
Abstract
Introduction
Breast cancer is the commonest cancer diagnosis in Canada, sadly representing 13% of cancer deaths in Canadian women. 1 No Canadian group is spared, but notably First Nations (FN), Métis and Inuit women 2 often present for care when the disease is more advanced than their European-descended counterparts, similar to other marginalized groups.2,3 To date, researchers have focused on treatment of breast cancer in the FN population, with a paucity of research exploring FN women's perceptions of, and possible barriers to, postmastectomy breast reconstruction (BR).2‐7 Herein we explore views of FN women who have received or would have been eligible for BR. Importantly, our study was completed by 2 FN women healthcare professionals, adding face validity to the work.
FN people in Canada face healthcare challenges. Ongoing colonialism, racism, and the generational effects of the Indian Residential School Systems (IRSS) continue to negatively impact the physical, social, emotional, and mental health of FN people. 8 Ninety-four calls to action in The Truth and Reconciliation Commission of Canada (TRC) seek to enact meaningful change in order to advance reconciliation following the legacy of the IRSS and to rectify past and present injustices imposed on FN people. In particular, call to action 19 declares that appropriate health services be made available to FN people, and this article investigates whether breast reconstruction, specifically, is available to FN women 9 and advocates for the development of culturally responsive protocols that support FN women as one approach to removing barriers in healthcare.
Method
The project proposal followed the Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans. 10 It was reviewed by the Alberta Innovates A pRoject Ethics Community Consensus Initiative (ARECCI). 11 ARECCI was started in 2003 in Alberta to address the gap in ethical oversight of quality improvement, evaluation, and human services projects, to minimize and mitigate risks to sponsors and stakeholders for project success which in turn builds public trust. Invitational flyers were distributed to local FN health and community organizations, and personal networking at FN community events was utilized. This was followed by purposive recruitment and snowball sampling via breast and plastic surgeons, an FN elder, and an FN health liaison.
Demographic information was collected to consider factors that may have contributed to participants’ interviews and lived experiences (Table 1). One-on-one semistructured interviews were conducted by an FN member of the study team and transcribed and subjected to thematic content analysis by several members of the team (FN and non-FN). The interview utilized 13 open-ended questions to guide conversations (Table 2). These questions were asked when applicable. Given the highly unique and personal journeys of our participants, questions and the content of each interview changed slightly based on each participant. An FN sharing circle, a ceremony led by an elder incorporating FN cultural traditions,12,13 was held after the individual interviews had been conducted. Sharing circles can vary based on different cultural protocols utilized by various FN communities, however, in general, sharing circles provide individuals the opportunity to share and reflect on their experiences in a respectful and supportive environment that is free from interruption and questioning. 14 A sharing circle usually begins with a prayer from an elder who is often there to facilitate. In addition, participants utilize FN oral traditions while an article (usually a feather) is passed around to indicate who is speaking. 14 In our study, this provided an alternative communal and culturally sensitive method of data collection. The FN elder provided culturally appropriate support to participants for discussing their perceptions and experiences.
Demographic Information on Women With and Without BR.
