
Abstract
Introduction
Spinal cord injury (SCI) results in disturbance of normal sensory, motor and autonomic dysfunction, contributes to substantial disability and loss of independence, and ultimately restricts participation and quality of life. 1 In cervical SCI, individuals lose upper limb function in addition to lower limb function and bowel and bladder control. In Canada, there are an estimated 21,000 people with traumatic cervical SCI living in Canada, 2 with over 750 new injuries each year. 3 The economic impact of SCI on the healthcare system has become an increasingly important topic. The average lifetime cost of cervical SCI is estimated to be $3 million per individual, with an annual cost of $2.7 billion across Canada, which includes equipment and home modifications, and attendant care.4,5
People living with cervical SCI have identified improvement of upper limb function as a top priority over other essential functions.6–8 Recent advancements in the surgical treatment of peripheral nerve injuries offer promising opportunities to improve upper limb function in traumatic cervical SCI.9–14 Nerve transfer surgery offers several advantages over traditional tendon transfer techniques15–18 but can be time-sensitive due to concomitant lower motor neuron involvement.19–22 Both nerve and tendon transfer surgeries have the potential to substantially improve quality of life and independence, and reduce caregiver burden as well as personal and societal costs.
Unfortunately, surgery (nerve transfer, tendon transfer) to improve upper limb function remains under-utilized in this population world-wide. 23 In the United States, it was estimated that only 14% of people that would benefit from tendon transfer receive care. 24 No studies have examined surgery rates in this population in Canada, or the rate of nerve transfers in this population exists. The purpose of this study was to evaluate the utilization of nerve and tendon transfer surgery in cervical SCI across Canada. Specifically, we sought to determine rates, regional variations, and change in utilization of nerve and tendon transfer surgery in cervical SCI performed in Canada over the last 16 years. By understanding the number of Canadians with cervical SCI undergoing nerve and tendon transfer surgery, we can better understand the gap in care that exists, and identify the barriers that may be preventing individuals from accessing care; thereby reducing the burden of illness in Canadians living with cervical SCI.
Methods
Study Design and Setting
We conducted a retrospective analysis of all nerve and tendon operations performed in Canada (excluding the province of Québec) in individuals with traumatic SCI between fiscal years 2004/05 and 2019/20. This study used data from the Canadian Institute for Health Information (CIHI) Discharge Abstracts Database (DAD) and the National Ambulatory Care Reporting System (NACRS). These data holdings capture administrative, clinical, and demographic information on all patients discharged from acute care hospitals in Canada excluding Québec. The databases contain individual, coded, linkable data that include longitudinal inpatient and outpatient healthcare interactions. The NACRS database contains information on day surgery, clinics and emergency departments, while the DAD contains data on day surgery, acute inpatient hospital admissions, and rehabilitation settings. Québec data were not included because parity information is currently not available in the province's clinical administrative data submitted to CIHI. Prior studies have successfully used the DAD and NACRS databases to determine national rates of various surgeries including mastectomies, 25 Caesarian sections, 26 and lower extremity amputations. 27 The large size of this database makes this dataset ideal for tracking rare diseases such as cervical SCI.
Population
Individuals who sustained a traumatic SCI were identified in the DAD and NACRS databases using the enhanced Canadian version of the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada (ICD-10-CA) codes for SCI (see Supplement 1). Only the first occurrence (NACRS visit or DAD hospitalization) was included. The date of admission/registration was defined as the first occurrence of SCI and to identify the interventions of interest. Data linkage was used to query the NACRS and DAD databases for all nerve or tendon operations subsequently performed in these individuals using ICD-10-CA Classification of Health Interventions (CCI) codes (see Supplement 2, Supplement 3). To identify those undergoing nerve transfer, the codes for “nerve graft” and “nerve repair” were combined (Supplement 2). We also obtained data on other nerve procedures: “nerve excision” and “decompression/neurolysis” (Supplement 2), which were recorded separately. For tendon transfers, we included codes for other procedures that could be performed in conjunction with upper extremity reconstruction such as “arthrodesis/joint fusions”; data on “tendon release” was recorded separately (Supplement 3). Unlinkable records (records with invalid or missing health card numbers or birth years) were excluded.
