
Abstract
Introduction
Conceptually, residency training is moving away from a fixed duration and toward an emphasis on the acquisition of knowledge and proficiencies.1–3 With the rise of competency-based medical education (CBME), residency has shifted to an outcome-centered approach, ensuring competency and development of core skills during residency through documentation and timely feedback.
This paradigm is now becoming the standard educational practice in North American post-graduate medical training. The Royal College of Physicians and Surgeons of Canada, in the footsteps of the American Accreditation Council for Graduate Medical Education, has begun implementing entrustable professional activities (EPAs), each with a set of milestones to assess residents’ progress in training. 4 These EPAs have been identified as the specialty-specific skills required for competency in future surgical practice.5–7
For the field of plastic surgery, a CBME curriculum has been implemented. A study by Knox et al identified key procedural competencies for plastic surgery residency training. 8 The study came to a consensus for 154 core, essential and 23 core, nonessential competencies. Notably, procedures such as cleft lip and palate repair have been identified as a key procedural competency but are not required as an EPA by the Royal College of Physicians and Surgeons of Canada. 9 Among these competencies, Canadian graduates reported feeling comfortable in all subdomains of plastic surgery with the exception of pediatrics. 10 Understandably, faculty must balance dueling responsibilities including patient care and resident education. It is unclear how rapidly or at what stage of training competency in pediatric plastic surgery might best be obtained, and whether resident competency in pediatric plastic surgery is due to a deficit in exposure or lack of involvement in pediatric cases. Therefore, the objective of this study was to determine the exposure of Canadian graduating residents to core pediatric procedural competencies and to identify the level of involvement in those cases.
Materials and Methods
We conducted a retrospective review of data collected over 10 years (July 1, 2004 to June 30, 2014) for all graduating Canadian residents with completion of at least 5 years of residency at any English-speaking accredited plastic surgery program. The institutions involved in this study included University of Alberta, University of British Colombia, University of Calgary, Dalhousie University, University of Manitoba, McGill University, McMaster University, University of Ottawa, University of Toronto, and University of Western Ontario. Institutions were kept anonymous throughout the study and analyses. All study procedures were approved by the appropriate Research Ethics Board. Exclusion criteria included case logs recorded by plastic surgery residents with less than 5 years of recorded case logs or less than a total of 300 case logs over 5 years. Non-plastic surgery, or what is known as “Off-Service” case log procedures, were also excluded. Program and individual data were anonymized throughout the analysis. As variation in procedure name exists between databases, case logs were coded according to the list of 8 Pediatric Core Procedural Competencies previously described by Knox et al. 8 These core competencies included cleft lip repair, cleft palate repair, setback otoplasty, hemangioma/vascular anomaly excision, congenital melanocytic nevi excision, dermoid cyst excision, syndactyly release and reconstruction, and polydactyly reconstruction.
The case logs of all Canadian plastic surgery programs are represented by 3 databases: T-Res (©Resilience Software), POWER—POstgraduate Web Evaluation and Registration (©Knowledge4YouCorporation), and New Innovations (©New Innovations, Inc). Data collected on each case log included: procedure name, diagnosis, date of procedure, academic year, program of resident, resident submitter, role resident played in procedure, and personal competence scores (Likert Scale from 1 to 5). As some fields differed between databases, level of involvement (resident role) and personal competence scores were combined: require further training/1, no equivalent/2, comfortable performing procedure under supervision/3, no equivalent/4, and comfortable performing procedure independently/5. Descriptive statistics, including mean, median, standard deviation, interquartile range (IQR), and percentiles, were used to summarize the data findings.
