
Abstract
Introduction
Submucous cleft palate (SMCP) is a congenital condition initially described by Roux in 1825 1 and further characterized by Calnan who specified the triad findings of a midline muscular diastasis (zona pellucida), notch of the posterior border of the bony palate and bifid uvula. 2 It has an estimated incidence of 0.02% where 2 of the 3 findings are present. 3 SMCP diagnosis is easily missed due to its subtle clinical findings, which are often not examined for until the development of, or delay in the development of, speech. 4 Some children will have earlier detection due to persistent ear infections or difficulty feeding. Diagnosis and subsequent treatment are therefore frequently late relative to the population of children with an overt cleft palate for several reasons.
Surgical techniques for SMCP are many and include palatal reconstructive techniques (Furlow double opposing Z-Plasty (FP), radical intravelar veloplasty (IVV)+/− palatal pushback flaps), pharyngeal wall techniques (sphincter pharyngoplasty (SP), pharyngeal flap (PF)) and combination procedures of the above. The question remains as to which surgical technique offers the optimal outcome, that being resolution of velopharyngeal insufficiency (VPI) without need for further operative intervention.
A Cochrane review in 2008 for the management of submucous cleft was eventually withdrawn in 2016 as being out of date and not meeting current methodological standards. 5 Gilleard et al published a comprehensive systematic review in 2014 addressing a similar question based on speech outcomes. 6 Their review found little conclusive evidence for establishing the most efficacious technique due to the mixed etiologies of the included study populations, and lack of objective validated speech assessments for the studies included. 6 Furthermore, this was not restricted to the pediatric population. To date, there is no clear evidence in the pediatric population to support which technique best addresses SMCP-associated VPI. Given the difficulty in comparing speech outcomes between populations without an established and consistently used speech assessment tool, we have elected to compare the proportions of patients recommended for secondary surgery to address residual VPI as our determinant of surgical success.
Specifically, our goal is to determine the surgical technique that yields the best result for SMCP in the pediatric non-syndromic population as defined by the lowest rate of recommended secondary surgery due to persistent VPI. The analysis will also take into account overall speech improvement rates and complications reported for each surgical technique, where possible.
Methods
The systematic review was registered online with Prospero (ID CRD42020153761). A detailed search strategy was developed and conducted in order to identify relevant articles for review (Appendix 1).
Several databases were searched from inception: Ovid MEDLINE, Embase, CENTRAL, Web of Science Core Collection, CINAHL, and Health Technology database. Clinical trial registries (clinicaltrials.gov, OpenTrials), conference proceedings (PapersFirst, Proceedings), and theses and dissertations (ProQuest Dissertations & Theses Global, Theses Canada Portal, Networked Digital Library of Theses and Dissertations) were searched for additional unpublished studies. These database and gray literature searches were supplemented with forward and backward citation chaining to identify any studies missed by the initial search. Prior to the final analysis, searches were repeated such that newly published studies were included. There were no limitations on publication date or language in the search. Only full publications were included in the final review.
Identified publications underwent a 2-stage screening process against the inclusion and exclusion criteria, first at the title and abstract stage, followed by a full-text review of studies included at first screening. This was completed in duplicate by 2 independent reviewers (SG and LB), and disagreements were resolved with consensus. Inclusion required that (1) studies included pediatric patients treated surgically for nonsyndromic SMCP, and (2) studies included data on postoperative speech outcomes. Case studies and systematic reviews were excluded, as studied in which data for pediatric patients or patients with SMCP only or nonsyndromic patients could not be separated. Non-English publications were translated into English for review.
Following 2-step screening, the 2 independent reviewers extracted data in duplicate from included publications. Data extraction was facilitated by a template that was created in Microsoft Excel Version 16.54 (Redmond, WA). This data extraction template was piloted on an initial 10% of full-text papers and modified as required, following recommendations by the Cochrane Handbook for Systematic Reviews of Interventions. 7 Extracted data included the following: year of publication, location of study, study design, number of patients with nonsyndromic SMCP, gender of patients, age of patients at diagnosis and at surgery, criteria for diagnosis of SMCP, method of speech assessment, presence of pre- and postoperative speech therapy, surgical technique, recommendation for and number of secondary procedures performed, postoperative speech outcomes, postoperative complications (fistula, OSA, hyponasality), and length of follow-up.