Analyses
Data were aggregated by year intervals (2004-2009, 2010-2015, 2016-2019) and provinces (British Columbia, Manitoba/Saskatchewan/Alberta, Ontario, Newfoundland/New Brunswick/Prince Edward Island/Nova Scotia). Data on level of SCI (cervical, thoracic, lumbar, sacral), sex, average age, and length of hospital stay were obtained. The frequency of nerve transfers and tendon transfers was calculated as the number of events in each time interval. These data were compared to published national data on incidence of traumatic SCI to determine the utilization of nerve and tendon transfer. Previous studies have reported that 60% to 75% of individuals with cervical SCI would benefit from some type of upper extremity tendon transfer.28–31 A conservative estimate of 50% was used as a denominator of those eligible and willing to undergo surgery based on previous research. 24
Data across provinces were compared to assess regional variation of upper extremity reconstruction. Data were compared across years to evaluate the trends in rates of nerve and tendon transfers over the last 16 years. No identifiable information was collected and where there were fewer than 5 cases reported, the data were suppressed. All data analyses were performed with SAS® University Edition. Institutional research ethics board review was obtained.
Results
Rates of Nerve and Tendon Transfer Surgery in Cervical SCI
The number of nerve and tendon procedures performed in individuals in Canada with cervical SCI from 2004/05 to 2019/20 are presented in Table 1. A total of ≤ 80 nerve transfer procedures were performed over 16 years and the majority of procedures were done on younger patients (mean age 38.3 years) and male patients (81%). During the same period, a total of 61 tendon transfers (78% male, mean age 45.0 years) and 40 arthrodesis procedures (70% male, mean age 47.1 years) were performed in individuals with cervical SCI. All nerve and tendon procedures were performed as day surgery or with a single overnight stay.
Upper Extremity Reconstruction Procedures Performed for Individuals With Cervical SCI in Canada Between 2004/05 and 2019/20.
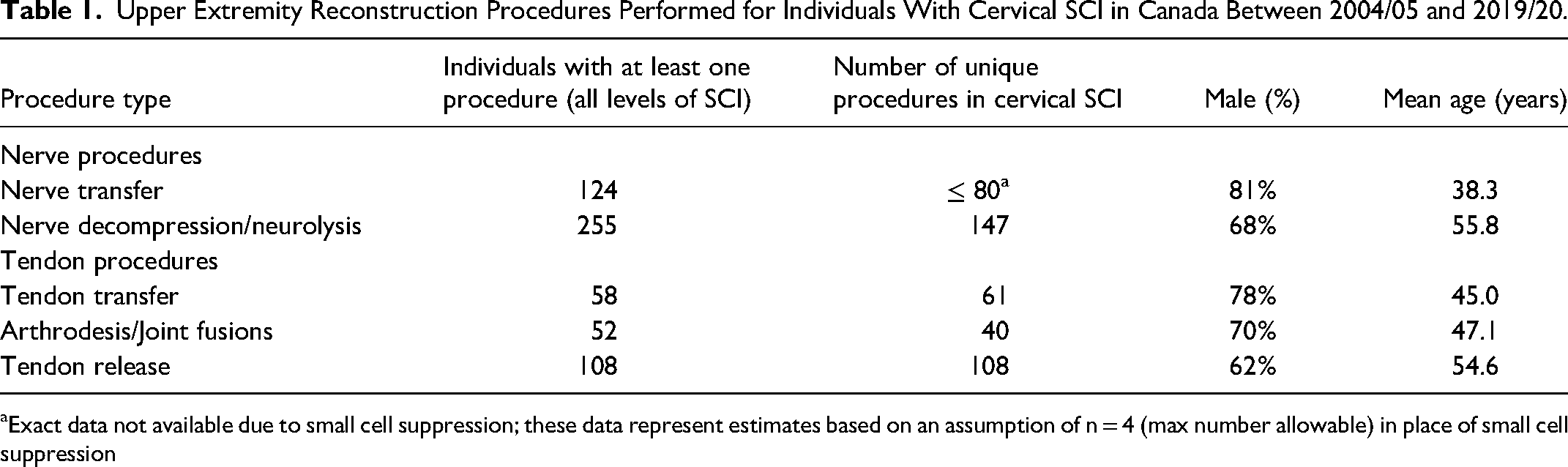
Exact data not available due to small cell suppression; these data represent estimates based on an assumption of n = 4 (max number allowable) in place of small cell suppression
An estimated 787 individuals sustain a traumatic cervical SCI each year in Canada. 3 Using a conservative estimate of 50% eligibility, and assuming that one procedure is performed in each individual, approximately 1.3% of eligible individuals undergo nerve transfer, and an average of 1.0% of eligible individuals undergo tendon transfer.
