
Abstract
Introduction
The global incidence of breast cancer is substantial, having recently surpassed lung cancer to be the most diagnosed cancer at 11.7% (2.3 million cases) of all new cancer diagnoses in 2020. 1 It is the most commonly diagnosed cancer in women, at 24.5% of all diagnoses. 1 These statistics are mirrored when looking specifically at North America. 1 Fortunately, most breast cancers diagnosed in North American women are diagnosed at an early stage.2,3 Patients diagnosed with localized breast cancer often have the treatment option of mastectomy with immediate breast reconstruction (IBR).
IBR contributes to improved quality of life, with increased measures of psychosocial well-being and body image in breast cancer survivors.4,5 Rates of IBR have been increasing, with a 42% 10-year increase among Canadians and 30% increase among Americans as a proportion of total mastectomies delivered.6-8 Although patients may choose an implant-based (alloplastic) or tissue-based reconstruction, alloplastic IBR is heavily favored and represents approximately 75% of all reconstructions. 7
Acute and chronic pain are major concerns for patients in their recovery after breast surgery. Severe acute postoperative pain increases the likelihood that patients will experience chronic pain in the breast and ipsilateral arm. 9 Chronic post-operative pain—defined as pain continuing beyond 3 months post-surgery—is experienced by approximately 36% to 47% of mastectomy patients.9,10 Factors associated with increased chronic pain include young age, adjuvant radiotherapy, and axillary lymph node dissection. 9 Despite the benefits and increased delivery of IBR, there is a lack of consensus on the risk of acute and chronic pain following IBR as compared to mastectomy alone.11-14
Patient reported outcome measures (PROMs) are tools that solicit the patient's perspective on the impact of their medical condition and its treatment. Examples of PROMs for psychosocial well-being, sexual well-being, physical well-being, and overall satisfaction with the procedure and outcome are EORTC-Q30/Q23, SF-36, and FACT-B. 15 However, these tools do not sufficiently query patients on their post-operative acute and chronic pain experiences. 16
Although studies have examined rates of post-operative pain in breast cancer patients undergoing mastectomy with IBR, these sources are few and rarely concentrate on alloplastic IBR. 17 With rising rates of alloplastic IBR across North America, there is an increasing need to comprehensively evaluate chronic pain in this specific patient population. The primary objective of this study is to quantify the burden of chronic pain in women who have undergone alloplastic IBR. Specifically, we sought to examine the prevalence, severity, quality, and interference of chronic pain in this cohort using validated PROMs. Our secondary aim is to compare 3 validated PROMs for measuring chronic pain in this population. The results of this study will inform the future use and interpretation of PROMs of chronic pain in patients undergoing alloplastic IBR.
Methods
Study Sample
This multi-site cross-sectional survey study recruited women who underwent mastectomy with alloplastic IBR between January 2018 and March 2021 at 3 institutions. Inclusion criteria were female patients 18 years or older, fluent in English, with a breast cancer diagnosis or undergoing prophylactic mastectomy, who received mastectomy with alloplastic IBR at least 3 months prior to recruitment. Alloplastic IBR includes patients who have undergone either a single or a 2-stage reconstruction with implants. All patients underwent reconstruction with acellular dermal matrix sutured to the chest wall. The majority of patients underwent subpectoral reconstruction, with a minority undergoing prepectoral placement.
Patients were not eligible if they were currently receiving radiation therapy at the time of recruitment given the potential for acute effects of radiotherapy to confound chronic pain results. Eligible patients received initial contact by email or post as a cross-sectional group at least 3 months post-surgery. The invitation to participate outlined the purpose and goals of the study. Consent was obtained using either an electronic or paper consent form. Participants could complete either an online or paper-based questionnaire. Patients were sent 2 reminder emails if they did not initially respond.
Chronic Pain Assessment
The Breast Cancer Pain Questionnaire (BCPQ), Brief Pain Inventory (BPI), and BREAST-Q were completed by participants.