Additionally, the quality and risk of bias of studies meeting inclusion criteria were assessed independently by both reviewers using the McMaster tool. 8 Disagreements were resolved by consensus between reviewers.
Data Analysis
Collected study data were organized in a table and analyzed descriptively. The table was organized by study, and where applicable, each study population was divided into subcohorts according to type of surgery. Patients from different studies were then pooled into groups based on surgical technique.
Surgical technique was classified according to the principle of the procedure; we grouped all intervelar veloplasty and palatoplasty techniques together as “straight line repair” (SLR), Z-plasty closure techniques as Furlow palatoplasty (FP), and pharyngeal procedures as pharyngeal flap (PF) or sphincter palatoplasty (SP) separately. Techniques were grouped accordingly to increase the power of pooled results, due to the small volume of studies that met our inclusion criteria. Where combination procedures were described these were grouped as “combination.” Combination procedures and sphincter pharyngoplasty were excluded from the final analysis due to small numbers.
The primary study outcome, proportion of patients recommended for secondary surgery was compared between groups based on surgical technique using a random-effects model. In this analysis, papers without specified recommendations for secondary surgery were excluded, as well as small groups based on surgical technique with a total n < 20 deemed too small to provide conclusive evidence, and study subcohorts with n < 5 patients being too small to contribute and resulting in potentially poor effect estimates. The proportion of patients with secondary surgery recommendation was calculated with 95% confidence intervals (CIs) and presented in a forest plot.