Changes in Utilization of Nerve and Tendon Transfer Surgery Over Time
The change in nerve and tendon procedures in SCI over each time interval is shown in Figure 1. The number of nerve transfers increased over time (2004-2009, n = <5; 2010-2015, n = 27; 2016-2019, n = 49), while the number of nerve decompressions, tendon transfers, and arthrodesis procedures has remained relatively constant.
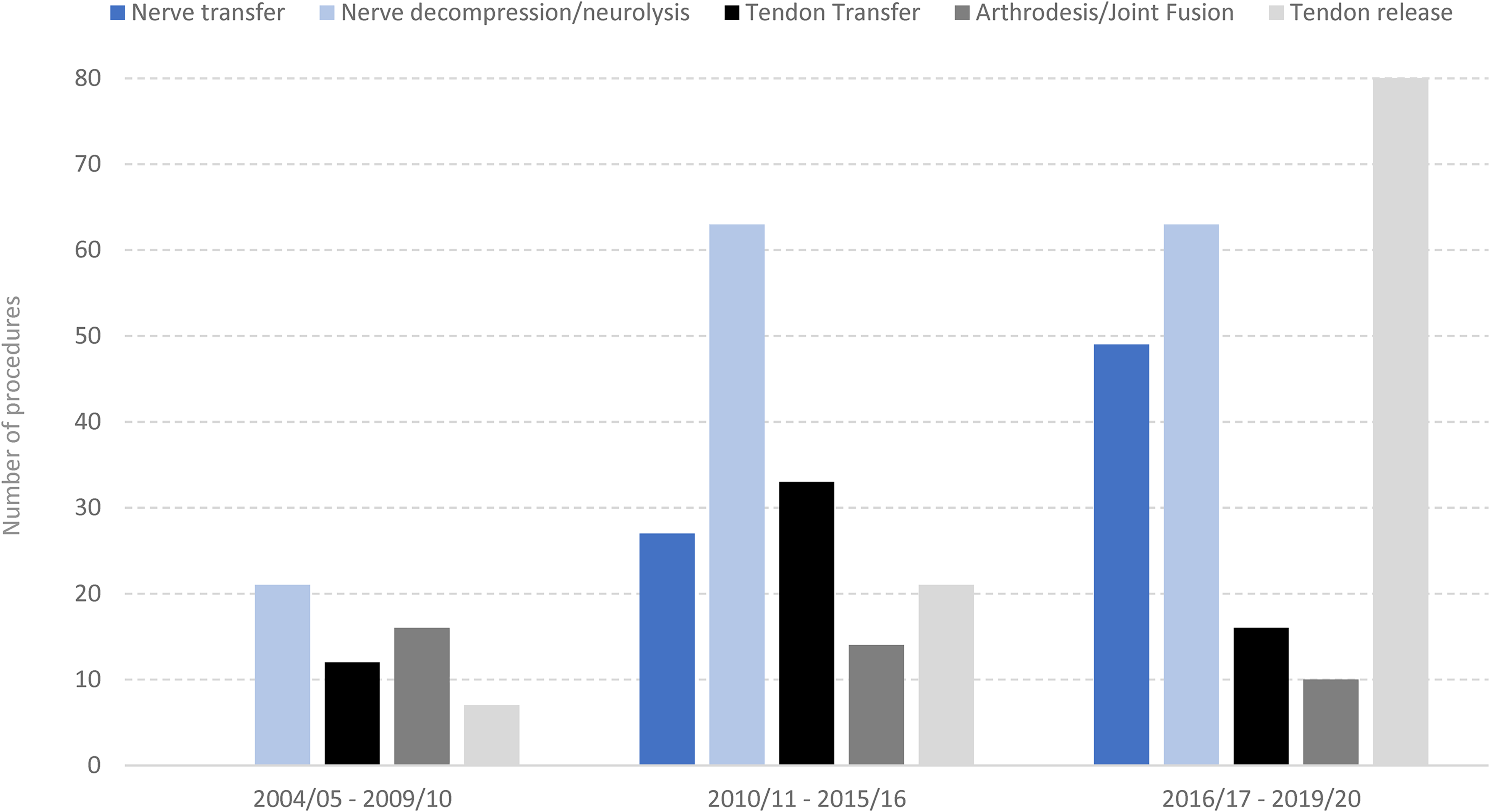
Number of upper extremity nerve and tendon procedures in traumatic cervical SCI have changed over time.
Regional Variations in Nerve and Tendon Procedures