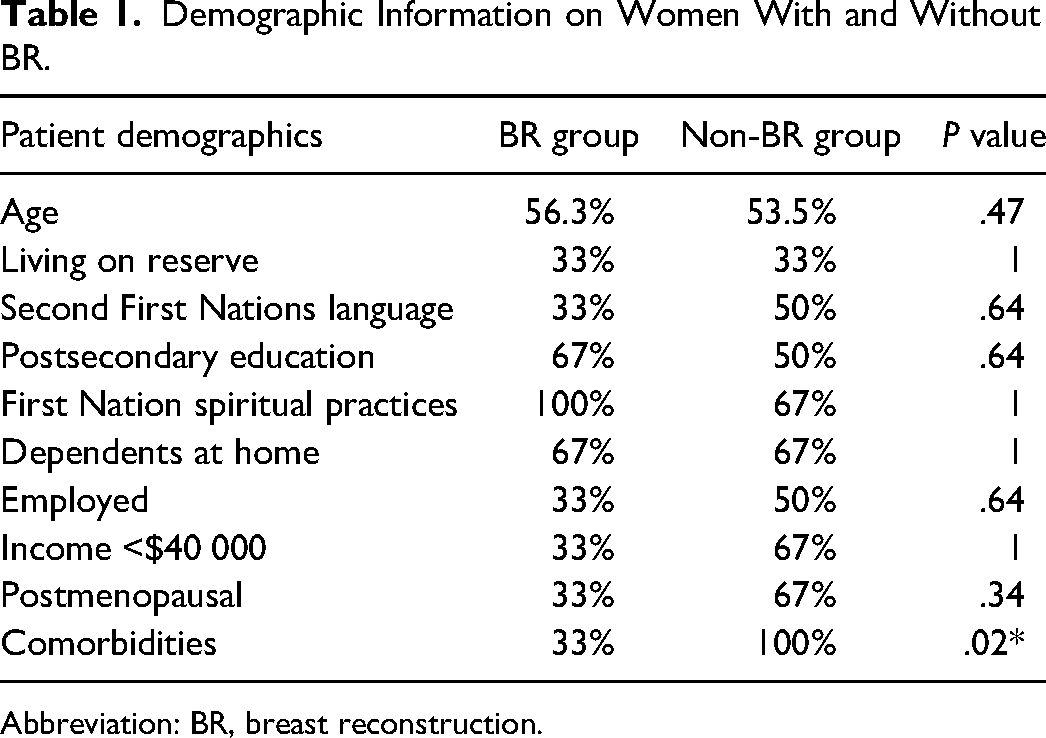
Abbreviation: BR, breast reconstruction.
Participants Were Asked 13 Open-Ended Questions.
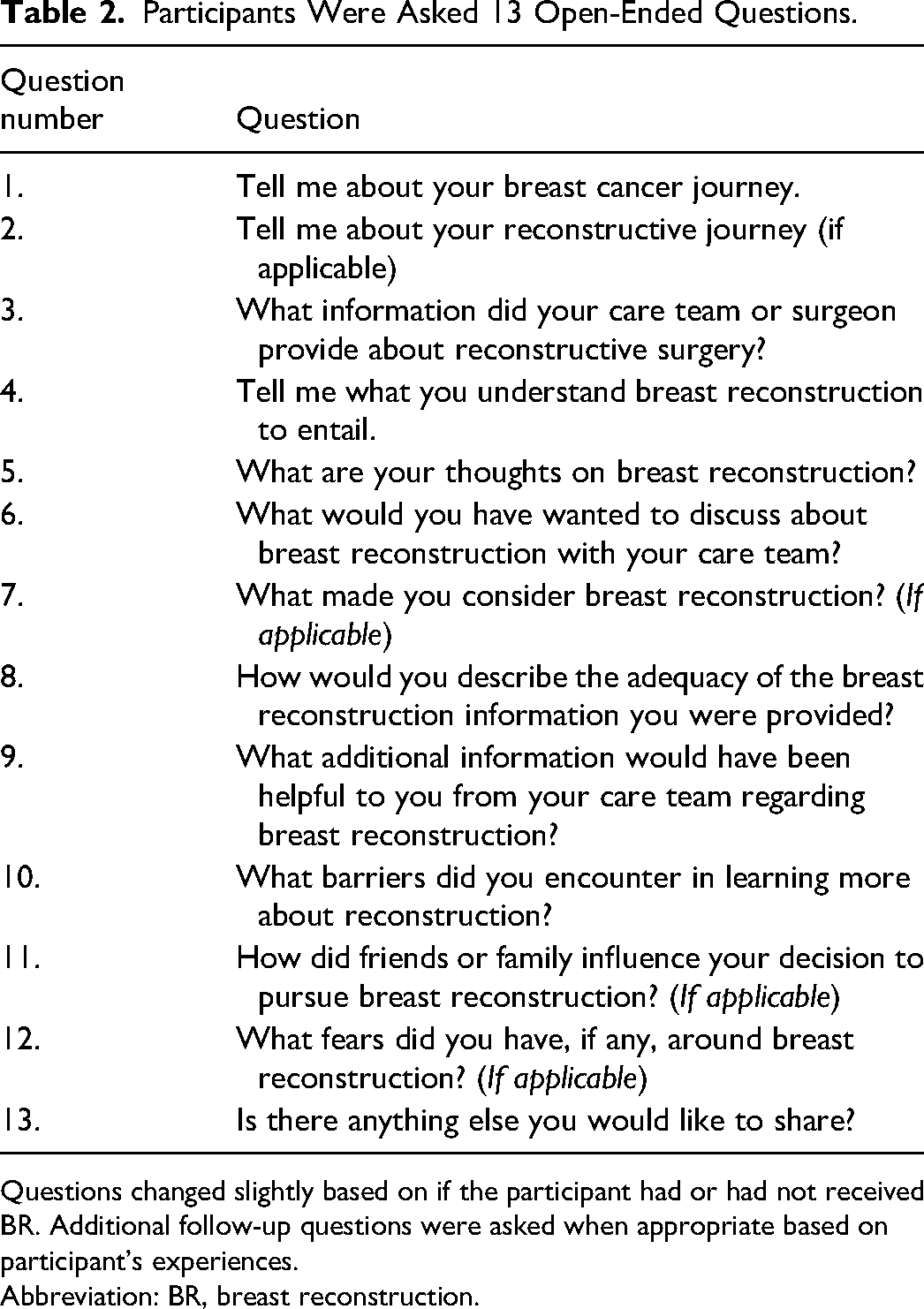
Questions changed slightly based on if the participant had or had not received BR. Additional follow-up questions were asked when appropriate based on participant's experiences.
Abbreviation: BR, breast reconstruction.
All 11 women in this study identified as FN. Nine women participated in the semistructured interviews, 2 of whom also participated in the sharing circle. Two additional women participated in the sharing circle only. Statistics were compared between the 9 women interviewed, 6 who received BR and 3 women who had not received BR. The t-test was employed to make continuous variable comparisons. Socstatistic.com calculator was used for statistical analysis.