Improvement in speech was considered as a binary datum, with an improvement in speech achieved or not. The proportions of patients with improvement in the speech were added to the table, and the range was reported. The frequency of complications (postoperative fistula, obstructive sleep apnea (OSA), and hyponasality) was reported in the table and analyzed descriptively. Missing data were reported as not specified (NS) and omitted from the analysis.
Results
Fifteen manuscripts from the period 1954 to 2017 have been included in the final analysis, after a total of 419 studies were screened by 2 independent reviewers (Figure 1). Excluded articles were those that did not include speech outcomes or treated patients in adulthood. Studies that did not report treatment and outcome data separately for patients with syndromic SMCP were also excluded. Where combination techniques were used, these patients were also excluded from the analysis. The 15 studies report on 383 patients with nonsyndromic SMCP that were operated on in childhood, and 343 of these patients had follow-up data with secondary surgery recommendations where relevant.
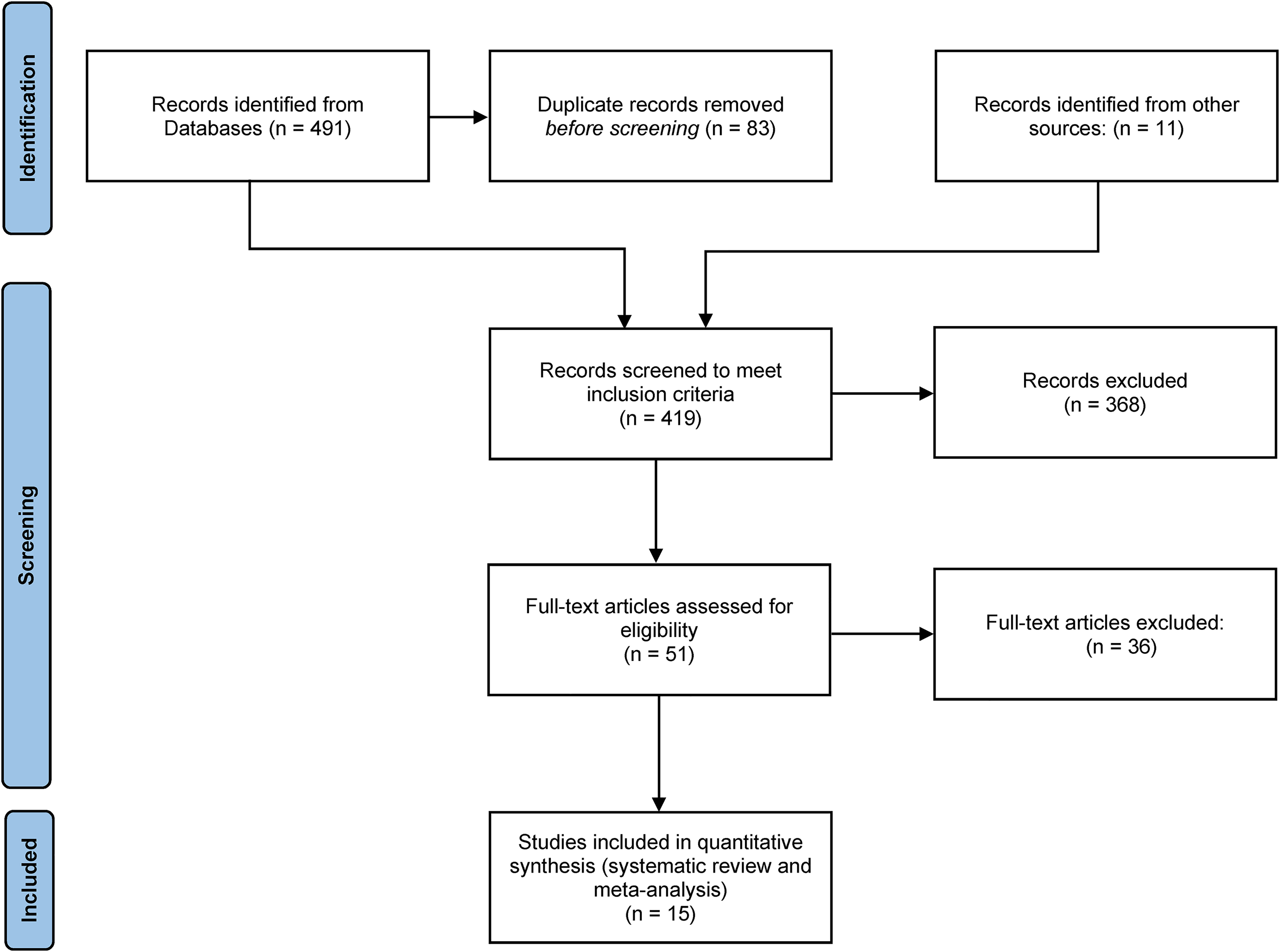
PRISMA flow diagram.
The 15 manuscripts included one randomized comparative trial, 4 comparative studies (one prospective and 3 retrospectives) with 2 to 6 different surgical techniques utilized, and 10 single cohort studies (2 prospectives, 8 retrospectives) reporting on one surgical technique each. The quality scores for the included manuscripts varied, with 8 manuscripts scoring less than 8. Three of these papers were published before 1988. A quality score of 8 or less is representative of low-quality data. Characteristics of the patient population and the outcomes specified have been summarized in Tables 1 and 2.
Characteristics of Included Studies.