Regional variations in upper extremity nerve and tendon procedures performed in cervical SCI between 2004/05 and 2019/20 are shown in Table 2. The total number of procedures was highest in Ontario (n = 166) and British Columbia (n = 119).
Regional Variations in Upper Extremity Nerve Procedures (Nerve Transfer, Nerve Excision, Nerve Decompression), and Tendon Procedures (Tendon Transfer, Arthrodesis, Tendon Release) Performed in Individuals With Cervical SCI in Canada.
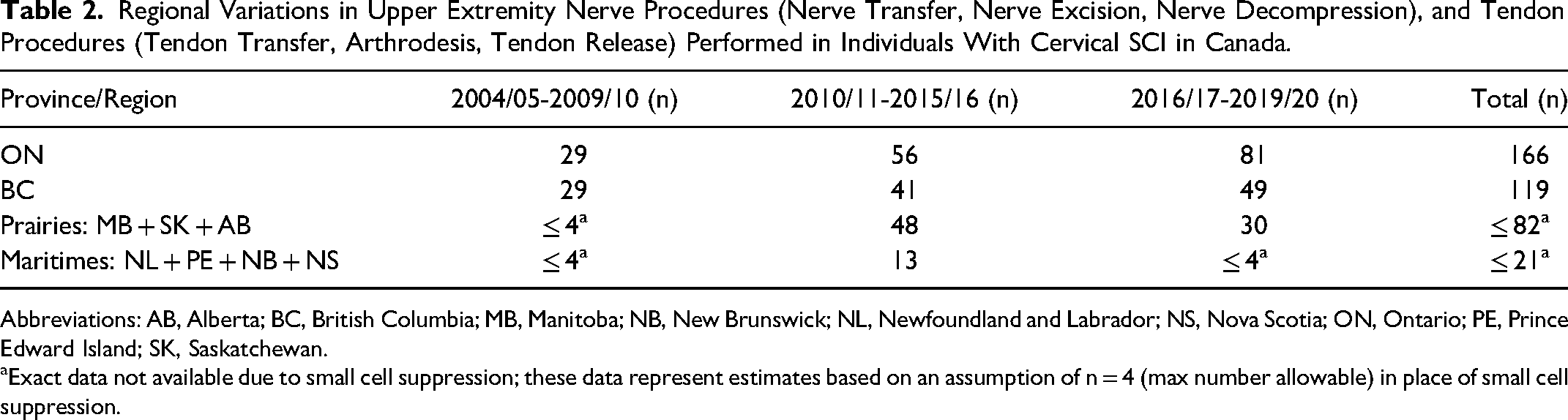
Abbreviations: AB, Alberta; BC, British Columbia; MB, Manitoba; NB, New Brunswick; NL, Newfoundland and Labrador; NS, Nova Scotia; ON, Ontario; PE, Prince Edward Island; SK, Saskatchewan.