Results
Breast cancer factors for both groups of women, those who had undergone or those who had not undergone BR, were similar including type of oncological surgery, chemotherapy, and radiation (Table 3). All 6 of the 6 women in the BR group had received mastectomy (vs lumpectomy) whereas 2 of the 3 women in the non-BR group had a mastectomy. Six of the 9 women were offered and pursued BR, while 3 of the 9 were either not offered or had not pursued BR.
Breast Cancer Treatment of Women With and Without BR.
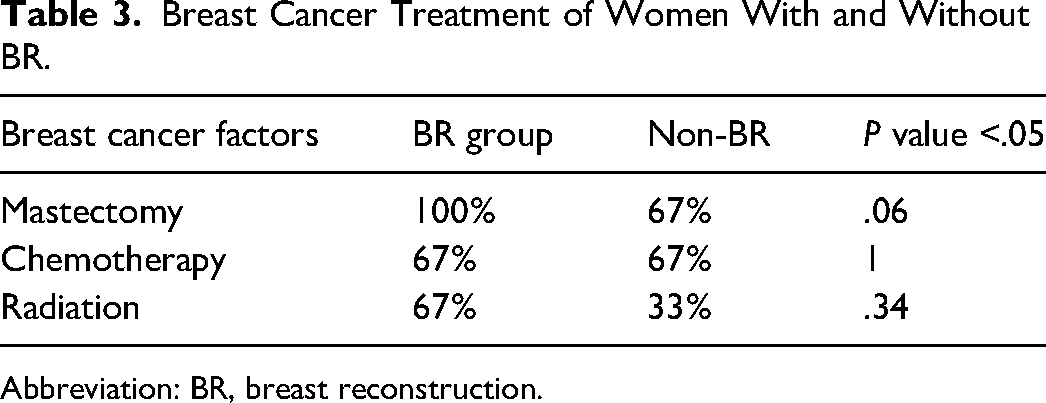
Abbreviation: BR, breast reconstruction.
Following thematic analysis, 4 key themes were identified: identity, information gaps, financial and transportation barriers, and the consequences of colonization.