Results
Residency Program Volume and Variability
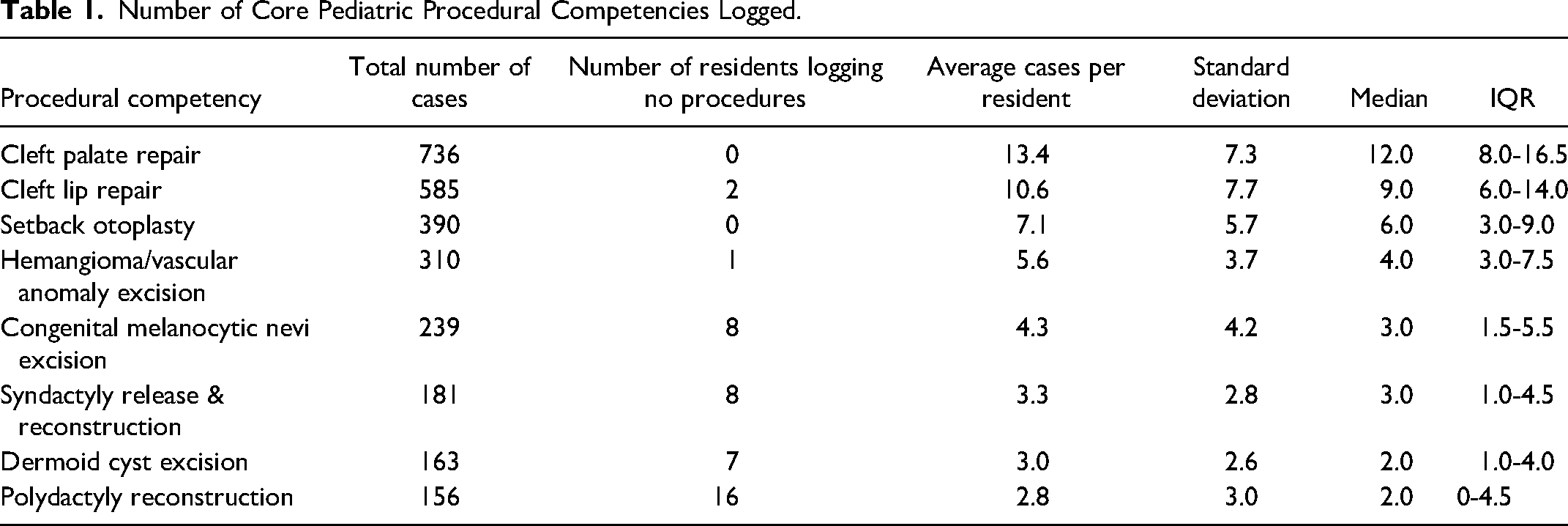
The total number of graduating residents was 55 with 59 405 logged cases. A total of 3061 logged cases (5.2%) were core pediatric procedures with an average of 55.6 ± 23.0 cases logged per resident. The average number of procedure-specific cases ranged from 13.4 ± 7.3 (median 12.0, IQR 8.0-16.5) for cleft palate repair to 2.8 ± 3.0 (median 2.0, IQR 0-4.5) for polydactyly reconstruction with large standard deviations across all procedures (Table 1). The top 3 most commonly logged procedures were cleft lip repair and cleft palate repair followed by setback otoplasty. The least common procedures consisted of dermoid cyst excision and syndactyly/polydactyly reconstruction (Table 1).
Number of Core Pediatric Procedural Competencies Logged.
The total number of logged cases increased in senior years with the most cases logged in postgraduate year (PGY) 3-5 (Table 2). A greater proportion of cases were logged as co-surgeon or surgeon in PGY3 (42%), PGY4 (40%), and PGY5 (62%) compared to junior years. The total number of logged cases per program varied widely with the most at 731 and least at 85 cases. However, most programs had a broad representation of core procedures (Figure 1).