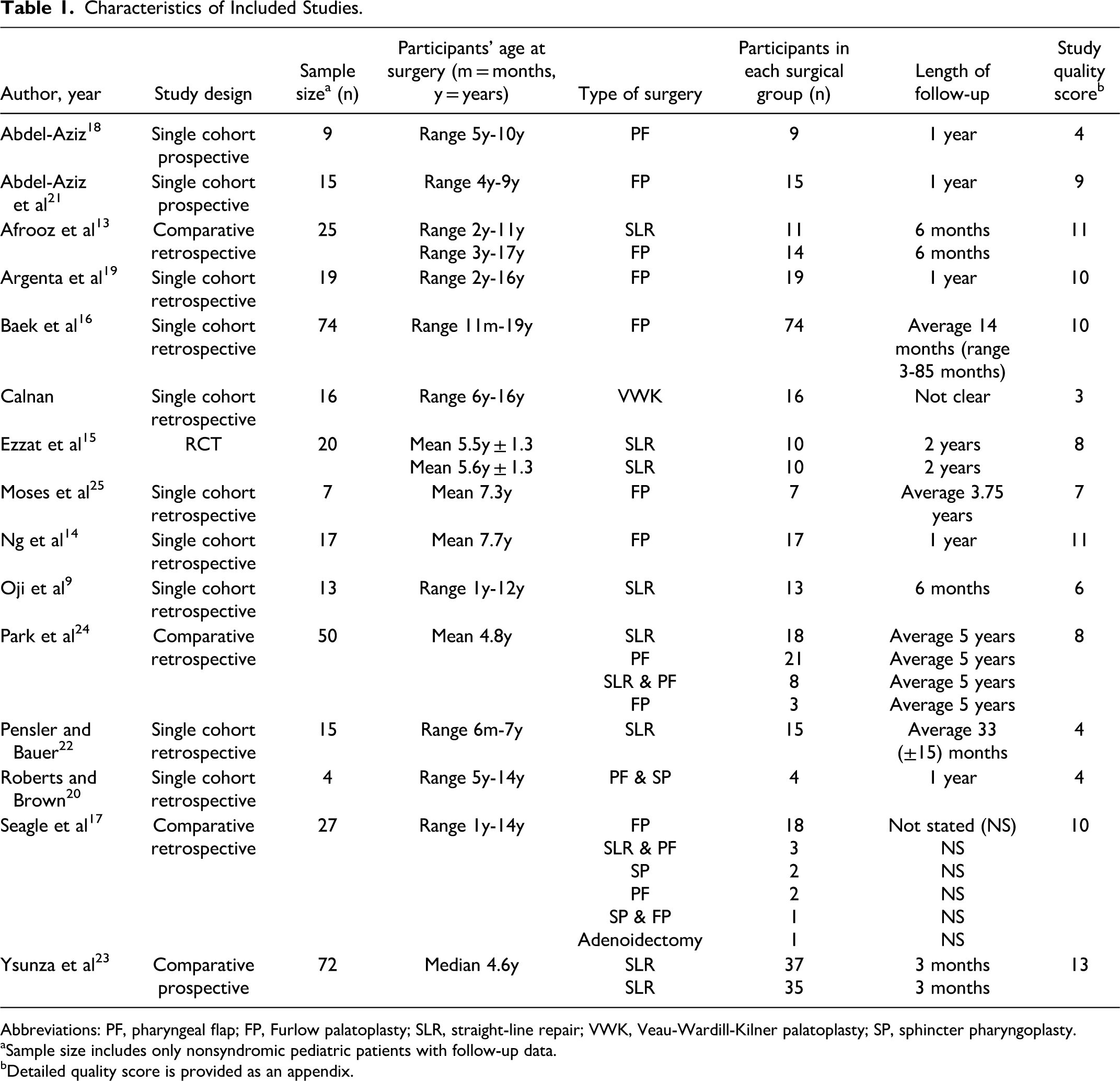
Abbreviations: PF, pharyngeal flap; FP, Furlow palatoplasty; SLR, straight-line repair; VWK, Veau-Wardill-Kilner palatoplasty; SP, sphincter pharyngoplasty.
aSample size includes only nonsyndromic pediatric patients with follow-up data.
bDetailed quality score is provided as an appendix.
Summary of Study Outcomes.