Exact data not available due to small cell suppression; these data represent estimates based on an assumption of n = 4 (max number allowable) in place of small cell suppression.
Discussion
Our findings demonstrate that the number of individuals with SCI who receive surgery to improve upper limb function is low, despite upper limb function being identified as a top priority by this population.6–8
Previous studies have reported that the majority of adults (over 18) with traumatic SCI in Ontario are male (74.1%) with a mean age 51.3 ± 20.1 years. 32 These data are similar to the national estimates from 2018 (77% male; average age 53.4 years old). 5 Our data on surgical rates in the traumatic cervical SCI population in Canada show similar demographics (Table 1). Notably, the mean age at time of nerve transfer (38.3 years) and tendon transfer (45.0 years) are lower than for nerve decompression (55.8 years), and tendon release (54.6 year). These differences may reflect the timing of nerve and tendon transfer as procedures to provide new function after injury as compared to nerve decompression and tendon releases, which are associated with prolonged use and treat syndromes that may develop over time. Individuals with SCI are at high risk of developing upper limb compression neuropathies, such as cubital tunnel and carpal tunnel, due to positioning and weight-bearing activities on the upper limbs. 33 Nerve decompression can alleviate symptoms of compression neuropathy and improve function. 33 Tendon/muscle releases are used in SCI to treat contractures that result from spasticity. Further research would be warranted to examine time to procedures post index injury.
The rates of nerve transfer and tendon transfer surgery found in our study are exceptionally low, with 1.3% of eligible individuals undergoing nerve transfers and 1% undergoing tendon transfers. These rates may be an overestimation based on the assumption that one procedure was performed per individual. However, a single individual may have several nerve and/or tendon transfers performed in each limb, 9 and therefore the identified rates may reflect fewer unique individuals who underwent nerve or tendon transfer. In a 2005 study of tendon transfer rates in the United States, Curtin et al reported a low utilization rate of 14%, 24 which is much greater than the rate found in our study. This highlights the need to understand, contextualize, and address local and regional barriers that may be affecting access to care in Canada.
Notably, although tendon transfers for individuals with SCI were introduced in the 1960s 34 and the first report of nerve transfers in SCI was published in 2012, 35 the rates of tendon transfer procedures are similarly low to nerve transfers. This suggests the need for knowledge dissemination and implementation efforts targeted at surgical procedures to improve upper limb function including both nerve and tendon transfer procedures. Importantly, there are advantages to each of these procedures and choice of reconstruction should be individualized to patient's clinical circumstances and preferences. 36 Furthermore, although incidence of nerve decompression is higher than nerve and tendon transfer (Table 1), numbers are still comparatively low, pointing to an underdiagnosis and treatment of compression neuropathy in this population. 33
While overall rates of procedures are low, there has been an increase in nerve transfers over time (Figure 1). Many factors may influence the rise in procedures, such as increasing awareness of nerve transfers among individuals with SCI and/or their healthcare providers, and an increase in the number of surgeons trained in these procedures. There are increasingly more interdisciplinary clinics across the country to serve this patient population. Regional variation in upper extremity surgical procedures (Table 2) follows population densities of the corresponding provinces (Ontario: 14.8 million > Prairies: 7.0 million > Maritimes: 2.4 million) with the exception of British Columbia (population 5.1 million), where rates of upper extremity surgical procedures are greater than in the Prairies. 37 Further research would be warranted to examine why regional differences exist. For example, relatively higher incidence of surgery in British Columbia may reflect a difference in practices and relationships among SCI healthcare providers, surgeons, and advocacy organizations. Moreover, this province has a single rehabilitation hospital that cares for all patients with SCI. This may make it easier to streamline and implement changes in SCI care. The present study reinforces the need to understand how improvements can be made to increase access and availability of surgeries for persons with traumatic SCI in Canada.
