
Abstract
The anatomic subunit approximation approach to unilateral cleft lip repair was developed over 20 years ago. While the underlying principles of the repair are unchanged, its description has been simplified, additional landmarks and creases have been added, and objective analysis of perioperative changes have provided better clarity regarding goals and desired alterations. We review recent insights regarding the deformity; describe the repair in a simplified manner; and link a stepwise approach to foundation-based primary rhinoplasty as a part of the avenue to creating nasolabial balance and harmony.
Introduction
The Deformity
Descriptions of the unilateral cleft lip and nose deformity have been based upon subjective observations that are prone to misperception 1 and optical illusion.2,3 While some models should be abandoned, others thread a common truth in which the severity of deformity can be explained by manifestations of the underlying pathology.
Clefting occurs along a spectrum in which mesenchymal penetration along embryologic lines of fusion fails. In the case of a unilateral cleft (Figure 1), uncoupled growth of the premaxilla 4 results in an anterior and lateral swing of the greater segment and retrusion of the lesser segment.5‐7 The overlying nasal base elements follow, with the septum, columella, and non-cleft alar base deviating lateral and the cleft alar base retruding posteriorly.1,3,5,7 The orthogonal vectors result in a “twist” deformity in which nasal arch forms (defined by the nostril rims and the oblique course of lower lateral and accessory chain of cartilages) collapse on the cleft side and become prominent on the non-cleft side1,5 (Figure 1).
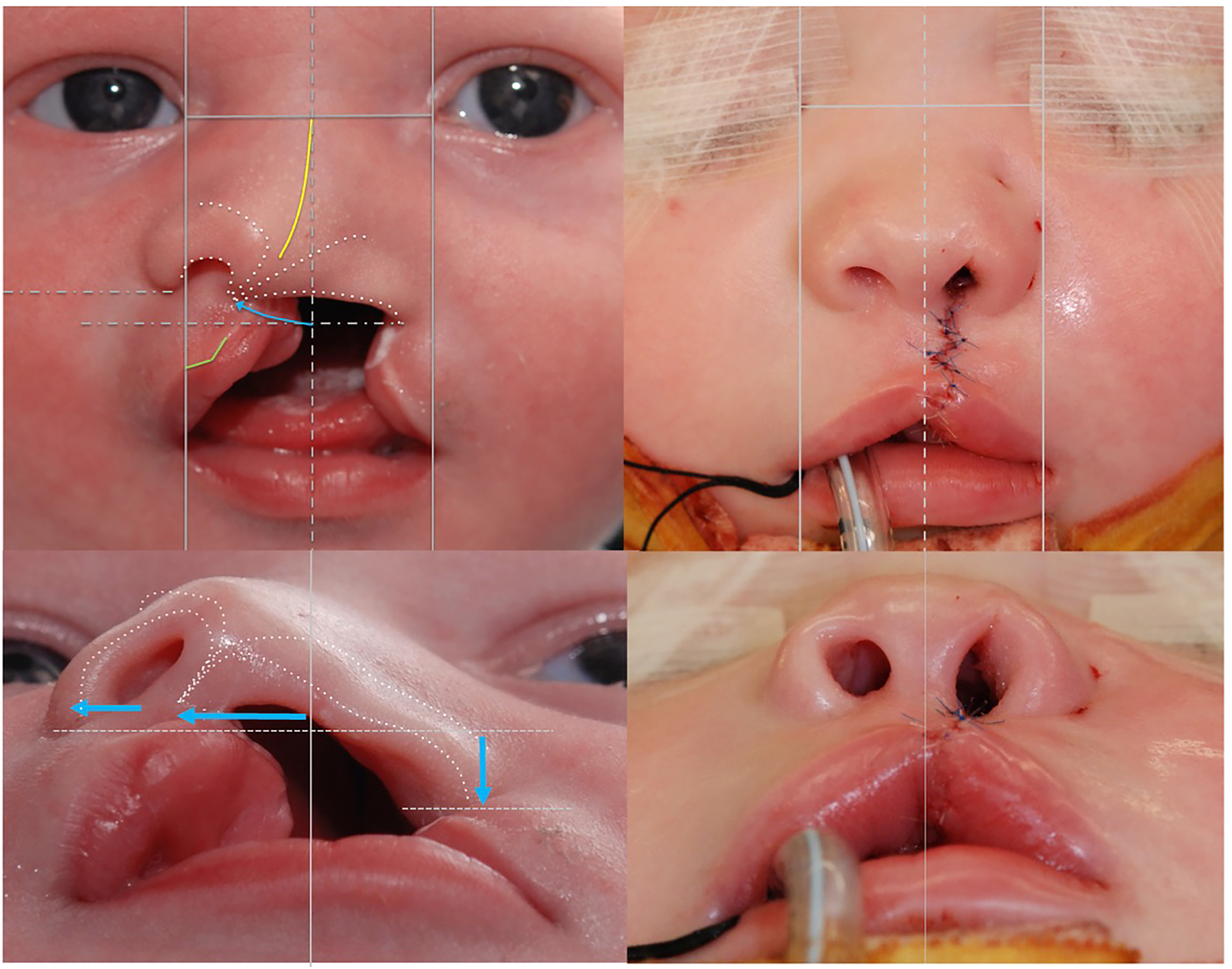
Primary unilateral cleft lip and nose deformity. (Left) Uncoupled premaxillary growth (curved blue arrow) pushes the non-cleft alar base and columella lateral and leaves the cleft alar base retruded. The twist alters the arch forms that define nasal form (white dotted lines) while distorting the septum (yellow) and displacing Cupid's bow (green). (Right) Balanced nasolabial form with the same reference frame. The columella and non-cleft alar base have advanced medial while the cleft alar base has advanced anteriorly. (Modified with permission from Tse RW, Ettinger RE, Sitzman TJ, Mercan E. Revisiting the unrepaired unilateral cleft lip and nasal deformity using 3D surface image analysis: a data-driven model and its implications. J Plast Reconstr Aesthet Surg. 2021;74:2694-704).
In addition to deformation, there is progressive tissue deficiency along the cleft such that the vermilion heights along the cleft are always short. When using current anthropometric definitions, the medial lip height is always lacking and the lateral lip height and width are variably undersized. 8
Principles of Treatment
Given that neither side of the cleft is normal, the non-cleft side should not be considered the ideal normal. 1 Non-cleft side structures and anatomic subunits change with surgical repair such that their form is only apparent after the cleft has been closed. The goals of treatment should therefore be to balance the opposing cleft and non-cleft side changes while producing natural 3D form and alignment. All anatomic subunits should be considered, including, mucosa, vermillion, cutaneous roll, philtral dimple, philtral column, nasal sill, medial footplate, and alar base.