Theme 1: Identity
The women who received BR expressed the importance of reconstruction for their sense of femininity, body image, and return to a previous sense of self. One participant voiced the importance of BR in making her feel like a woman: I felt that I wasn’t a woman [without] my breasts. I felt like I didn’t want to live anymore because it made me feel like I wouldn’t be a woman. So, the breast reconstruction really made and helped make me feel better about myself and helped bring confidence within myself…
Another woman discussed her feelings of self-consciousness before reconstruction with regard to wearing a prosthetic in her bra “I really felt self-conscious like wearing little fluffies to work in my bra…, I could only wear… I didn’t want to wear anything too low.” One woman related that it was her sense of self when nude that was problematic “when I have clothes on and things stuffed in there… when you take everything off and look at yourself… that's not what I want to be looking at for the rest of my life.”
Theme 2: Information Gaps
Both groups of women thought sufficient information about BR was lacking. They desired more plain language practical information with less medical terminology to allow them to make an informed decision about BR. One participant revealed “I didn’t know what kind of questions to ask this plastic surgeon after mastectomy… So that's where I was kind of lost…how to ask or what to ask.”
The women who were not offered BR, whether interested or not, expressed surprise that they were not given the opportunity to make that decision. When one woman was told that BR costs are covered by universal healthcare across Canada, she responded with surprise, stating “We’ve never been… we were never given that option.”
When one participant was asked what she knew about BR, she responded that she did not know anything. When asked if she had been informed about BR as an option, she replied: Nope. I have no clue what to expect. I’m hoping that doctor is going to call me and do a consult with me… to show me and tell me what is going to happen to me. But I haven’t had none of that… it's been two years and I’m still waiting… I don’t really know who I’m supposed to call… I don’t even have a number for anybody that I could call to even see where I’m on the list.
Additionally, the lack of information of the option to receive BR caused one participant to feel anxious stating “It does kind of raise your anxiety too, thinking why weren’t you told?”
Theme 3: Financial and Transportation Barriers
All the participants, including the 3 who lived on FN reserves, identified financial barriers as a contributing factor to accessing health services. One participant voiced: It costs a lot of money to go to your appointments every month, especially the radiation appointments every day. You have to consider parking, consider your meals, for attending an appointment.
When asked about barriers, another woman who lived on reserve described the challenges of getting into the city and using the transportation provided by health services: Sometimes transportation…they can only take you certain hours of the day…I always depended on that transportation. They really helped me a lot, with only myself I would have a hard time because it is so expensive, the gas and everything.
Another participant shared that without the medical transportation program, which provided transportation to and from medical appointments, she would not have been able to attend appointments and shared: I got connected with the driver program and that was great… I don’t know what I would have done without that… I live here and I had to travel to the Tom Baker.
One participant shared that following the prescription of antibiotics for an infection after her BR she encountered further barriers “Indian affairs actually contacted my doctor's office and questioned why and how long I was going to be on this medication. So I was thinking, why is that such an issue?”
Theme 4: The Consequences of Colonization
The effects of colonization, such as family abandonment and addiction which was intensified during the residential school experience, surfaced and impacted many of the women's breast cancer journeys. One woman described: I used to be an alcoholic and an addict… My life sucked. I lived awful. I used men. Men used me. I got a grip of myself …and I maintained eight years sobriety as of today. I still have my sobriety. And then I started going to get my body checked because it started paining in different places… So eight years in my sobriety I started going to go get myself a mammogram and pap smear.
Another discussed a lack of support during her cancer experience as she describes the interplay between addictions and family abandonment: My son was my main caregiver because my husband was…is an alcoholic. And during, he was there for the first little part. And then, he went on a binge. So he basically abandoned me through that, that time.
Another woman described how abandonment impacted her decision making around reconstruction. She stated “I’m fearful of even sleeping by myself. I don’t know why. I guess my childhood because I’ve been abandoned by my parents.”
Discussion
In this qualitative study, we explored perceptions of BR among FN women and found that identity, information gaps, financial and transportation barriers and the consequences of colonization effected whether the women in our study pursued or received BR. The demographic and breast cancer factor information collected in this study allowed comparisons of the FN women in BR and non-BR groups. Despite only comorbidities being found statistically different between the 2 groups, this data still provides insight into the background of FN women. Differences may exist, but the small sample is underpowered to reveal this.