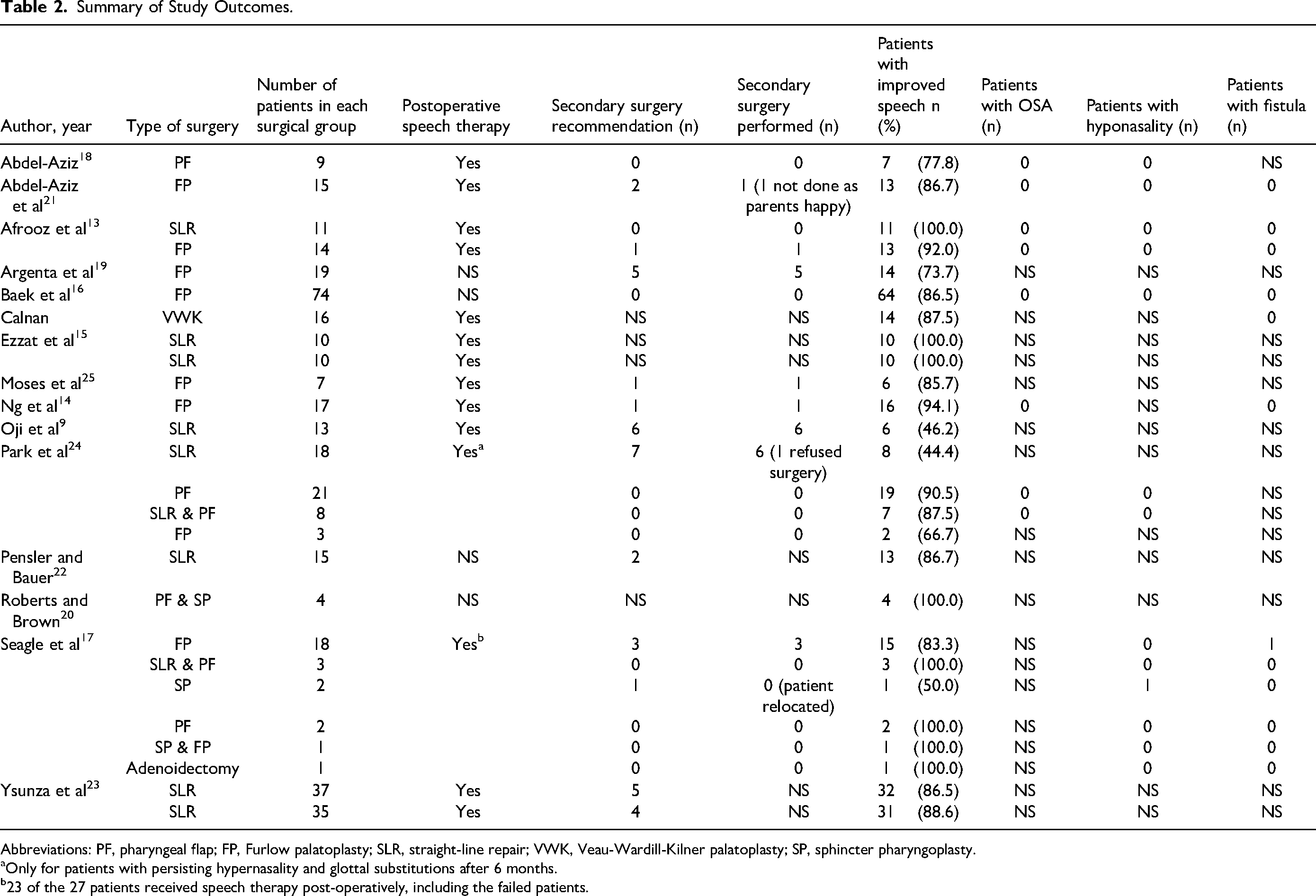
Abbreviations: PF, pharyngeal flap; FP, Furlow palatoplasty; SLR, straight-line repair; VWK, Veau-Wardill-Kilner palatoplasty; SP, sphincter pharyngoplasty.
aOnly for patients with persisting hypernasality and glottal substitutions after 6 months.
b23 of the 27 patients received speech therapy post-operatively, including the failed patients.
A number of speech assessment techniques were described; of these 73% of the studies (11 of 15) utilized a quantitative speech assessment technique. The range of quantitative assessment varied from perceptual assessment of resonance and nasalance scored on a sale of 1 to 4 with associated descriptors such as 1 “good” and 4 “poor,” 9 through to validated standardized scores such as the PWSS and GOS-SP.ASS.10,11 Perceptual speech assessment scores were used by 33% of the studies (5 of 15).