The design for repair should utilize the available cleft and non-cleft anatomic landmarks to guide incisions through the spectrum of presentation.
Although placing scars along borders of anatomic subunits and minimizing tissue discard are important, they remain secondary to the production of minimizing 3D form and alignment. When the latter are achieved, prominence of a less ideal scar pattern tends to attract less attention, making the scar effectively “fade”.
Anatomic Subunit Approximation and its Modification
In simplifying the original repair 9 and acknowledging recent findings (Figure 2), the following changes have been made to the design: numbered points have been converted to anthropometric names, additional landmarks have been added, and nasal sill creases are used to guide landmark placement. In addition, stepwise surgical releases, critical checkpoints, and component reconstruction of the nose have been incorporated.
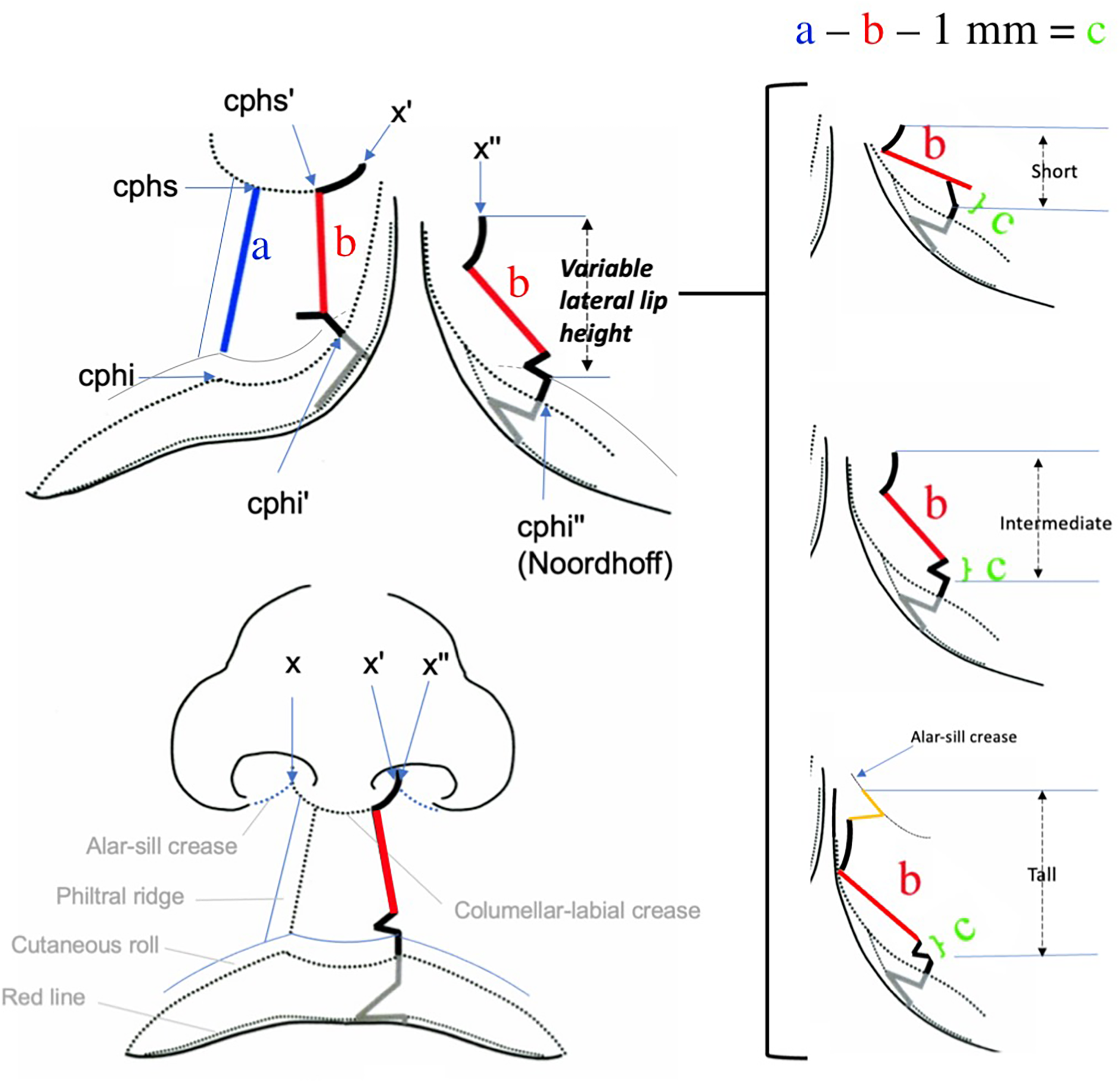
Anatomic subunit approximation. X’ and X” are points of nasal closure that are derived from landmarks and creases on the non-cleft side. Noordhoff point is considered a fixed anatomic landmark, thereby defining the lateral lip height. The lateral lip design will match the medial lip design and augment the medial lip as needed. The configuration of the lateral lip design varies according to the height defined between Noordhoff and point and X”. (Modified with permission from Fisher DM. Unilateral Cleft Lip Repair: An Anatomical Subunit Approximation Technique. Plast Reconstr Surg. 2005;116(1):61-71).
Planning
Marks are placed starting with midline and non-cleft side landmarks to facilitate identifying the corresponding (and less distinct) cleft side landmarks. The medial design does not vary and should be marked first. The lateral design needs to match the medial design and augment the medial deficiencies and is therefore marked afterward.
Lip Landmarks
The center of the columella (subnasale, sn) and non-cleft philtral height (crista philtra superioris, cphs) are identified along the nasolabial crease (Figure 3a). Notably, cphs is identified along the medial edge of the philtral column. The proposed height of the cleft philtral column incision (cphs’) is also identified along the nasolabial crease using the corresponding non-cleft landmark so that it is equidistant to subnasale.