Our study reports similar findings to other research that found that the socioeconomic status, ethnic background, and geographic location of the patient, influence the uptake of BR. 15 Zhong et al 16 also noted discrepancies in rates of BR in Ontario based on factors such as age, ethnicity, and location. Immediate BR was more common in younger women, while immigrant women were less likely to receive immediate BR (IBR), and neighborhood household income was lower in the mastectomy alone group versus the IBR group. 16 Alderman et al 15 found that minority women in LA and Detroit, particularly less acculturated Latinas, had low receipt of BR, likely due to limited access to information and to the procedure itself. These findings align with our study themes in that marginalized women face similar barriers when receiving or considering BR.
Regarding the theme identity, FN women in this study pursued BR for reasons similar to non-FN women, including a desire to restore a sense of femininity and self and improve their self-image.17–19 The participants described the nuisance of prosthetics. Mastectomy without reconstruction has been associated in some women with detrimental psychological side effects such as anxiety, depression, poor body image, and sexual issues17,18,20‐24 which were echoed by our participants. Although societal norms and expectations can motivate women's desire for accepted standards of femininity, the FN women in the BR group reported that their decision to have BR was free from pressure from friends, family, or spouse. This is similar to a non-FN population where women reported exercising individual choice and decision making without influence of friends, family, or spouses. 18 Since FN women expressed the desire to learn more about, and possibly pursue BR, the TRC call to action 19 is applicable in considering how to increase health equity with regard to holistic breast cancer care, including information about and access to BR.
Regarding information gaps, the women expressed their confusion, frustration and feeling of helplessness when they received pamphlets that were written in language too advanced and technical for their education level, and not presented in their Indigenous language. We found a systematic review of 15 qualitative research studies focusing on women diagnosed with breast cancer from nondominant ethnocultural groups, of which 2 studies focused on FN women. 25 These studies echoed that the lack of culturally and language-appropriate educational resources exacerbated language and communication barriers, contributing to feelings of isolation. Our participants suggested that educational information session pamphlets with pictures of BR results as well as videos be made more culturally appropriate and more easily available on FN reserves. Suggestions for ameliorating materials included inclusion of video rather than written materials; the provision of materials in women's own languages; and the provision of image-based information.
The FN women in our study suggested that oral rather than written information about cancer and BR could also be less threatening. Educational materials for these FN women could be improved if the importance of oral traditions and storytelling among FN people were incorporated as an important and holistic healthcare approach for Indigenous patients. A support group or peer volunteer program could encourage sharing of personal stories. In one study, culturally safe healthcare was demonstrated to show improved clinical outcomes, including higher patient satisfaction for FN patients who have diabetes mellitus. 26 Traditional FN cultural values can serve as a reliable source to improve FN women's BR access. In FN cultures there is a deep respect for oral traditions as both a source of knowledge and a method for teaching and learning. 10 Oral traditions and storytelling are central forms of communication in FN cultures. 10 Elders tell stories to teach cultural values and guide people toward balance and health. Stories are said to come alive as they are shared, so others can learn. 10 Personal experiences conveyed in stories are highly respected. 27 Telling one's personal story and journey related to BR can be a powerful vehicle to share information and help others consider their own decision to pursue or decline BR. 4
Currently there are existing educational and community events aimed at educating, empowering, and connecting women on the decision-making process and outcomes of BR surgery. A collaboration between the Canadian Cancer Society and the Canadian Society of Plastic Surgeons has resulted in “Breast Reconstruction Awareness Day” or BRA DAY, an annual Canada wide event that has also gained momentum internationally. The goal of BRA DAY is to provide information and a community for women considering BR, and since COVID, it has morphed into a national rather than city-based event, and held online as a webinar. While such events are promising, these events may not provide the support many FN women require, and the online offering may exclude those on reserves with unreliable internet connection. 28 The inclusion of FN elders and FN cultural practices may be beneficial at such events. Given that many FN people value a holistic approach, FN elders can provide support, knowledge, and cultural ways of being that may be beneficial for some women. 29