The BCPQ is a condition-specific instrument to assess chronic pain in post-surgical patients. 9 Pain severity and frequency are self-reported in 4 regions: area of the breast, axilla, arm, and side of the body. Severity is ranked on a 0 through 10 scale, with 10 being the most severe pain. Frequency is established on a 3-point scale: (1) almost every day, (2) 1 to 3 days a week, or (3) more rarely. For each participant, a Pain Burden Index (PBI) is generated to summarize the quantitative scores of pain severity and frequency. 18
The BPI is a well-established generic tool to assess patient perception of pain severity or intensity and how it interferes with daily life. It has been used to measure pain in the setting of cancer and post-surgery. 19 The BPI was used in this study to complement the cancer-specific PROMs.
The BREAST-Q is a validated procedure-specific PROM for breast reconstruction.20,21 Questions querying satisfaction with breasts, psychosocial well-being, sexual well-being, and physical well-being were selected from the Breast Cancer module. Normative data has been developed for BREAST-Q scores, including evidence from a control group versus patient pre-operative scores and for evaluating change following breast reconstruction.20,22 The BREAST-Q has limited questions directly addressing post-surgical pain, which include the frequency of different pain qualities (eg, aching and throbbing).
Data Collection
Participant medical records were reviewed and data collated for demographics and medical history data including age, BMI, cancer diagnosis, time since surgery, and breast size. Details of the surgical procedure were recorded including anesthesia type, lymph node dissection or biopsy, reconstruction stages, surgical indication, and incision type. Ethnicity was self-reported.
Statistical Analysis
Descriptive statistics were used to analyze demographic and chronic pain data gathered from the PROMs. Each respondent's PBI was calculated using the formula: (frequency[1-3]* severity breast pain[0-10]) + (frequency[1-3]* severity arm pain[0-10]) + (frequency[1-3]* severity axillary pain[0-10]) + (frequency[1-3]* severity side pain[0-10])18,23 Higher numbers indicate a larger pain burden.
Results from both the BCPQ and BPI were used to calculate the total prevalence of chronic pain among respondents. Quality of pain was evaluated using responses from the BREAST-Q. A non-respondent analysis was not possible given that patient consent was required to access medical records. The sample size was determined by the number of surveys returned and its adequacy was assessed at the time of analysis.
Risk factor analysis was carried out in R version 4.0.4. 24 Demographic and clinical variables were compared between patients with and without pain using Wilcoxon rank sum tests for continuous variables and Fisher's exact tests for categorical variables. Linear regression was used to test for the relationship between PBI and demographic/surgical variables. p < .05 was considered statistically significant. Variables emotional health, self-confidence, and sexual confidence were interpreted as numeric variables: 1 = None of the time and 5 = All of the time.
To assess reliability between instruments for the presence of chronic pain, key questions that best queried the binary presence of pain were taken from each of the PROMs. Patients were only able to answer “yes” (they experience chronic pain) or “no” (they do not) to these questions. The 3 PROMs were compared using Fisher's exact tests.
Results
A total of 351 eligible patients were contacted and 118 consented to participate in the study. The study response rate was 33.6%. Patient characteristics are outlined in Table 1. The study population had a median age of 50 (range 29-74) and BMI of 22.5 kg/m2, with most of a BMI <25. Most respondents (77.1%) self-reported their ethnicity as Caucasian, with the second most reported ethnicity (9.3%) being East Asian (eg, Chinese, Japanese, and Korean).
Study Population Characteristics (n = 118).