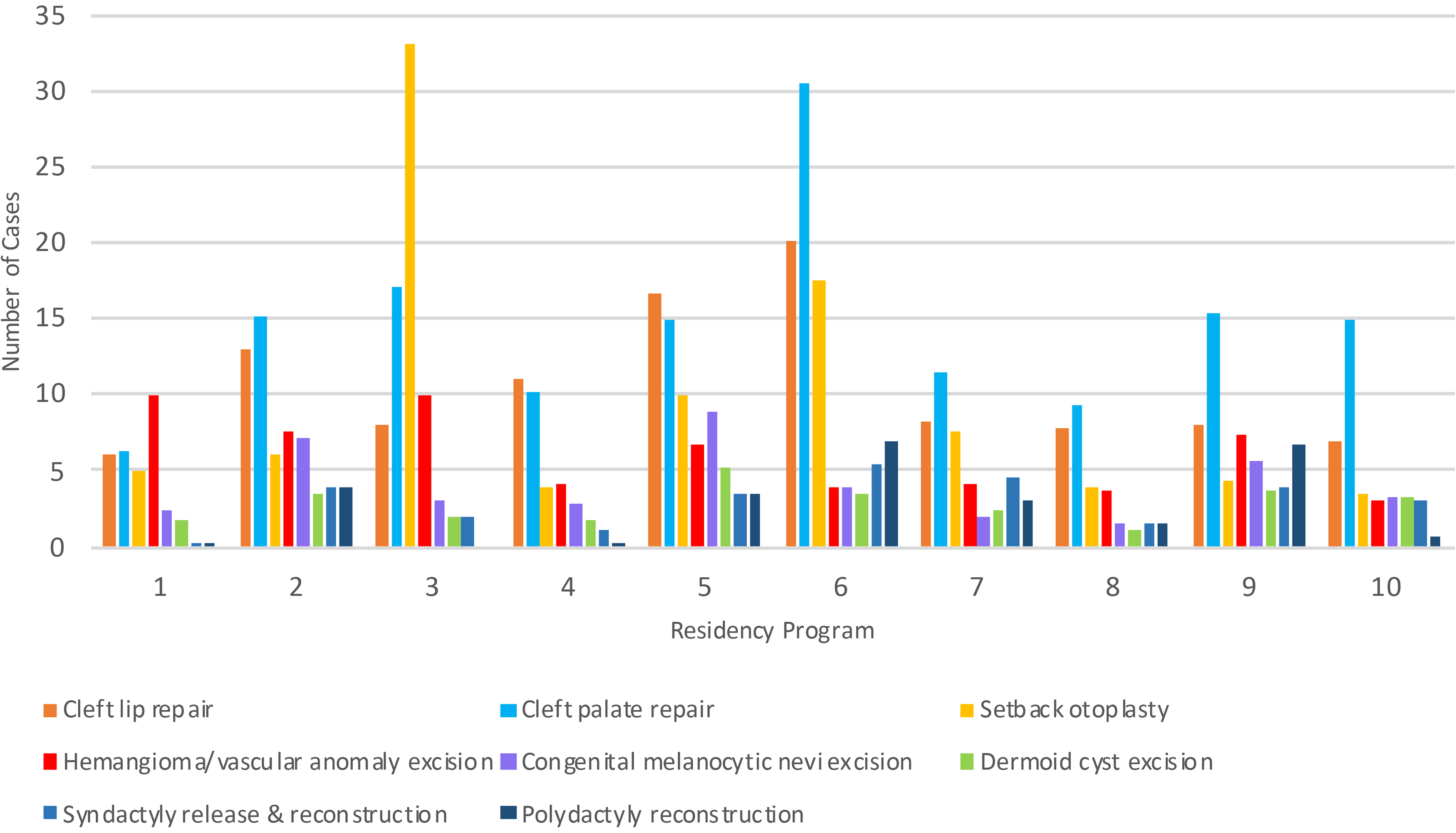
Number and type of pediatric cases logged by Canadian residency programs (anonymous).
Number of Pediatric Cases Logged by PGY Level and Role.

Resident Case Number and Role
For individual residents, there was a wide range of total cases logged even within the same program, with the highest and lowest number of cases being 114 and 12, respectively. Moreover, across all institutions, over 20% of residents had no cases logged as the primary surgeon with great variability in an identified role during cases, where residents most commonly identified as the assistant rather than surgeon or co-surgeon. Although high numbers of cleft lip and palate repairs were reported, residents were very rarely the primary surgeon and more commonly identified as student or first assist (Figure 2). Residents identified as the primary surgeon or co-surgeon more routinely for simple excisional procedures (Figure 3). Resident reported self-competency demonstrated that most residents felt comfortable performing cleft lip and palate procedures under supervision (3/5) rather than independently. However, residents were comfortable performing excisions of congenital melanocytic nevi independently (5/5) (Figure 4). Other procedural trends are less discernable.