Regarding the theme financial and transportation barriers, our results show that FN women share many obstacles to BR encountered by other marginalized groups, such as immigrant women. 30 There are areas of overlap between FN and other marginalized women's breast cancer journeys including variables associated with poverty including high rates of comorbidity, the burden of addictions and abuse, lack of employment, dysfunctional family dynamics, and limited access to adequate healthcare. FN women also experience additional obstacles due to their experiences of colonization that in turn affect their access to adequate healthcare. The effects of colonization exacerbate and add an additional layer of complexity to women's breast cancer journey, and access to BR. Specific barriers unique to FN women that arose in our study include transportation to and from the reserve in addition to financial barriers. Our study agrees with others in that living on reserve serves as physical barrier to accessing healthcare as illustrated by various participants who were only able to attend medical appointments if subsidized transportation was available. 31 Depending on the scheduling of such transportation, limitations in accessing specialist's clinic hours or having to miss work could further add burden or limit access. FN women accessing care via transportation experience unique barriers because their relationship to being transported is informed by contemporary and historical colonialism. For example, the fact that medical care is far away for FN women living on reserve is due to the forcible relocation to remote reserves in the first place. Additionally, FN women's relationship to transportation has been disturbed by events such as children being forcibly transported away from reserve to residential schools, and the pass system where FN people required an Indian Agent approved pass to leave reserves. These events inform FN women's specific perspectives on, and readiness to use, transportation to access healthcare.
One unique challenge to the FN women noted in our study is the barrier of accessing the Non-Insured Health Benefits (NIHB). NIHB coverage is fraught with challenges including insufficient information on compensation models and patient coverage benefits, 32 voiced by one of our participants. Addressing this barrier, and other transportation and financial barriers, are important aspects in improving FN women's breast cancer care and access to BR.
Regarding the consequences of colonization, the women in our study shared their experiences with abandonment, alcohol use disorder, and addictions. It is important to consider the challenges FN women face that are specific to their experiences of colonization. FN women bear the burden of colonization and institutionalized racism, which in turn affects their self-esteem and sense of empowerment. Colonization has created socioeconomic barriers for FN people that are especially difficult to overcome. These social and institutional barriers inhibit constructive change and negatively impact FN communities’ ability to access basic human needs. 12 Various elements of intergenerational trauma that stem from the IRSS surfaced in our study including addiction and abandonment. These elements are unique to the legacy of colonization and the effect it has had on FN peoples. It has been well documented that FN people are impacted by substance use and face disproportionate harms related to it. 33 Regarding abandonment, traditional child-rearing practices were impeded by the IRSS leading to emergence of negative parenting practices. 34 While exploring this idea would be out of scope for this study, colonialism has impacted FN gender ontologies and our participants understanding of their own gender has impact on their perspectives of BR. When considering colonialism and its effect on FN peoples, the impact has largely determined FN health as we know it today. 35
Moving forward, the role of academic institutions and the Canadian plastic surgery community needs to ensure culturally sensitive training and Indigenous ways of knowing are incorporated into their practices when serving Indigenous patients. Furthermore, healthcare professionals need to make themselves aware of continued health inequalities while working to ensure these inequalities are addressed as mandated by the TRC calls to action. 36 In order for many of the themes identified in our study to be meaningfully addressed, Canada must train and educate more Indigenous physicians, including in plastic surgery. 36 Indigenous plastic surgeons can serve as a bridge between Indigenous communities/patients and ensure these inequalities are addressed in a respectful way that is centered in trust and FN ways of being. 36 Expanding the diversity of plastic surgeons, including Indigenous people, will likely lead to more research such as this, to improve Indigenous health.
In summary, FN women share many obstacles to BR with other marginalized women, such as lack of access to adequate healthcare due to conditions of poverty and racism. Additionally, FN women face unique obstacles to BR due to their collective experiences of colonization, including a climate of institutional racism and a historically based fear of Western-based medical services. The results obtained provide direction to overcome these particular obstacles faced by FN women, such as developing more appropriate educational materials on BR that is reflective of FN women's worldview and lived experiences.