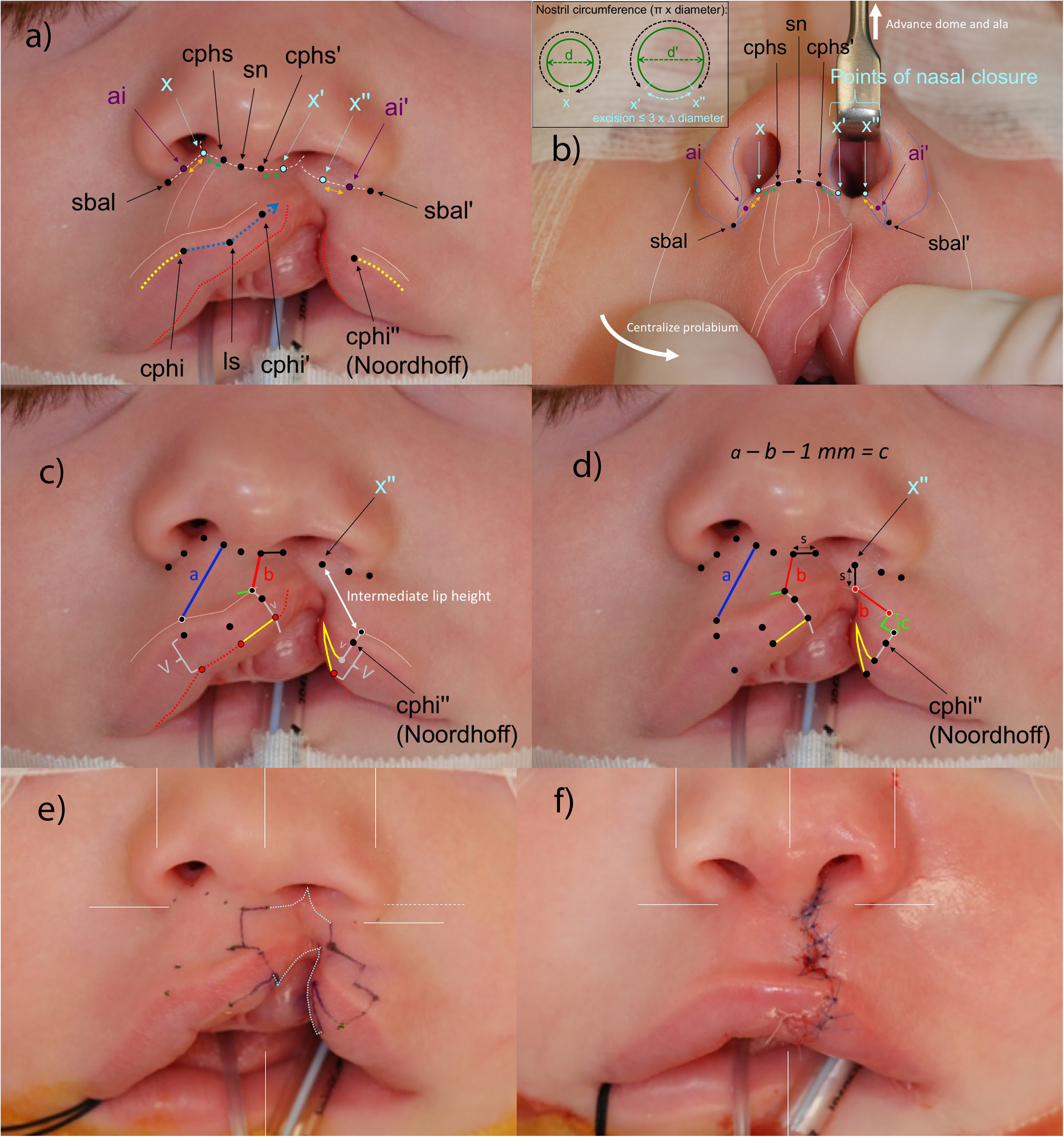
Landmarks. (a) The philtral column and labial cutaneous roll (vertical and horizontal white dotted lines) are considered distinct anatomic subunits. The height of the philtral column is defined along the medial border of its prominence. The corresponding Cupid's bow peak is defined at the junction of the straight (blue) and convex (yellow) part of the peak. X is defined on the non-cleft side at the intersection of columellar-sill crease and alar-sill creases (white dashed lines). The points of nasal closure, X’ and X” on the cleft side are defined along the same creases, using the other landmarks to define their location (green and orange arrows). The vermilion-mucosal junction is marked as a red line. (b) Nasal base landmarks should be symmetric in position and configuration when the deformity is manually corrected. The points of nasal closure can then be confirmed. The excision between those points can be verified when the nasal floor is intact by measuring relative differences in nostril size. (c) Corresponding labial landmarks are placed above the cutaneous roll (black dot with white outline) and along the vermilion-mucosal junction (red dot with black outline). The deficient medial lip vermilion height is transposed to the vermilion below Noordhoff point. The remaining vermilion height defines the base of the vermilion flap. (d) The lateral lip design needs to span or fit into the height between the lateral point of nasal closure and the landmark above the cutaneous roll at Noordhoff. (e) Incisions to connect the two sides. (f) Immediately following repair (Modified with permission from Tse R, Lien S. Unilateral Cleft Lip Repair Using the Anatomical Subunit Approximation: Modifications and Analysis of Early Results in 100 Consecutive Cases. Plast Reconstr Surg. 2015;136(1):119-130).
Cupid's bow is identified along the vermilion border (Figure 3a). The low-point (labiale superioris, ls) can be confirmed by tracing the frenulum from the gingiva and the non-cleft peak (crista philtri inferioris, cphi) is identified where the straight portion of the bow meets the gentle convex curve (corresponding to the medial border of the philtral ridge). The cleft side peak (cphi’) tends to be indistinct but can be marked equidistant to the center of the bow. On the lateral lip, Noordhoff point is identified along the vermilion border, at the site where the vermilion-mucosal junction starts to converge with the vermilion border. 10 Lateral to this point, the cutaneous roll is normal, whereas medially, the roll becomes less distinct. Corresponding landmarks to each point along the vermilion border are identified above the cutaneous roll and along the vermilion-mucosal junction.
Nose Landmarks
Subalare (sbal) is the lowest point along the ala-sill crease and the alar insertion point (ai) is the intersection of the alar rim and the ala-sill crease (Figure 3b). Those landmarks are identified on both sides with the lip and nose in their anticipated/corrected form (non-cleft alar base and columella centralized, cleft alar base advanced anteriorly, and cleft side dome supported with a retractor) so that the configuration of landmarks from the submental view are symmetric. When the lip and nose are at rest (ie, lip elements are allowed to splay and nose is left to collapse), the configuration of those landmarks will appear asymmetric (Figure 3a).
On the non-cleft side, the ala-sill crease is followed or projected into the nasal floor while the nasolabial crease is followed as it continues along the medial footplate (Figure 3b). The intersection of these creases, which is sometimes at the base of a valley, is marked (X). Corresponding landmarks are defined on the cleft side along the respective creases so that they mirror the non-cleft side relationships. These points of nasal closure (X’ and X’’) are critical to the repair. When X’ and X” are brought together, the desired nasal correction should be produced. The surgeon should take time to verify that this is the case and to carefully make any adjustments so that the configuration of nasal base elements is symmetric along all axes. If there is uncertainty, a preliminary release of the alar base can help facilitate landmarking. Particular attention should be made to ensure that the superior–inferior relationship of alar base position is appropriate given that malposition is difficult to correct.
If the nasal floor is intact (i.e. less severe clefts) the points of nasal floor closure can be further verified by measuring nostril circumferences using urethral sounds (Figure 3b). The nasal floor excision (X’ to X’’) should not exceed the difference in circumferences (approximately 3 × the difference in nostril diameter) to avoid producing a micronostril.