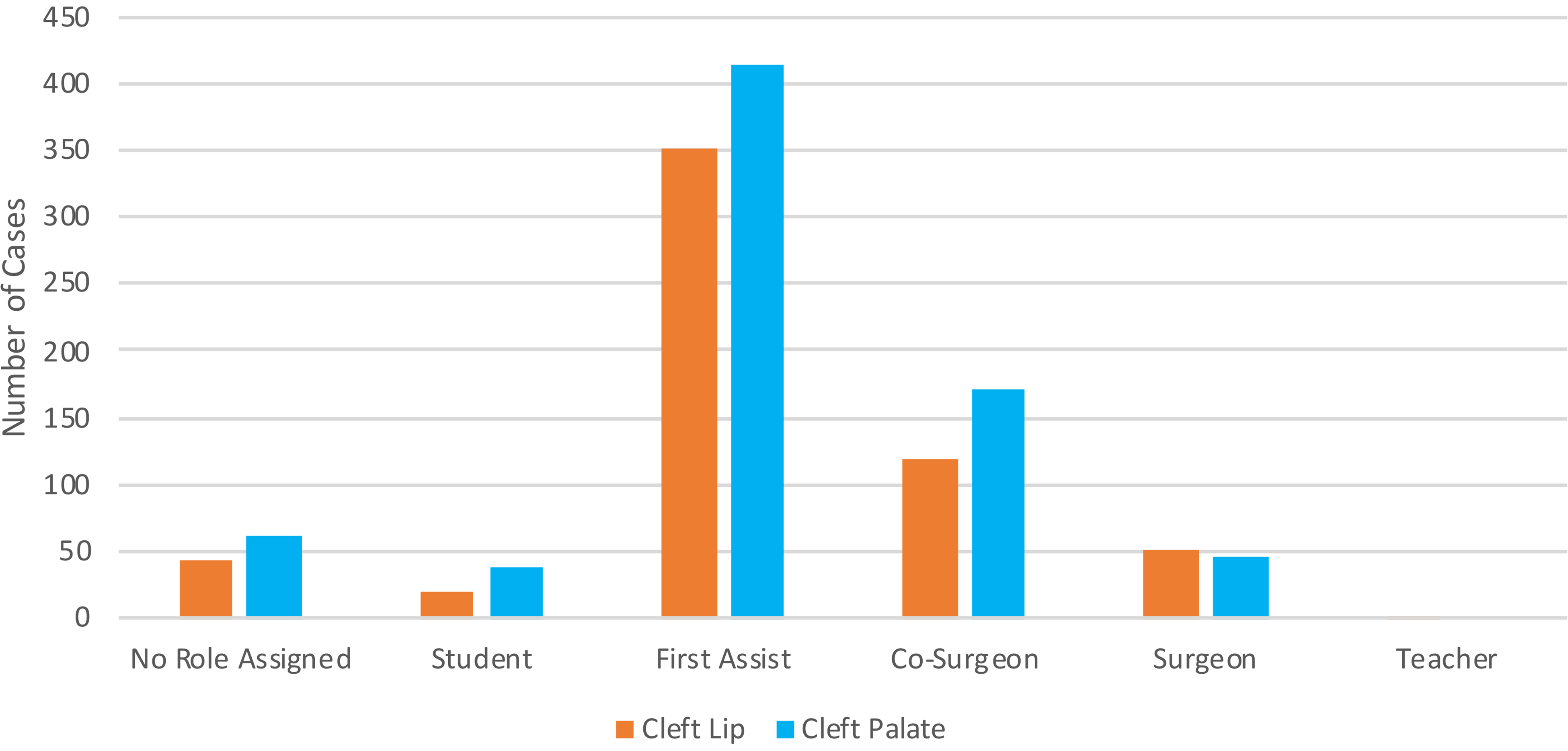
Resident role in cleft lip and palate cases.