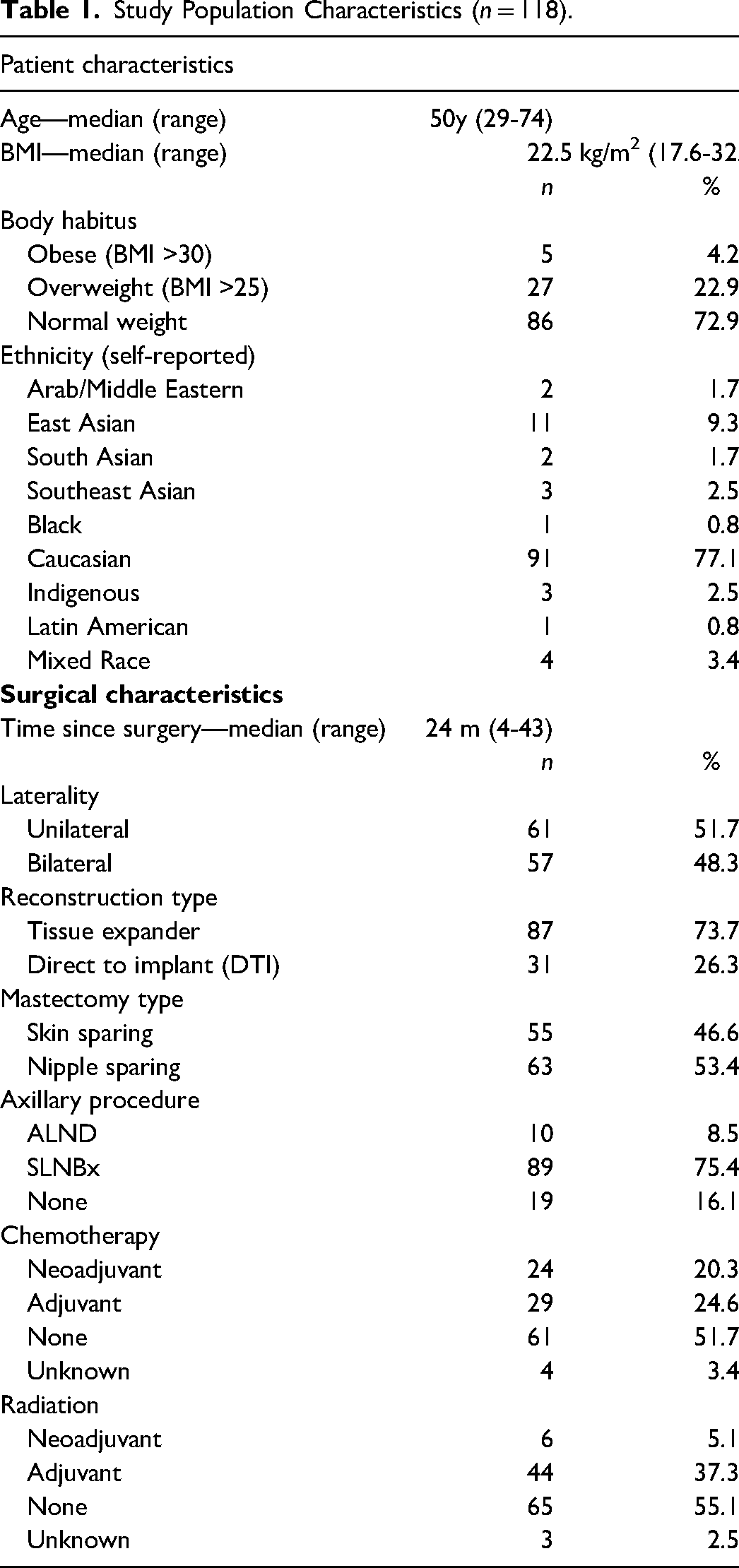
The median time from surgery to survey completion was 24 months (range 3-43). Approximately half (51.7%) had unilateral procedures. Most (73.7%) respondents underwent 2-stage reconstruction, with the placement of a tissue expander prior to implant. Slightly more respondents received nipple-sparing mastectomy (53.4%) compared to skin-sparing. For axillary surgery, 75.4% had a sentinel lymph node biopsy and 8.5% had a full axillary lymph node dissection. A minority of patients received chemotherapy (44.9%) and radiation (42.4%).
Prevalence of Chronic Pain
A total of 52.5% of respondents experienced pain in at least one of four areas (breast, armpit, side of the body, or arm on the side). The most common location was the breast, reported by 45.7%. Pain on the side of the body was the second most common location (37.1%), and the arm was least reported (19.8%). Frequency of pain was reported in a similar pattern, with side pain and breast pain experienced most frequently. Of the 62 respondents reporting chronic pain, 18 (29.0%) had consulted a physician within the past 3 months for their pain and 13 (21.0%) used analgesics for this chronic pain.
Severity of Chronic Pain
Of those participants reporting chronic pain (n = 62, 52.5%), the severity of pain was widely distributed for both “average pain” and “worst pain,” ranging from 1 up to 9 on an 11-point Likert scale (Figure 1). Among those reporting chronic pain (n = 62), the median value of “average pain” was 3.1. Pain severity did not differ by location.