Medial lip Design
The design simply “connects the dots” (Figure 3c) along nasal sill (X’-cphs’), philtral column (cphs’-cphi’), and across the cutaneous roll, vermilion border, and vermilion-cutanous junction (at cphi’). The latter is perpendicular to the lip so that its incidence with the philtral column incision (cphs’-cphi’) forms an angle that will open once incised (Rose-Thompson effect).
A small opening incision is designed above the cutaneous roll and oriented perpendicular to the philtral column incision to maximize the vertical release. It will be filled by an equilateral triangle from the lateral lip, if needed, to augment medial lip height. Another incision is designed along the vermilion-mucosal junction so that the deficient vermilion can be augmented by a lateral vermilion flap.
Lateral lip Design
The medial lip vermilion height (at cphi’) is almost always deficient whereas the vermilion height at Noordhoff point (cphi”) is similar to that at Cupid's bow peak on the non-cleft side (cphi). The vermilion height at cphi’ is therefore transposed to the lateral lip so that the remainder of the vermilion height at Noordhoff point serves as the base of a triangle that will augment the medial vermilion (Figure 3c).
The medial lip cutaneous height is always deficient and needs to be augmented. Elongation is produced by the Rose-Thompson effect (diamond-shaped excision with vertical closure) and is estimated at 1 mm. If a lateral lip triangle flap is needed, the base width, c, is estimated as a – b – 1 mm; where “a – b” is the difference in philtral heights (Figure 2). Of critical importance in the design is to measure the non-cleft height, a, at rest and the cleft philtral height, b, with downward traction to unfurl the lip. Failure to do so can result in overcorrection producing a “long lip” that is too tall.
Thus far, the design has only involved identifying landmarks. The remaining lateral lip design requires more visual-spatial anticipation given that the lateral lip height can vary, ranging from short to excessively tall (Figure 2).
The lateral point of nasal closure (X’’) and the superior edge of the cutaneous roll at Noordhoff point (cphi’’) define the space (Figure 3c) in which lateral lip markings need to match the medial lip incisions, and augment the medial lip as needed. The 3 limbs include the nasal sill, s; the philtral height, b; and the inferior triangle, with base width of c. Depending upon the presentation, the limbs can articulate open and closed with one another to accommodate the space.
When the lateral lip is short (ie, complete clefts) the angles between the limbs will be made more acute (Figure 2). The philtral height incision will be more horizontal, and its lateral extreme may need to be coincident with the upper incision of the inferior triangle (Figure 4).
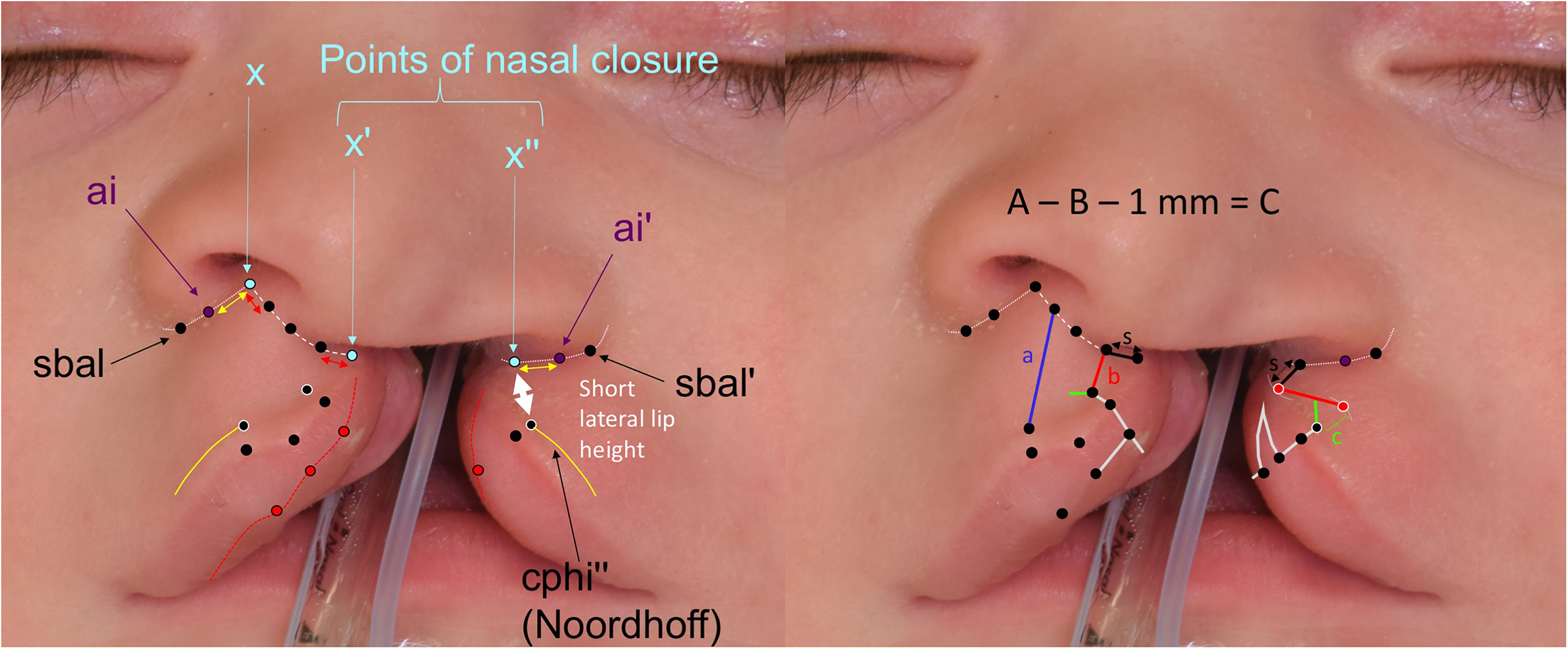
Case example, wide complete cleft with short lateral lip height. The appearance and configuration of landmarks should be symmetric when the lip and nose are in their corrected form and position. Due to the constricted non-cleft nostril, the cphs-x distance was small, making the cphs’-x” limb short and necessitating a short s limb (sill) to be incorporated into the lateral lip design. The short limb helps because the lateral lip height is extremely limited. The border of the inferior triangle and the b limb (cleft philtral height) on the lateral lip are made coincident so that they can fit into the space. (Reproduced with permission from Tse RW, Fisher DM. Anatomic subunit approximation to unilateral cleft lip repair. In: Neligan P, ed. Plastic Surgery, fifth edition. Elsevier. In print).