A random-effects model was used to estimate the proportions of secondary surgery recommendations with 95% CIs and the results are presented in a forest plot (Figure 2). The model showed the highest proportion of secondary surgery recommendation belonged to the SLR group, 17.8% (CI 8.9, 32.5), and the lowest proportion belonged to the PF group, 0.0% (CI 0.0, 100.0). However, there was no statistically significant difference between the surgical techniques in respect to the proportion of patients with recommendation for secondary surgery (P = .33). Our model demonstrated low heterogeneity (I2 = 11%), which was not statistically significant (P = .33).
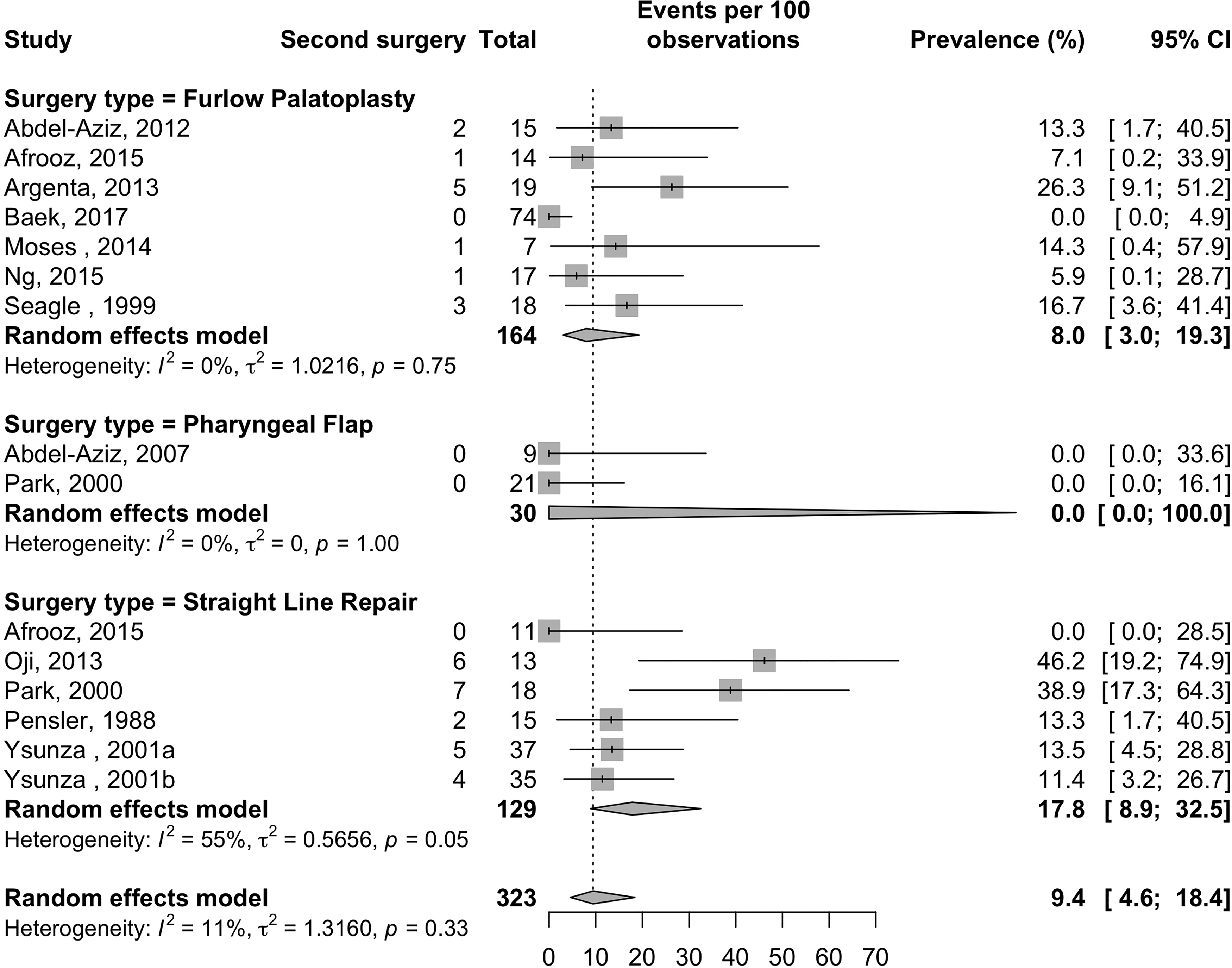
Forest plot: A random effects model of proportions of patients requiring secondary surgery, grouped by surgical technique.