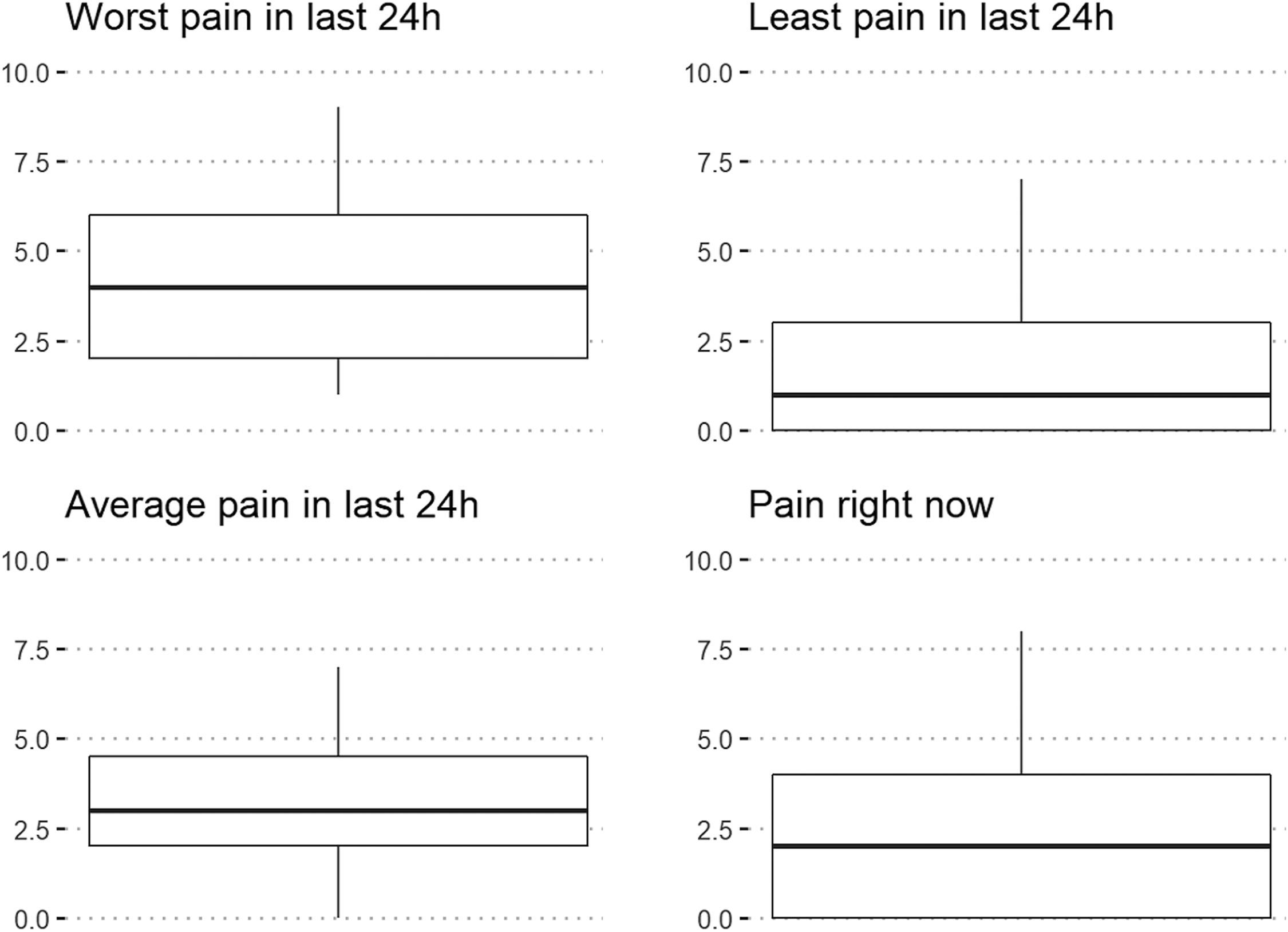
Pain severity from the brief pain inventory 11-point scale (n = 62). Box plots show the (a) median worst pain experienced over the last 24 hours (b) median least pain experienced over the last 24 hours (c) median average pain experienced over the last 24 hours and (d) the pain being experienced right now by the 62 respondents who reported experiencing some level of chronic post-surgical pain.