When the lateral lip is intermediate in height (ie, complete cleft with Simonart band and some incomplete clefts), the philtral height incision will be more vertical, and the inferior triangle will have a more horizontal pointing orientation (Figure 2). The angle between the nasal sill and philtral height limbs should be made to match the angle between these 2 limbs on the medial lip (Figure 3d).
When the lateral lip is excessively tall (ie, incomplete and minor form clefts), a vertical wedge excision is incorporated so that the lateral lip design can match the medial lip design (Figure 2). A common mistake is to open the angle between the nasal sill and philtral height incisions to accommodate the excessive lateral lip height. This produces an overly obtuse configuration that does not match the angles between limbs of the medial lip incision, resulting in distortion of anatomic subunit contours upon inset and potentially driving the cleft alar base superiorly into a malpositioned configuration. The latter is a critical problem that does not have a reliable secondary remedy. Incorporating a wedge excision of the upper lip in the design mitigates these issues. Starting from the lateral point of nasal closure (X’’), the upper edge of excision is designed along the ala-sill crease with its apex extending up to subalare (Figure 2). The lateral lip markings are designed starting from the cutaneous roll above Noordhoff point (cphi”) so that the limbs match the configuration on the medial lip. The upper extent of these markings then becomes the lower edge of excision that removes the vertical excess. Although there may be reluctance to commit to excision, there are several ways to confirm that the lateral lip height is excessive (Figure 5). First, the vertical position of Noordhooff point (cphi’’) may be lower than the non-cleft Cupid's bow peak (cphi). Second, the cleft lateral lip height (cphi’’-sbal’) is equal or greater than the non-cleft lateral lip height (cphi-sbal). Third, and most important, the angle between the nasal sill and the philtral height limbs does not match that of the medial lip markings.
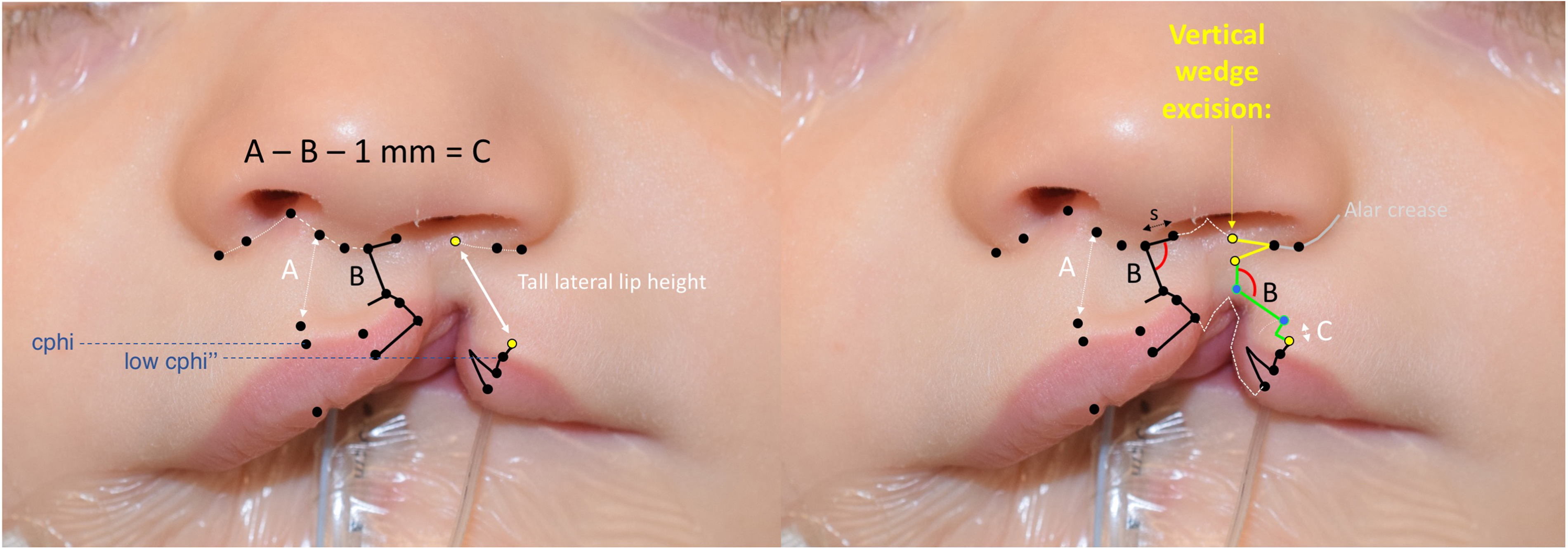
Case example, incomplete cleft with excessive lateral lip height. Most incomplete clefts require vertical wedge excision (yellow lines). The tall lateral lip height and relatively low cphi” position (blue lines) provide an indication that excision is needed. Ultimately, the angle between s limb (sill) and b limb (greater lip height) on the lateral lip should match that on the medial lip to avoid distortion of the closure along the borders of anatomic subunits (red arcs). (Reproduced with permission from Tse RW, Fisher DM. Anatomic subunit approximation to unilateral cleft lip repair. In: Neligan P, ed. Plastic Surgery, fifth edition. Elsevier. In print).
Connecting the 2 Sides
When a nasal floor is present (ie, incomplete clefts and some complete clefts with Simonart band), a wedge excision is designed to apices within the nasal floor and toward the alveolus (Figure 3e). When the nasal floor is absent (ie, complete cleft) or diminutive (some complete clefts with Simonart band), incisions from the points of nostril closure (X’ and X’’) extend intranasally along the cleft margins for closure of the nasal floor.
Lip mucosal incisions on either side of the cleft extend to the alveolus for eventual approximation. In all cases, a stepwise approach to tissue mobilization is as described further.
Repair: Surgical Release and Component Reconstruction
Designed incision lines will wash off as surgery progresses so points are imprinted by ink and needle.
Lip Release and Remeasure
Medial lip is always first (Figure 6). Incisions are made with a scalpel and excision of marginal tissue is completed with scissors. Emphasis is placed on making a clean incision across the cutaneous roll so that later alignment upon repair produces a seamless contour. An acute angle between the philtral height incision, b, and the incision that traverses cutaneous roll and vermilion is also emphasized to maximize the Rose-Thompson effect.