As this study explores a new area of research, there is a need for further research to substantiate and expand its findings. Limitations include the small sample size, which is related to challenges accessing this participant population. Breast cancer and reconstruction can be a sensitive and personal topic for most women, creating a challenge in recruitment. FN communities are wary when approached for research endeavors, given the history of exploitation in such undertakings. 37 Another limitation is that the select study group has higher rates of BR than general Alberta women BR rates, due to the purposeful sampling method employed. The need to make BR more accessible to both FN and non-FN women suggests further studies are needed with FN and other women involving larger and more representative sample sizes. The addition of more specific research questions, such as a deeper exploration of FN cultural values as they relate to BR is also required. Furthermore, we recognize another limitation of our study is the inclusion of data from only cis women and thereby infers gender as a binary concept. Further studies should include those who have received BR who are nonbinary people, transgender women, and various additional genders. This current study provides evidence of an opportunity to engage in constructive work, development of thoughtful educational resources, emphasizing oral communication and the telling of personal stories, with the inclusion of the FN women in the process of developing these materials.
Conclusion
This study confirms existing research that healthcare providers do not consistently discuss BR with women who have breast cancer. Marginalized women, including FN women, are at a distinct disadvantage, and FN women have further obstacles because of colonization. When offered, FN women are receptive to considering BR. Geographic isolation and low socioeconomic status, exacerbated by the continuing effects of colonization and its attendant racism, impact uptake of reconstruction. A first step includes improving methods of informational delivery regarding BR.
Footnotes
Acknowledgments
The authors thank the Alberta Cancer Foundation Richard R. Singleton Summer Student Scholarship for its support of this work.
Previous Presentation
Presented at Canadian Society of Plastic Surgery Annual Meeting 2015.
Breast Reconstruction perceptions and access in First Nations women.
Ethical Approval
This study was conducted as a quality improvement project. The project and its ethical parameters were reviewed by the Alberta Health Services’ internally recognized ARECCI (Alberta Research Ethics Community Consensus Initiative) quality improvement review process. All recommendations of the review process were integrated into the study design and deployment. Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HD received Alberta Cancer Foundation Richard R. Singleton Summer Studentship to fund this research. HS, CW, and CT have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research of this article: This work was supported by the Alberta Cancer Foundation Richard R. Singleton Summer Studentship.