Median PBI for only those reporting chronic pain was 17.3 on a maximum index of 120 (Figure 2). For most of these patients, pain burden was relatively minor (<10.0); 8 patients reported a pain burden of over 30.0.
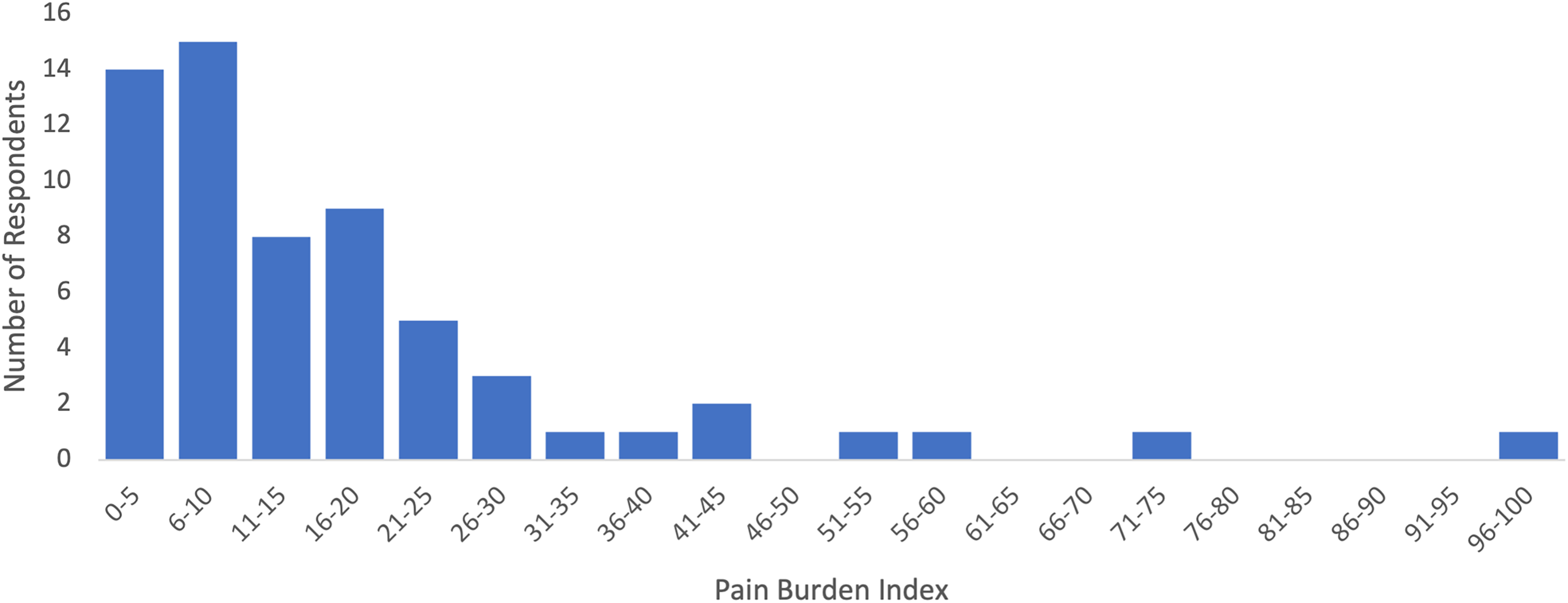
Severity of pain for those reporting chronic pain (n = 62).
Quality and Burden of Pain
The majority of respondents (67.8%) reported a sensory disturbance or quality of discomfort in one of four locations (breast, side, armpit, and arm). “Breast tightness” was experienced by 66.6% of respondents at least “some of the time” (Figure 3) and 63.2% experienced “pulling.” Over one-third of respondents experienced sharp pain or aching, with a minority (4.4%) reporting sharp pain “all of the time.” Throbbing was the least frequently reported (15.8%). Arm lymphedema was self-reported by 8.8% of this cohort.