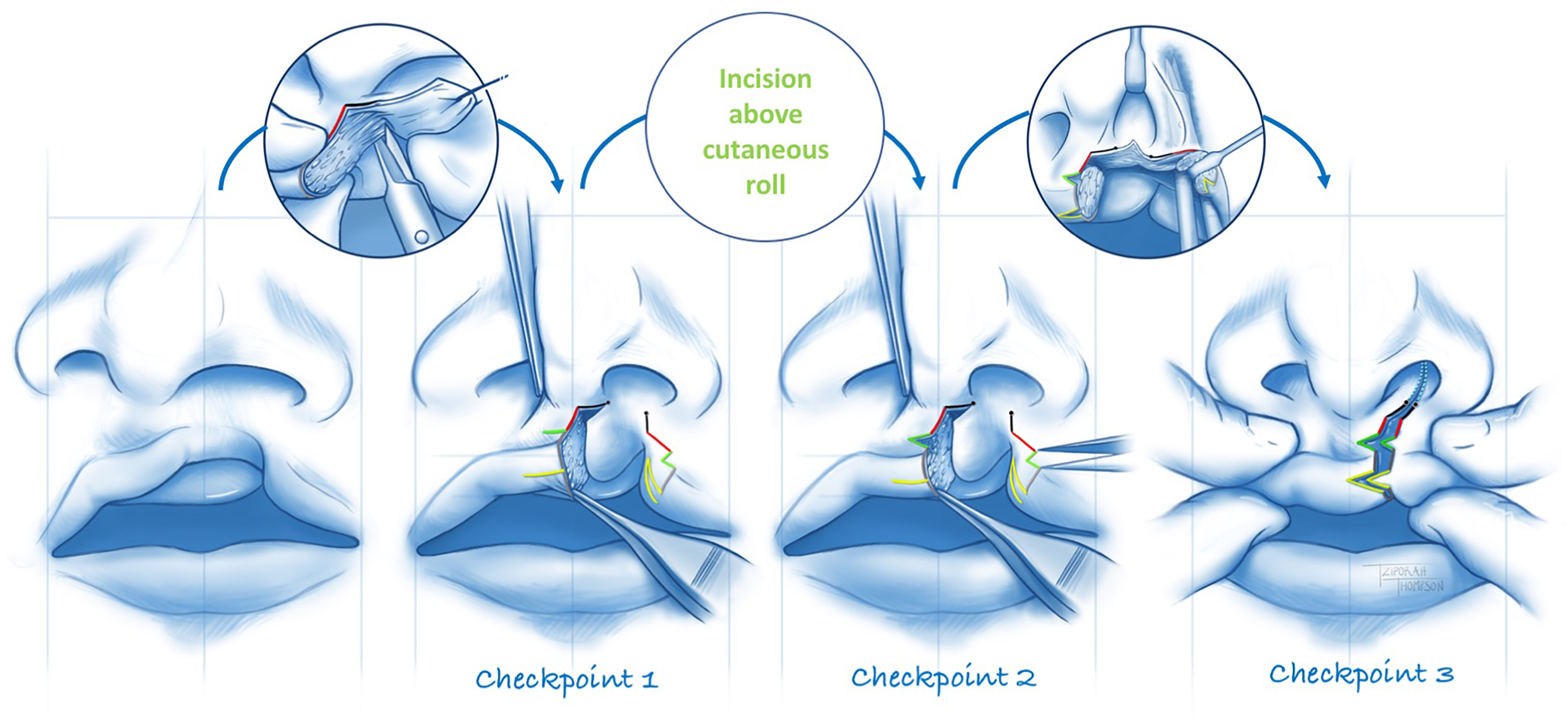
Sequence and Checkpoints. (1) The medial lip is incised and muscle dissected first so that the need for the releasing incision above the cutaneous roll can be verified. (2) Once the releasing incision has been made, the Cupid's bow is leveled so that the size of the defect can be measured and the lateral lip design verified. (3) The points of nasal closure should be verified prior to incision and after lateral tissue releases. Approximating these points should produce the desired nasal correction and if not, they should be revised.
Orbicularis muscle is then dissected from skin and mucosa and released from the alveolus (Figure 7), thereby producing an empty space under the columella (as the lip rotates downward). Dissection between muscle and skinalong the philtrum is minimal as to preserve the philtral dimple while still allowing eventual placement of sutures.
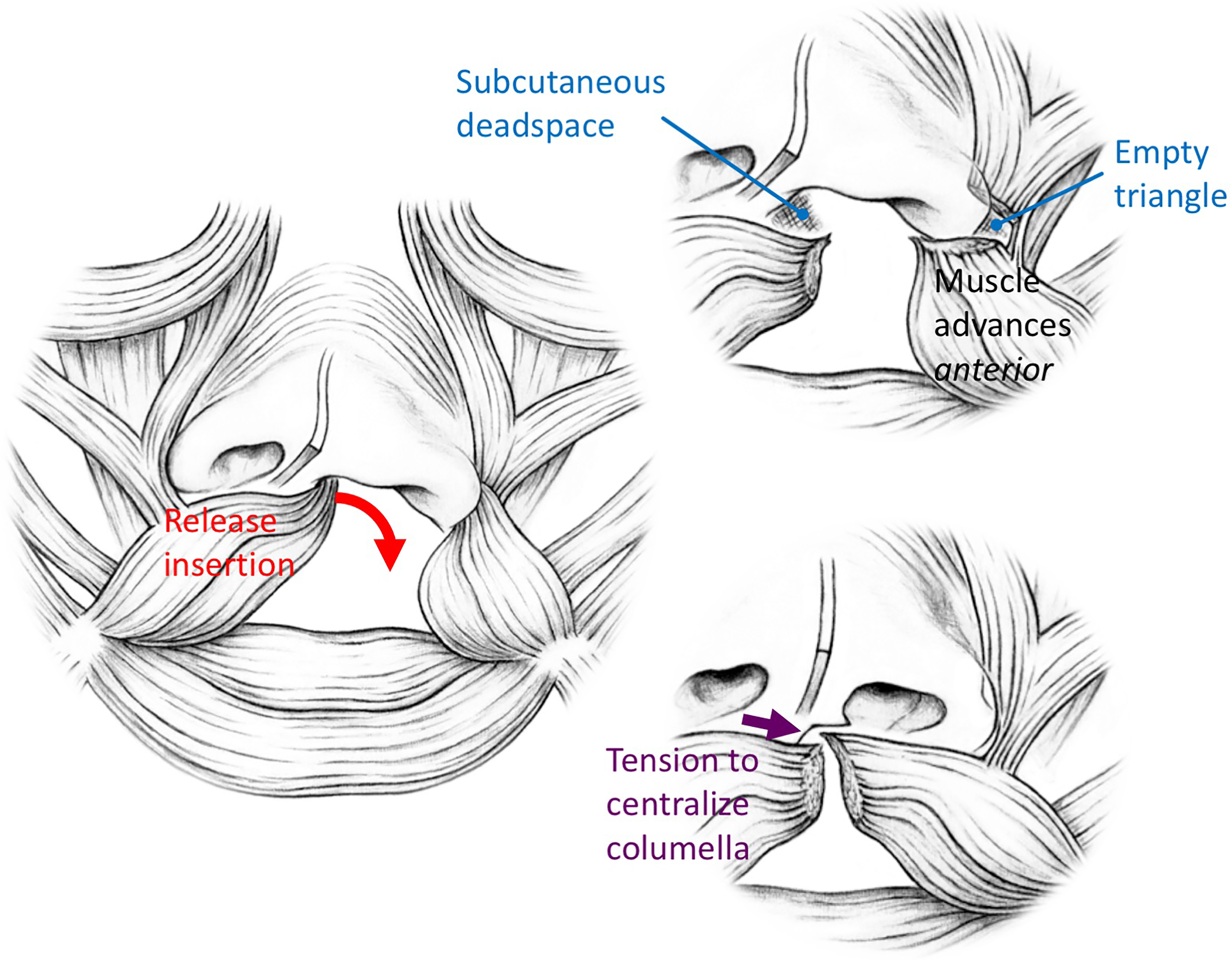
Muscle dissection and repair. The muscle is delaminated under the columella and released from the premaxilla so that the medial lip can drop down. Lateral muscle dissection is more aggressive with the release from maxilla extending beyond the ala. This produces an “empty triangle” that contains no muscle. The lateral muscle fills the dead space under the columella. While the lateral muscle is drawn anteriorly, tension of the repair draws the columella and non-cleft alar base toward midline. (Modified with permission from Tse RW, Mercan E, Fisher DM, Hopper RA, Birgfeld CB, Gruss JS. Unilateral Cleft Lip Nasal Deformity: Foundation-Based Approach to Primary Rhinoplasty. Plast Reconstr Surg. 2019;144(5):1138-1149).