Author Contributions
HS contributed to study analysis, background research, manuscript creation, and revision. HD was involved in study design, obtained ARECCI review, conducted all interviews and focus groups, transcription, study analysis, and draft revision. CW performed study design, obtained ARECCI review, study analysis, and draft revision. CT was involved in study design, obtained ARECCI review, study analysis, manuscript creation, and draft revision.
Appendix
Glossary of Key Terms.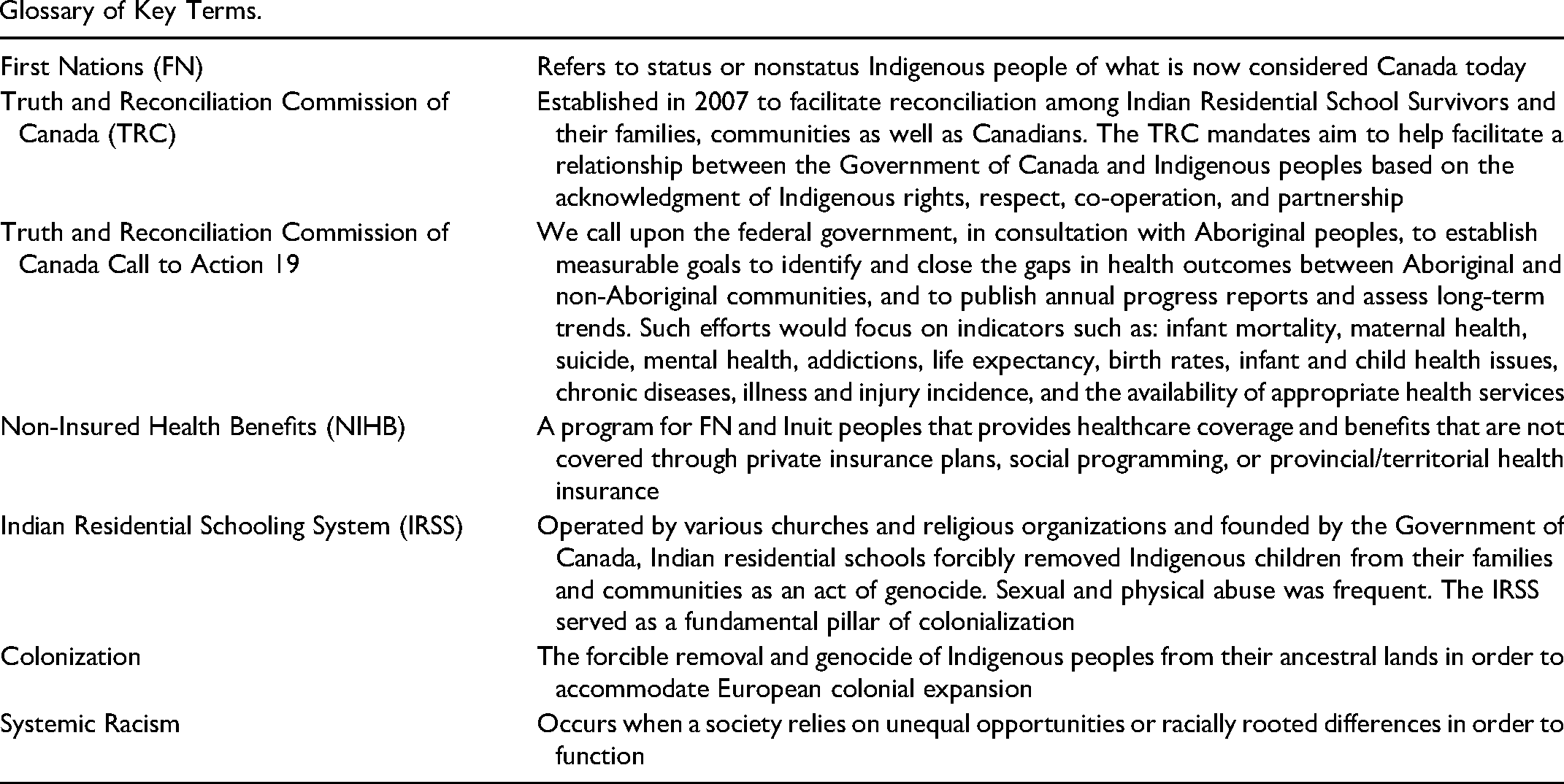
First Nations (FN)
Refers to status or nonstatus Indigenous people of what is now considered Canada today
Truth and Reconciliation Commission of Canada (TRC)
Established in 2007 to facilitate reconciliation among Indian Residential School Survivors and their families, communities as well as Canadians. The TRC mandates aim to help facilitate a relationship between the Government of Canada and Indigenous peoples based on the acknowledgment of Indigenous rights, respect, co-operation, and partnership
Truth and Reconciliation Commission of Canada Call to Action 19
We call upon the federal government, in consultation with Aboriginal peoples, to establish measurable goals to identify and close the gaps in health outcomes between Aboriginal and non-Aboriginal communities, and to publish annual progress reports and assess long-term trends. Such efforts would focus on indicators such as: infant mortality, maternal health, suicide, mental health, addictions, life expectancy, birth rates, infant and child health issues, chronic diseases, illness and injury incidence, and the availability of appropriate health services
Non-Insured Health Benefits (NIHB)
A program for FN and Inuit peoples that provides healthcare coverage and benefits that are not covered through private insurance plans, social programming, or provincial/territorial health insurance
Indian Residential Schooling System (IRSS)
Operated by various churches and religious organizations and founded by the Government of Canada, Indian residential schools forcibly removed Indigenous children from their families and communities as an act of genocide. Sexual and physical abuse was frequent. The IRSS served as a fundamental pillar of colonialization
Colonization
The forcible removal and genocide of Indigenous peoples from their ancestral lands in order to accommodate European colonial expansion
Systemic Racism
Occurs when a society relies on unequal opportunities or racially rooted differences in order to function