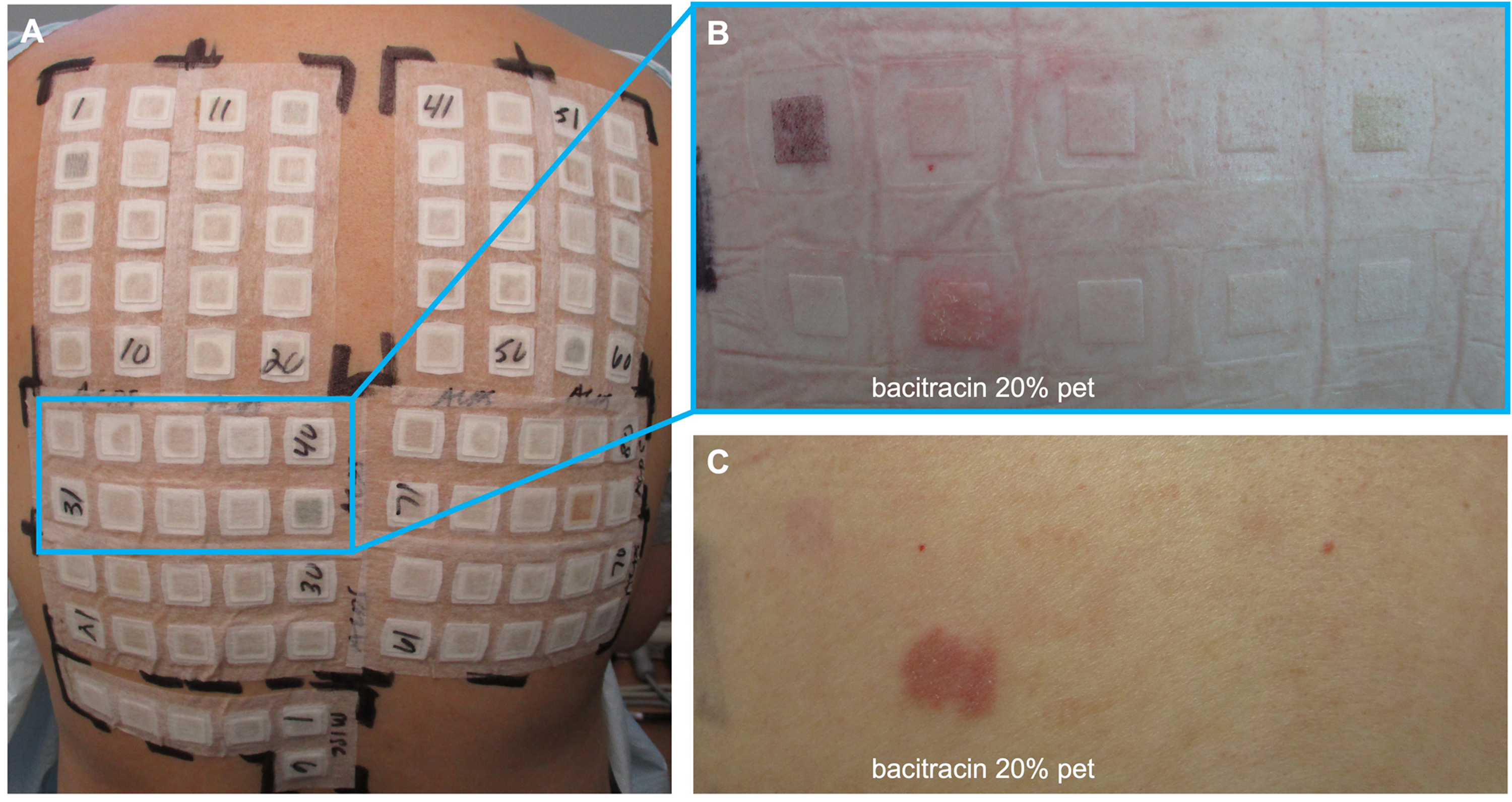
Patch test for assessment of allergic contact dermatitis: (A) patches with allergen in place on Day 1 of testing; (B) 2+ (strongly positive) patch test reaction to bacitracin 20% in petrolatum on Day 3 of reading; (C) persistent patch test reaction on Day 8 of reading.
Bacitracin is widely used as an antimicrobial pocket irrigation and implant soaking agent in breast surgery to decrease infection and capsular contracture. Although there are no evidence-based best practice guidelines for antimicrobial breast pocket irrigation, one study demonstrated that triple antibiotic solution (TAS; 50,000 units bacitracin, 1 g cefazolin, and 80 mg gentamicin) was the most popular and preferred by 40.5% of plastic surgeons followed by TAS with betadine with/without bacitracin (21.0%). 3 TAS was also the most popular choice for soaking of breast prostheses and utilized by 42% of plastic surgeons, followed by TAS with betadine variant (13%), or other (31%), including bacitracin alone. 3
Recognizing the presentation of ACD as delayed pruritic eczematous dermatitis is important as it can be mistaken for allergies to other systemic antibiotics. Approximately 7.7–9.2% of the patch-tested population was reported to have ACD to bacitracin. 4 With the wide use of bacitracin in pocket irrigation and implant soaking, ACD to bacitracin should be considered in any patient who has developed dermatitis soon after having bacitracin for pocket irrigation and implant soaking in breast surgeries. Povidone-iodine irrigation may be used as an alternative antimicrobial choice in breast surgery because ACD to povidone-iodine is less common with similar capsular contracture rates.5,6
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient has given written informed consent to publication of her case details including clinical photos.