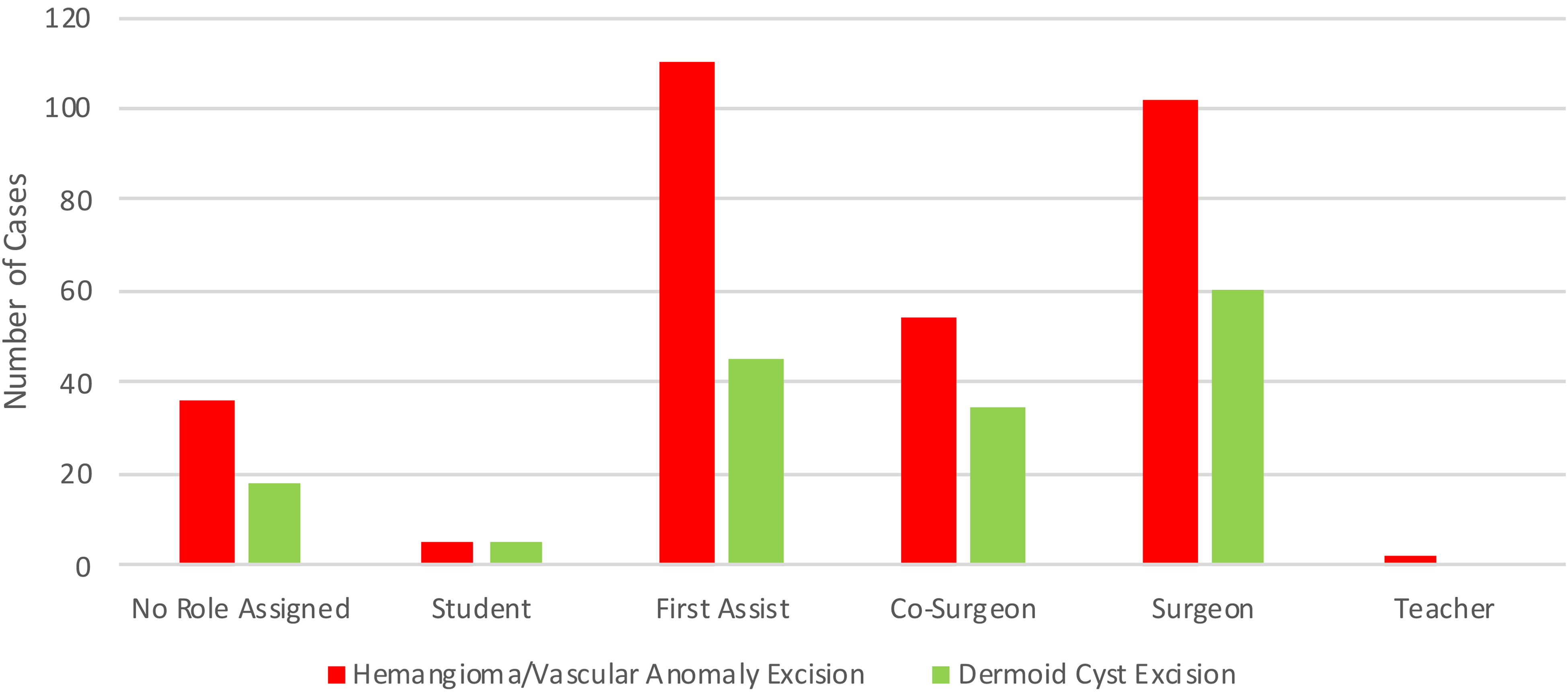
Resident role in minor excisions of hemangiomas/vascular anomalies and dermoid cysts.