Limitations
Database research has inherent limitations including the risk of under- or over-estimates of incidence. Submissions to the DAD and NACRS were not mandated in all provinces during the selected time period; and no data were included from Québec. This may lead to under-estimates of upper extremity reconstruction. As there was no ICD-10-CA/CCI intervention for nerve transfer, we used related procedure codes for “nerve grafting” and “nerve suture” which are the codes used by surgeons to describe their operative procedures. It is possible that these codes may have captured procedures other than nerve transfer. Using an estimate of 50% to represent those eligible and willing to undergo nerve transfer surgery was based on previous studies of tendon transfers. This is likely an underestimation since nerve transfers expand eligibility given the ability to restore function at higher levels (C5) and availability of nerve donors. Finally, small cell suppression limited the data we obtained. Nonetheless, the large size of the national database used for this study makes this dataset ideal for tracking rare diseases such as cervical SCI.
Conclusion
Nerve and tendon transfer surgery to improve upper limb function in Canadians with cervical SCI remains very low. This study highlights a substantial gap in care for this vulnerable population, however progress is being made. Identification of the barriers that prevent access to care has begun to develop and promote best practice guidelines for delivering upper extremity surgical care.
Supplemental Material
sj-docx-1-psg-10.1177_22925503221120544 - Supplemental material for An Examination of Utilization Rates Over Time of Nerve and Tendon Transfers in Canada to Improve Upper Limb Function in Cervical Spinal Cord Injury
Supplemental material, sj-docx-1-psg-10.1177_22925503221120544 for An Examination of Utilization Rates Over Time of Nerve and Tendon Transfers in Canada to Improve Upper Limb Function in Cervical Spinal Cord Injury by Jana Dengler, Maytal Perlman, Michelle Jennett, Edyta Marcon and Sara Guilcher in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503221120544 - Supplemental material for An Examination of Utilization Rates Over Time of Nerve and Tendon Transfers in Canada to Improve Upper Limb Function in Cervical Spinal Cord Injury
Supplemental material, sj-docx-2-psg-10.1177_22925503221120544 for An Examination of Utilization Rates Over Time of Nerve and Tendon Transfers in Canada to Improve Upper Limb Function in Cervical Spinal Cord Injury by Jana Dengler, Maytal Perlman, Michelle Jennett, Edyta Marcon and Sara Guilcher in Plastic Surgery
Supplemental Material
sj-docx-3-psg-10.1177_22925503221120544 - Supplemental material for An Examination of Utilization Rates Over Time of Nerve and Tendon Transfers in Canada to Improve Upper Limb Function in Cervical Spinal Cord Injury
Supplemental material, sj-docx-3-psg-10.1177_22925503221120544 for An Examination of Utilization Rates Over Time of Nerve and Tendon Transfers in Canada to Improve Upper Limb Function in Cervical Spinal Cord Injury by Jana Dengler, Maytal Perlman, Michelle Jennett, Edyta Marcon and Sara Guilcher in Plastic Surgery
Footnotes
Acknowledgments
We wish to acknowledge the contributions by Melanie Barwick, Sander Hitzig, Anita Kaiser, Kristin Musselman, and Christine Novak for their assistance with this manuscript.
Ethics Statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was waived. Ethics approval was obtained from the Sunnybrook Health Sciences Centre Research Ethics Board (Project ID 1749).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Canadian Society of Plastic Surgeons Educational Foundation's Clinical/Outcomes Study Grant, “Utilization of reconstructive surgery to improve upper limb function in cervical spinal cord injury in Canada.”
Supplemental Material
Supplemental material for this article is available online.
Presentation of Work
Jan 2022: E-poster. Utilization Rates of Nerve and Tendon Transfer to Improve Upper Limb Function in Cervical Spinal Cord Injury. 2022 American Association for Surgery of the Hand Annual Meeting. Carlsbad, CA. January 2022.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.