Discussion
This systematic review was designed to further elucidate the question of which surgical technique offers the optimal outcome for SMCP-related VPI. Of 419 studies, only 15 met our inclusion criteria. A large number of articles were excluded due to our narrow inclusion criteria; 383 patients were identified, between 1954 and 2017, this was further reduced to 343 to account for insufficient follow-up data.
Surgical Technique, Outcomes, and Secondary Surgery
The most frequent surgical technique across this 63-year cohort remains the FP. The other 2 most common techniques are SLR and PF as primary techniques for SMCP. Overall speech improvement ranged from 44.4% to 100%, across 15 studies, with 10 studies recommending secondary surgery. The difference between surgical techniques was not statistically significant, but the reported rates of secondary surgery per surgical technique were notable with 0.0% for PF to 17.8% for SLR. The lack of difference detected may be due to underpowered group analysis. Although the SLR was the most frequently recommended for secondary surgery, PF numbers are small, and primary PF patient selection may be biased toward larger velopharyngeal (VP) gaps. Nonetheless, based on our analysis, PF certainly had the lowest (0%) rate of reoperation due to persistent VPI.
Speech Assessment
Perceptual speech assessment in these included studies was carried out by a highly trained speech therapist and further assisted by the use of scoring systems such as the GOS.SP.ASS and PWSS and Henningsson perceptual speech assessment.10–12 Adjuncts to these scoring systems include nasometry, nasendoscopy, and videofluoroscopy. The quality of the speech assessment ranged from a subjective assessment to an in-depth quantitative assessment with nasometry and/or validated qualitative speech assessment scores. However, standardized assessment between cleft centers is not established, and this introduces inherent bias in the quality of the data collected and therefore limits comparisons between techniques across multiple centers. 6 Gilleard et al recommended previously that SMCP-related VPI should be assessed with pre- and postoperative audio/video speech assessment on a validated standardized scale, pre- and postoperative nasalance scores, and lateral video fluoroscopy with gap size reported. The 4 papers published after this recommendation and included in our systematic review all utilized a standardized quantitative speech assessment score (PWSS 13 ; GOS-SP.ASS 14 ; PWSS 15 ; and Henningsson and hypernasality scores 16 ). Ultimately, outcomes will more easily be critically contrasted if cleft palate teams use a standardized and universally accepted speech evaluation tool.
Complications
Complications across the 16 papers were variably reported but overall low. Obstructive sleep apnea was not stated in the majority of papers (60%), of those reporting, there were no cases identified. Similarly, only one case of hyponasality was reported (SP group). 17 Fistula rates were also largely not stated (60%); only one case was identified (FP group). 17 As such, it is difficult to make any recommendations based on these data. Nonetheless, complications of the chosen technique need to be part of the decision calculus regarding which technique to select.