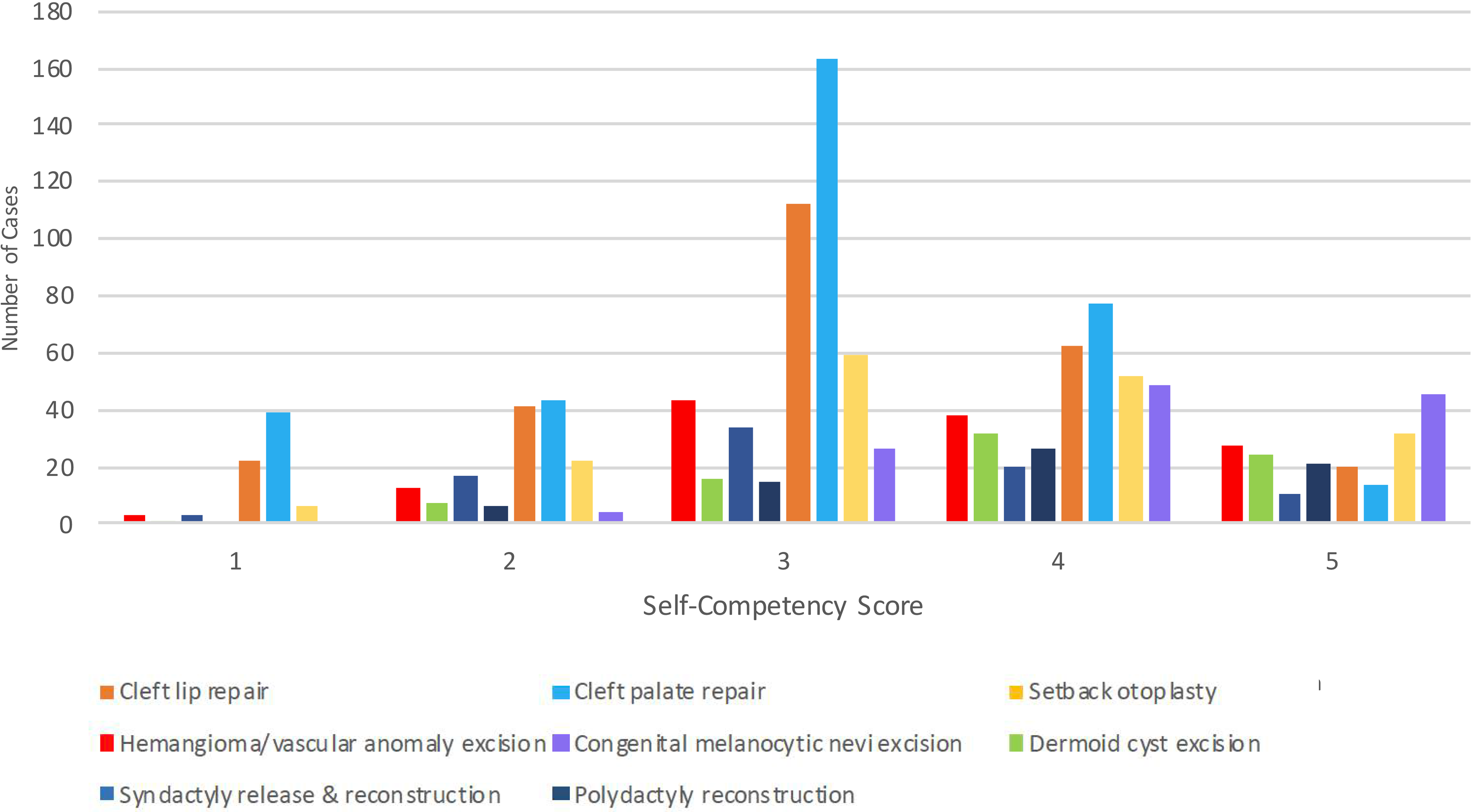
Resident self-competency score (Likert 1-5) across procedural competencies.
Discussion
Surgical residency programs have historically trained residents as apprentices. When ready (determined within their program to be competent) residents have taken externally administered written and oral examinations to assess knowledge and competency. 11 However, objective assessment of residents’ technical skills remains more elusive. Faculty typically assess residents’ characteristics, technical performance, and medical knowledge in order to entrust them with operative autonomy. 12 This involves a 3-phase process, including monitoring performance and “red flags,” assessing entrustability, and granting autonomy. 13
With the emergence of CBME, increasing efforts have been made to identify core activities within plastic surgery which can be entrusted to residents and assessed for competency. However, studies have demonstrated that residents have both adequate and inadequate exposure to various domains within the specialty.10,14 Approximately 63% of Canadian residents feel as though their role as a primary surgeon was inadequate throughout their training. 14 Largely, residents have the most exposure within the domains of hand and nonaesthetic breast. 10 However, when looking across all domains of plastic surgery and all levels of training, pediatrics had the fewest number of logged cases. 10
Few studies have investigated pediatric operative experiences of residents, specifically in plastic surgery. In the field of general surgery, 59% of residents felt inadequately prepared for their future practice. 15 Additionally, few Canadian and American residents gained experience in pediatric plastic surgery, compared to other pediatric surgical specialties 16 ; this seems to be a long-standing concern as these results were reported as far back as 1997. In our current study, resident exposure to core pediatric procedures was low overall with significant variation both within and across centers. High variability in plastic surgery training during residency has been noted in American institutions.17,18 Some of this variation may be due to differing amounts of time spent on pediatric rotations between programs.