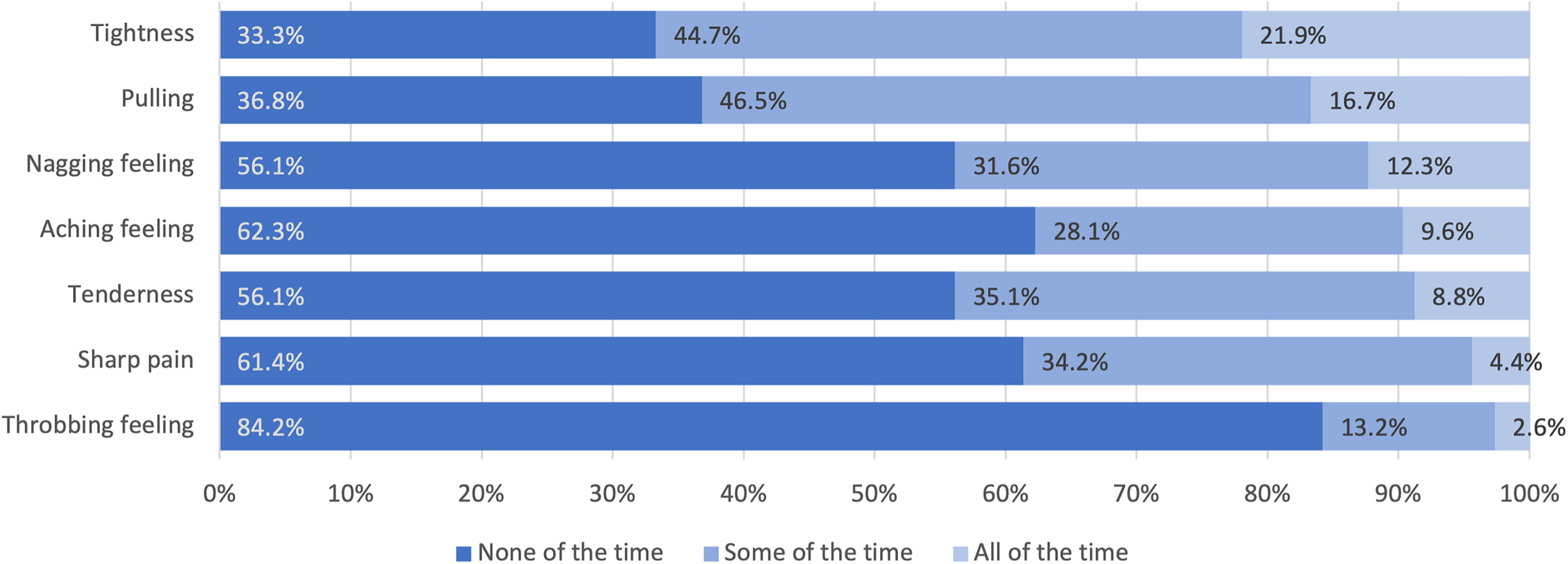
Quality of chronic pain (n = 114).
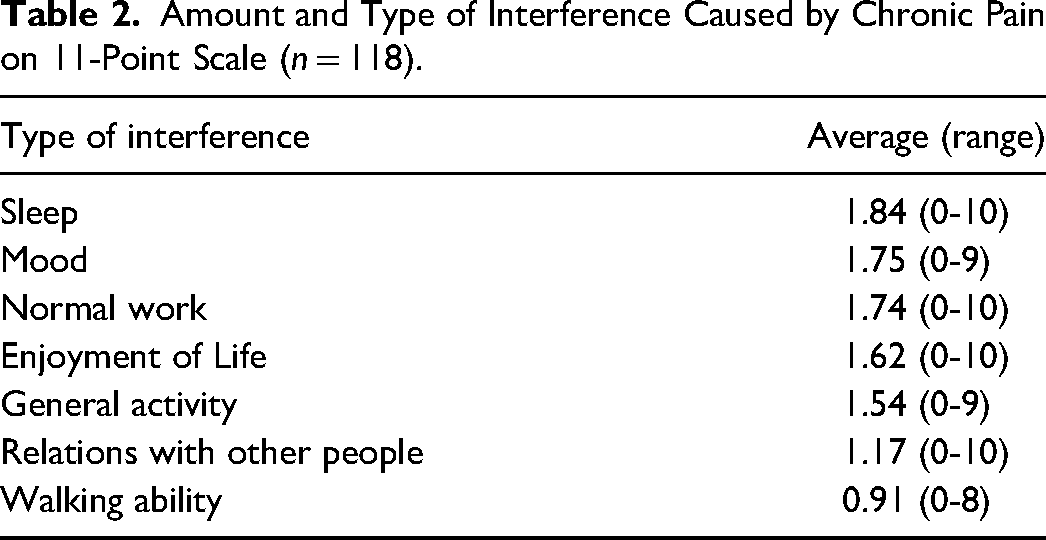
Pain interfered most commonly with sleep, mood, normal work, and general enjoyment of life (Table 2). Overall, the majority did not report strong interference with activities; only 5.9% of respondents rated their sleep interference above 8 and 4.3% rated their mood interference above 8.