Indications for Specific Techniques
The studies included in our review variably reported on their indications for the technique chosen. A number provided no justification.2,9,13,18–20 Some authors changed from using a PF due to concerning rates of OSA.21,22 Some authors utilized videoflouroscopy or nasendoscopy to justify their chosen surgical technique.17,23,24 Others established the role for FP or had criteria for when FP was performed that included gap size.14,16,25
Gap size
Surgical technique choice may be directed by gap size.17,26 Some papers limit the use of FP to gaps less than 8 mm 17 ; however, of 15 studies, only 4 studies discuss gap size. Park et al selected PF where palatopharyngeal disproportion (a relatively short palate or a deep pharynx) were observed on cephalography or nasendoscopy, without measurements specifically provided. 24 Baek perfomed FP on patients that met 2 or more of their inclusion criteria including intermediate gap size defined as 50% to 80% closure of the closing gap on nasendoscopy. 16 Postoperative outcomes did not delineate between the gap sizes. 16 Ysunza et al did not find any significant difference between the 2 groups. 23 Ezzat et al reported on gap size pre- and postoperatively comparing radical IVV with radical IVV and palatoplasty 15 ; they found no difference between groups with gaps up to 10 mm addressed with these techniques. 15 Of these techniques, 20% had mild hypernasality with a maximum postoperative gap of 5 mm. Of this group of 2 there was no comment on requirement for secondary surgery. Seagle et al reported that gaps less than 8 mm treated with FP were more successful than those greater than 8 mm. 17 This group measured gap size in all patients and compared the outcomes across FP, PF, combined palatal pushback with PF, and finally SP. Of the 3 patients who had a failed FP, these were successfully treated with a combined palatal pushback with PF. 17 Unfortunately, the gap size was not determined across the other 13 papers; this measurement would assist objective decision-making for technique choice and may assist to predict which patients are best managed initially with a PF.
Age of repair
All children were repaired in childhood (up to 17 years of age). We were unable to identify a correlation of repair age with technique or with the outcome as these data were not reported in sufficient detail across the series included. Nonetheless, although we aimed to provide analysis on timing and technique, our data do suggest that a plain vanilla SLR or FP which both rely on functional levator muscles may well not be achieving outcomes similar to those children operated with overt cleft palate. What is clear is that these patients do not have their repair until a diagnosis is made, which further relies on a compliant patient to participate in a perceptual speech assessment. Ultimately, this late diagnosis and surgery well into the second or third year of life likely result in poorer outcomes for operations that rely on the levator's function. Although only 2 studies reported on PF, a 0% reoperation rate for persistent VPI is impressive.
Limitations
The limitations of this paper relate to the low quality of the studies which has resulted in an underpowered subgroup analysis. There were no randomized controlled trials but one randomized comparative study, while most studies were retrospective cohort studies. The speech assessment tools were heterogeneous, overall limiting quality meta-analysis of speech outcomes, and lacking in comprehensive use of standardized objective assessment. This further reiterates the work of Gilleard et al and Boyce et al.6,27
Conclusions
The goal of successful SMCP surgery is normal speech, ideally achieved at a single, uncomplicated operation. This systematic review and meta-analysis have demonstrated that the PF has the best outcome for first-line treatment of SMCP; however, this did not reach statistical significance, likely a function of the limited number of studies and case numbers meeting inclusion criteria. Delayed repair age inherent to SMCP may render operations that rely on a functional levator muscle with less favorable outcomes. Gap size, which is often used in the post-palatoplasty VPI population to guide treatment, would seem a logical objective measurement useful to guide surgical technique for SMCP, although the delayed timing of surgery in these patients may not hold this assumption true. The absence of standardized surgical techniques, speech outcomes, speech therapy, and assessment makes comparative analysis and recommendation difficult. We advocate for a standardized speech assessment tool to improve future quantitative assessment of SMCP surgery outcomes and a randomized or other controlled, standardized trial to better elucidate the preferred first-line technique, with speech outcomes and complication profiles key metrics.
Supplemental Material
sj-pdf-1-psg-10.1177_22925503221110066 - Supplemental material for What Technique Results in the Lowest Rate of Velopharyngeal Insufficiency in Patients With Submucous Cleft Palate? A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-psg-10.1177_22925503221110066 for What Technique Results in the Lowest Rate of Velopharyngeal Insufficiency in Patients With Submucous Cleft Palate? A Systematic Review and Meta-Analysis by Sarah Gardiner, MD, FRACS, Lindsay Bjornson, MD, MSc, Colleen Pawliuk, MLIS, Marija Bucevska, MD, Jeffrey Bone, MSc, and Jugpal S. Arneja, MD, MBA, FRCSC in Plastic Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed no receipt of financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.