Many pediatric core competencies are not being performed independently prior to graduation. Despite higher numbers of reported cleft lip and palate cases, residents most commonly identified as the assistant rather than surgeon or co-surgeon. There has been no clear number of procedures identified to determine competency; however, studies in other surgical specialties suggest a range of 20 to 50 cases.6,19–22 The average number of cases reported in our study was below this suggested range, which may explain in part why residents feel less confident in this domain of the specialty. Additionally, Podolsky et al 23 demonstrated that the number of simulated cleft palate repairs required to reach a minimum standard and maximum score were 6 and 16 sessions, respectively. Pediatric procedures are often “high stakes” as the first operation is the best operation, and the outcome will determine the patient's form and function for, perhaps, their whole life. As such, these may be complicated, or difficult to teach and learn; therefore, they are logical targets for surgical simulation.
In contrast, for simpler, more common procedures, residents were more likely to act as lead surgeon. Given that the skills required for excision of pediatric lesions may overlap with those identified in other domains, 8 residents may reach competency at a faster rate with less exposure. However, a significant limitation to achieving competency is the variability in how it is defined. 24 Some studies have defined competence as meeting assessment tool criteria,25,26 while others distinguish competency from mastery by time and experience. 27
Notwithstanding, residents’ apparent lack of comfort with pediatric procedures throughout residency, those that decide to pursue a career in pediatric plastic surgery typically complete additional fellowship training. It has been shown that both high case volume and craniofacial fellowship training have been shown to reduce complication rates.28–30 Although the expert panel of Canadian plastic surgeons, including both community and academic plastic surgeons, have identified both cleft lip and palate as Core Procedural Competencies, 8 it remains controversial whether these procedures require further fellowship training to achieve competence. Current Canadian Royal College EPAs do not require completion of cleft lip and/or palate repair, but rather an observation of the skill including, marking of a cleft lip and/or palate, demonstrating adequate soft tissue handling, performing complex layered closure and anatomical correction, and intra-oral suturing. 9 It may be possible with these guidelines for a trainee to meet their EPA requirements without participating as the primary surgeon. Nevertheless, if it remains imperative that residents are proficient in the identified core procedures by completion of their training, then current operative exposure should be supplemented with additional simulation-based training sessions on high-fidelity cleft lip and palate simulators.
There are several limitations to the current study. Firstly, our findings represent a snapshot of the current training environment. With the emergence of CBME the exposure to, participation in, and evaluation of competency for pediatric cases may change. Additionally, these data represent procedural logging before the COVID-19 pandemic and the integration of CBD curriculum. Our results are also dependent on the logging of cases by each respective resident. Despite case logs being mandated by each program, it is possible that residents may not accurately report their exposures thereby underestimating the number of cases. It is also possible that there is variability in residents’ definition of each intraoperative role. Finally, the number of logged cases does not necessarily represent competency itself; there is a need to combine case logs with assessment data to investigate this association.
These findings highlight a potential problem of limited resident exposure and a resultant gap in competency in the area of pediatric plastic surgery. Additionally, there may be a discrepancy between the expectations of the trainee and their exposure. Wide variation exists between Canadian institutions that may be due to differences in exposure, site volume, level of independence, and duration of pediatric rotations. It is also possible that the presence or absence of fellowship programs could improve resident exposure or not. In future studies, it may be beneficial to further assess these variables and correlate them with competence and resident role. Overall, fewer pediatric core competencies are performed independently compared to other plastic surgery domains. This may be an area that would benefit from further curriculum development and incorporation of surgical simulation.
Footnotes
Authors’ Note
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was waived by the research ethics board (Hospital for Sick Children, REB#1000046793).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.