CHECKPOINT 1 is to verify whether the opening incision above the cutaneous roll is needed (Figure 6). If Cupid's bow can be leveled with the columella centralized and gentle downward traction on the lip, the release is not needed and the lateral lip design is adjusted accordingly. Otherwise the incision is made through the skin.
CHECKPOINT 2 is to verify whether the lateral lip inferior triangle needs to be adjusted (Figure 6). With the columella centralized and Cupid's bow leveled, the defect above the cutaneous roll is measured and the lateral lip design is verified. If there is any discrepancy, the size of the inferior triangle can be redrawn such that it exactly matches the size of the opening defect required to level the bow.
CHECKPOINT 3 is to verify the points of nasal closure before committing to the lateral lip incisions (Figure 6). When approximating these points, balanced nostril circumferences and alar base positions should be achieved. If not, the lateral point of nasal closure can be revised. If there is any doubt, mobilization of the cleft alar base (ie, upper sulcus incision and anterior maxilla/piriform release) can facilitate this assessment.
Once all 3 checkpoints have been verified, the lateral lip incision is made. Orbicularis is dissected from skin and mucosa and released from the alveolus. The latter release continues beyond the alar base so that an “empty triangle” of muscle is produced (Figure 7). If further mobilization of the lateral lip is needed, an upper buccal sulcus incision is made.
Stepwise Reconstruction of the Nasal Foundation11
The medial lip incision provides access to the caudal septum (Figure 8). If the septum is visible in the non-cleft nasal airway when the columella has been centralized, it is relocated. The caudal septum is released from the anterior nasal spine and mobilized to the midline of the face. This may involve a subperichondral dissection of the septum on the non-cleft surface or a superiosteal dissection and release along the floor of the non-cleft nostril.
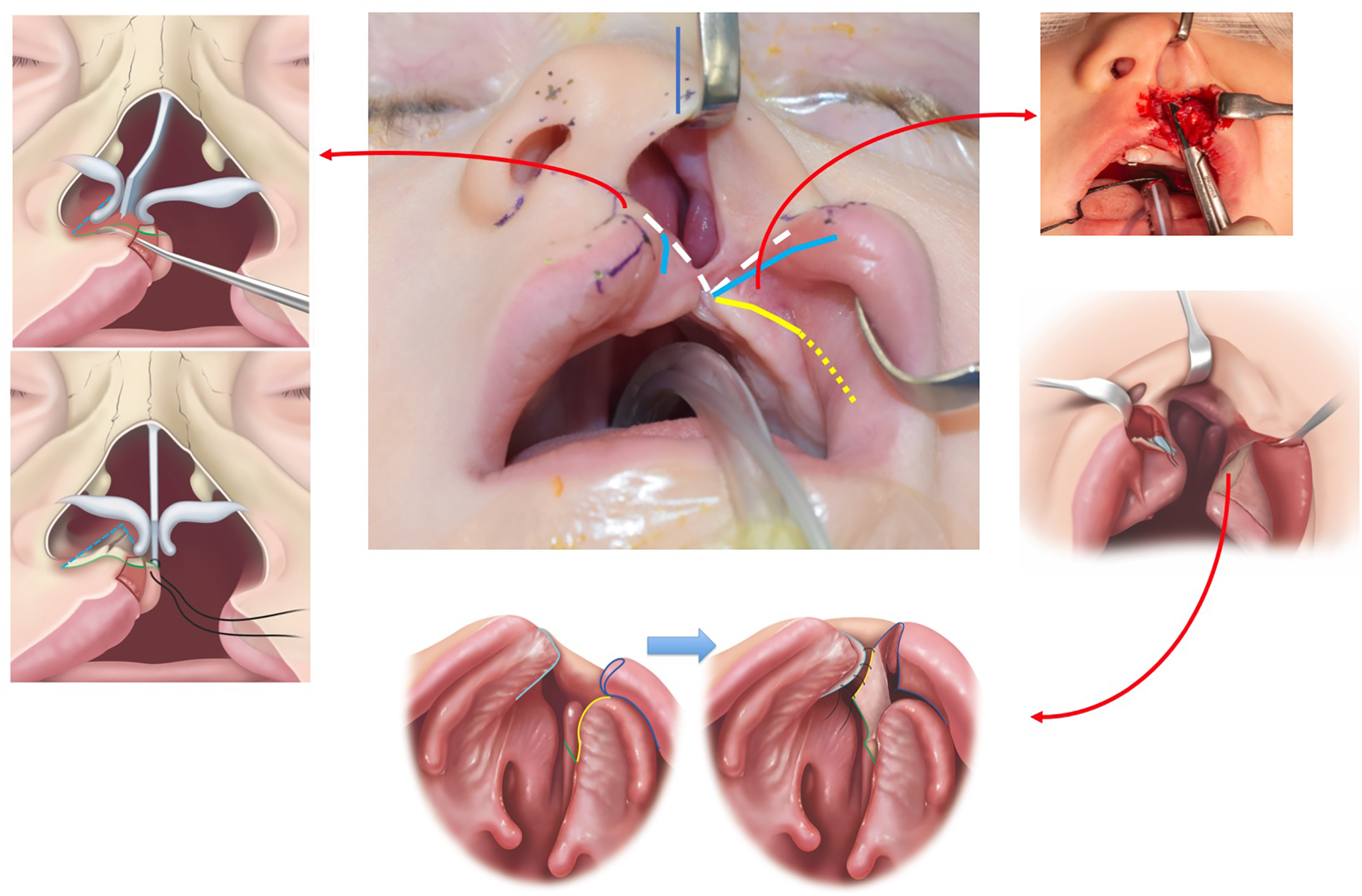
Foundation-based primary rhinoplasty. The septum is released from the anterior nasal spine and nasal floor so that it can be centralized to midline. An upper buccal sulcus incision with supraperiosteal dissection over the anterior maxilla and subperiosteal dissection along the lateral nasal sidewall. A back cut in the mucoperiosteum allows the flap to be advanced en-block with the ala. The flap is inset into the septum to produce a nasal floor. (Modified with permission from Tse RW, Mercan E, Fisher DM, Hopper RA, Birgfeld CB, Gruss JS. Unilateral Cleft Lip Nasal Deformity: Foundation-Based Approach to Primary Rhinoplasty. Plast Reconstr Surg. 2019;144(5):1138-1149).