Amount and Type of Interference Caused by Chronic Pain on 11-Point Scale (n = 118).
Risk Factors
There was a significant association between chronic pain and radiation (p = .018), emotional health (p = .0003), self-confidence (p = .022), and sexual confidence (p = .044).
With respect to the burden of pain, there was a significant relationship between PBI and laterality of reconstruction (p = .05), emotional health (p = .01), self-confidence (p = .00036), and sexual confidence (p = .02). Patients receiving bilateral reconstruction reported an average of 4.67% higher on the PBI than those receiving unilateral reconstruction. For each categorical improvement in emotional health, self-confidence, or sexual confidence, PBI decreased by an average of 3.75%, 3.75%, and 2.00%, respectively.
There was no statistically significant correlation between the presence of pain or PBI and age, BMI, breast size, mastectomy type, incision type, axillary surgery, 1-stage versus 2-stage, ethnicity, months since surgery, chemotherapy, or presence of lymphedema.
Inter-Tool Reliability
Questions that queried the binary presence of chronic pain were taken from each of the 3 PROMs and data was compared to assess inter-tool reliability. These questions were:
BCPQ: Do you have pain in the area of the breast, armpit, side of the body, or arm on the side where you were operated? BPI: Throughout our lives, most of us have had pain from time to time (such as minor headaches, sprains, and toothaches). Have you had pain other than these everyday kinds of pain TODAY? BREAST-Q: In the past week, how often have you experienced: Sharp pains in your breast area?
Participant answers correlated across all the instruments for the self-reported presence of chronic pain (p < .0001).
Discussion
This study provides a comprehensive evaluation of chronic pain in patients undergoing mastectomy with alloplastic IBR, including the prevalence, severity, quality, and risk factors associated with chronic pain. For the 52.5% of patients reporting chronic pain following alloplastic IBR, pain was most frequently experienced in the breast itself and side of the body. The patients who did experience chronic pain reported moderate severity of pain. Pain burden was endorsed by a minority, with those patients experiencing severe pain in multiple locations. The presence of pain was correlated with radiation, worse emotional health, and less self and sexual confidence. There was a high correlation in the reporting of chronic pain across 3 validated instruments in this population.
In this cross-sectional study, 52.5% of patients report chronic pain after mastectomy and alloplastic IBR. Previous studies of chronic pain in this patient population report prevalence rates ranging from 7.3% to 90.9%, with a pooled prevalence of 26.3% across 10 studies and 534 participants.25-33 A meta-analysis of breast cancer patients undergoing either alloplastic or autologous reconstruction reported a mean pain prevalence across 12 studies of 32.8% (24.4-42.5%). 17 Existing research on chronic pain using the BCPQ in patients undergoing mastectomy alone reports an average pain prevalence of 47%. 9 It is currently unclear whether data from our study represents a significant deviation from this, thus warranting further study. Additionally, given the effect of response rate on the reported prevalence in this study and others, it is necessary to interpret these results in the context of a cross-sectional study design. The wide range of prevalence rates may be caused by selection and response biases, as well as variance in the instrument used for reporting pain.