The lateral lip incision provides access to the piriform aperture. Supraperiosteal dissection frees the alar base and ensures that the accessory chain of cartilages is freed from the piriform rim. If the alar base needs further mobilization, supraperiosteal release over the anterior maxilla and zygomatic body is performed. If the nasal floor is intact (ie, incomplete clefts), the selected points of nasal closure are brought together using a wedge excision that is tapered posteriorly.
If the cleft alar base can't be adequately advanced to a balanced position relative to the non-cleft side or the cleft extends through the nasal floor, the lateral nasal sidewall is advanced (Figure 8). Through the prior anterior maxillary dissection, the periosteum along the piriform aperture is incised so that a subperiosteal plane can be established along the nasal vault of the lesser segment extending from the palatal shelf to base of inferior turbinate. Scissors are used to incise the mucoperiosteum along the palatal shelf and a releasing incision is made along the mid-hard palate extending up to the base of the turbinate. Mucoperiosteum of the lateral nasal wall can then be advanced in continuity with the ala, leaving the flap donor site posterior to the piriform aperture, along the bony nasal vault. The mucoperiosteum can then be inset into a counter incision along the vomer/septum to create a nasal floor. Closure progresses from posterior to anterior so that the 2 points of nasal closure are eventually aligned. The planned points of nasal closure can be adjusted as needed given that following closure, the alar base positions should be balanced and symmetric, especially when the incised lip elements are manually approximated.
Nasal tip and ala contour can then be adjusted as needed. Using a retractor to elevate the cleft side dome, the lower lateral cartilage is repositioned over caudal edge of the upper lateral cartilage thereby establishing a more correct scroll configuration (Figure 9a). One or 2 horizontal mattress sutures are used to secure the cartilages. Alar transfixion sutures are placed to lateralize the vestibular tissue, stabilize the new alar base position, and accentuate the external alar crease (Figure 9b).

Nasal suture. (a) Internal nasal valve plication. An elevator lifts the lower lateral cartilage so that it sits on top of the caudal margin of upper lateral cartilage. Horizontal mattress sutures secure the cartilage in place. (Reproduced with permission from Tse RW, Fisher DM. Anatomic subunit approximation to unilateral cleft lip repair. In: Neligan P, ed. Plastic Surgery, fifth edition. Elsevier. ISBN 9780323810371; In print). Nasal suture. (b) Alar transfixtion. Sutures are placed to lateralize the vestibular skin, support the new position of the ala, and to accentuate the lateral alar crease. (Reproduced with permission from Tse RW, Fisher DM. Anatomic subunit approximation to unilateral cleft lip repair. In: Neligan P, ed. Plastic Surgery, fifth edition. Elsevier. ISBN 9780323810371; In print).
Lip Approximation
Closure progresses from the posterior to anterior layers with inset from superior to inferior, thereby providing access for accurate suture placement and minimizing distortion that can occur when retracting tissues.
Lateral lip mucosa is approximated to the medial lip mucosa.
Muscle repair follows. The tension and manner of muscle inset can have a profound effect on nasolabial balance. Muscle that was previously delaminated from the cleft alar vestibule is inset into the void at the base of the columella. Although this inset is often described as a medial advancement of the lateral lip muscle, in reality, the tension of the inset produces almost the opposite. With muscle inset, the columella and non-cleft alar base shift medial while the cleft alar base is supported in its new anterior position. Tension on inset “balances” nasolabial form and is perhaps one of the most critical parts of the repair. As the muscle inset progresses caudally, there should be less tension, thereby allowing the intricate “J” shape of the orbicularis muscle on each side to be approximated (Figure 10). Any distortion of the natural muscle shape is avoided so that the natural 3D pouting form of the lip can be preserved.

Component approximation. The orbicularis oris muscle has an intricate shape that should be preserved in order to maintain the pout of the lip. Inset progresses from deep to superficial and superior to inferior so the “J” shape of the orbicularis muscle can be preserved and aligned across the repair. There may be some tension of cutaneous repair just above the cutaneous roll which can help to maintain the lip pout. (Reproduced with permission from Tse RW, Fisher DM. Anatomic subunit approximation to unilateral cleft lip repair. In: Neligan P, ed. Plastic Surgery, fifth edition. Elsevier. ISBN 9780323810371; In print).
Skin inset follows with a minimal number of deep dermal sutures and final surface inset. Final adjustments can be made at this stage to fine tune the repair.
Pearls
Noordhoff point is considered a fixed anatomic landmark. Deficiencies in lateral lip height are addressed by altering the configuration of the design rather than sacrificing lip width by moving the point of lip closure further lateral. The latter discards excess tissue, produces greater tension, and thins the lip.
Beware of making Cupid's bow too wide. The peaks are identified along the medial border of philtral ridge. This reduces the philtral height discrepancy and ultimately produces a more natural form.
If the lateral lip is tall (ie, incomplete clefts), excision of vertical excess may be needed to allow medial and lateral elements to “dock” together and to avoid cephalic displacement of the cleft alar base. The excision is similar to that performed with rotation-advancement repairs but is pre-measured.
Defining accurate points of nasal closure is critical but also difficult. While the landmarks and measurements are intended to facilitate design, the overall appearance when those points are brought together ultimately dictates the outcome. Check, recheck, and adjust through the course of design and repair.
The best predictor of long-term outcome is the final appearance, balance, and harmony in the operating room. While landmarks and measurements serve to facilitate, an astute surgeon's judgement is ultimately the more sensitive tool. Trust your “eye” over anything else, use checkpoints to verify progress, and don't leave the operating room unless the best balance has been achieved. The first time is the best time.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This article does not contain any studies with human or animal subjects.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.