Importantly, a minority experienced a high pain burden and pain interference. The PBI quantifies burden by incorporating severity and frequency of pain across 4 different locations. This is useful to diagnose any underlying etiology and evaluate therapeutic effects of targeted interventions. In this cohort, few patients obtained medical advice or used analgesics; their reported PBI was significantly greater than those who did not. PBI may be useful in a clinical setting to assess the presence and burden of chronic pain and evaluate the effectiveness of interventions.
The measure of pain severity was consistent with previous studies24,27,34,35: on an 11-point scale, the average pain among all respondents was 1.72 and 3.27 for those who reported at least some pain. As expected, the mean “worst pain” was consistently greater than the mean “least pain” reported. The wide range of scores reported between worst, least, and average pain demonstrates its fluctuant nature whereby patients with chronic pain may experience days with mild pain, severe pain, or no pain at all.
Risk factors for chronic pain identified in this study agree with and extend the findings of other reports. Bilateral reconstruction is associated with a greater burden of chronic pain than unilateral reconstruction. 11 Radiation is associated with the development of chronic pain. 9 Our study sample was inadequate to analyze the risk factors of Direct-to-Implant (DTI), Axillary Lymph Node Dissection,33,34,36,37 and age,11,36 as suggested by other studies. Our analysis did not identify ethnicity as a risk factor for pain, however, our cohort lacked ethnic diversity with over 75% self-identifying as Caucasian.
Our study found that chronic pain may influence social and personal adjustment after mastectomy and IBR. Patients who experienced higher levels of pain reported feeling emotionally healthy or self/sexually confident far less often than those with less pain. This suggests that chronic pain results in an emotional burden in addition to a physical burden.
Existing research in this area has used broad, heterogeneous methods and survey tools to assess chronic pain. We used 3 different PROMs to assess how results may differ depending on how questions are asked. Despite a difference between the chronic pain prevalence indicated by the BCPQ (53%) versus the BPI (46%), further analysis showed this was not statistically significant. Differences in how researchers query chronic pain, in addition to its subjective nature, may account for the spread in published prevalence rates.
A gold standard tool to query chronic pain among this population is needed to create comparability between studies. Due to its ability to assess the binary prevalence of chronic pain as well as the severity of the pain with the PBI formula, the BCPQ may be a good candidate for a preferred tool.
Limiting factors of this study include its cross-sectional nature, subjective experiences of pain, and lack of pain baseline for each patient prior to surgery. Patients who experienced pain may be more compelled to share their experiences, potentially resulting in self-selection bias. 38 In addition, completion of a non-respondent analysis was not possible due to consent requirement to review medical records. With fewer than 50% of eligible patients participating, our study population may not adequately represent the target population, leading to a sampling bias. Our analyses were exploratory in nature and hypothesis-generating to examine chronic pain in this specific population, thus a target sample size for the power of the study was not prespecified. Perioperative pain management may also be a confounding factor: since 2020, the majority of patients have received perioperative regional blocks with preoperative analgesia (Tylenol, gabapentin, and Celebrex) but prior to 2020, there were significantly fewer regional blocks being done. Finally, most of the patient sample self-identified as Caucasian. Despite an intention to investigate ethnicity as a risk factor, diversity was not obtained in the study sample.
Conclusion
Chronic pain may burden patients who have undergone mastectomy with alloplastic IBR. There is an opportunity to prevent, assess for, and intervene in the presence of chronic pain. Future research efforts are warranted to establish a gold standard PROM for this patient population and to prospectively evaluate chronic pain.
Footnotes
Acknowledgment
Dr Kathryn Isaac is the holder of the Dr Patricia Clugston Chair in Breast Reconstruction Surgery at the University of British Columbia and would like to acknowledge the support of VGH and UBC Hospital Foundation's donors and partners who made this Chair possible. We also thank statisticians Arianne Albert and Ulrike Mayer for their contributions.
Author Contribution
LR designed and led the study. CI provided technical and administrative support. SM, PL, CD, NVL, and EB provided access to patient lists and medical records. KI conceived and supervised the project. LR, CI, and KI contributed to the final manuscript.
Data Availability
Data will be made available upon request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Informed consent was obtained from all individual participants included in the study. UBC CREB: H21--00405.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Mach-Gaensslen Foundation of Canada.