
Abstract
When intraorbital wooden foreign bodies are missed, the consequences can be devastating. While the gold standard diagnostic imaging is computed tomography (CT), it has low sensitivity. We present a 61-year-old man with a bamboo injury to his right eye. He underwent two CT scans that failed to raise the possibility of intraorbital foreign bodies. Upon additional review, a rectangular-shaped pocket of air was identified in the orbit which was most consistent with wooden foreign bodies based on the clinical history. A combined mid-lid approach followed by a transconjunctival and transcaruncular extension were employed to remove several wooden splinters. Postoperatively, due to recurrent orbital compartment syndrome, he required a second decompression with an inferior rim osteotomy. He had good recovery at 3 months follow-up. Overall, intraorbital wooden foreign bodies are challenging to diagnose due to imaging limitations. Providing a clear history and suspected diagnosis to radiology is critical for diagnosis.
A 61-year-old male presented to a local emergency department after a bamboo pole struck his right eye during gardening. Computed tomography (CT) showed air and soft tissue swelling in the medial orbit and possible undisplaced medial wall fracture.
He was transferred to our tertiary trauma center with diplopia, pain, total ophthalmoplegia, 20/50 vision, and increased intraocular pressure (IOP) of 42 mm Hg, with no relative afferent pupillary defect (RAPD). Based on imaging, he was diagnosed with orbital emphysema of unclear etiology and was treated with IOP-lowering drops.
Next day, the plastic surgery team noticed a 1.5 cm laceration to the lower eyelid and a new RAPD (Figure 1). CT facial bones did not report a foreign body. However, a careful review of the images revealed a sharply demarcated rectangular radiolucency, differing from surrounding areas of emphysema along the medial extraconal compartment. Given this anomalous finding and high clinical suspicion, neuroradiology was re-consulted. Foreign bodies were noticed, measuring 2.3 × 8.7 cm along the inferomedial aspect of the orbit by the medial rectus (Figure 2A and B). Lateral canthotomy and inferior cantholysis were performed to prevent orbital compartment syndrome.

Extraocular movement of the patient at presentation, demonstrating chemosis, swelling, and total ophthalmoplegia in the right eye.
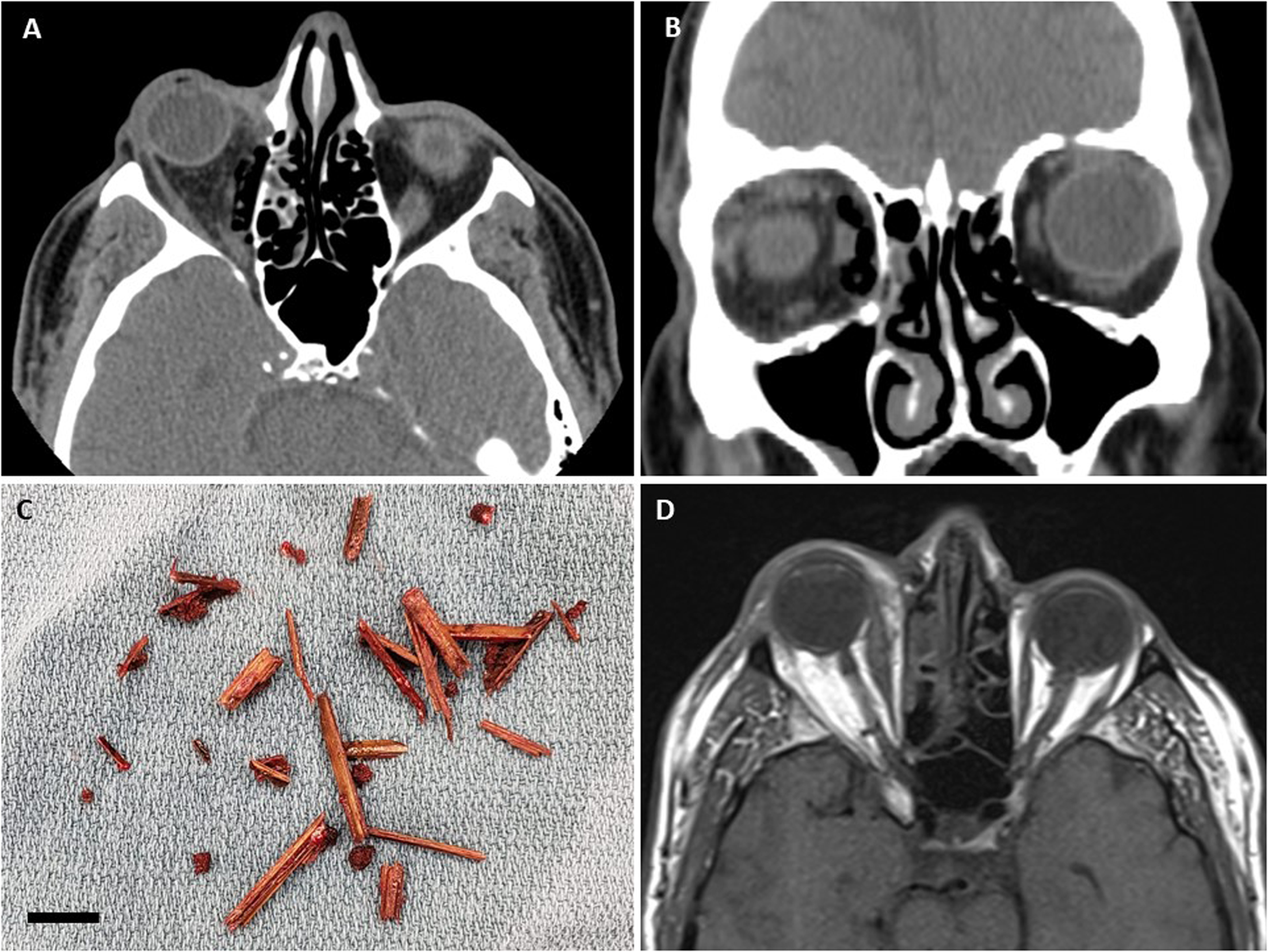
(A) Transverse and (B) coronal view of computed tomography images of the patient pre-operation, showing a well-defined geometric emphysema in the right orbit with multiple air locules, measuring 2.3 × 8.7 cm along the inferomedial aspect of the right orbit adjacent to the medial rectus muscle. (C) Wooden splinters removed from the patient's orbit during a transconjunctival peritomy. The bar indicates 1 cm. (D) Transverse view of the magnetic resonance imaging of the patient post-first operation, showing attenuation of the right optic nerve, profound swelling in the inferomedial aspect of the orbit, and significant proptosis, but no evidence of retained foreign body.
He underwent right orbital decompression and foreign body evacuation. A mid-lid approach was used, incorporating the existing laceration to follow the presumed penetration trajectory. However, no foreign body was visualized. A transconjunctival approach with transcaruncular extension provided wider access to the inferomedial orbit. Small, disintegrated pieces of wood were visualized in the medial rectus (Figure 2C).
Patient's proptosis and RAPD improved the following day. MRI showed small foci abutting the medial rectus, representing air or residual wood (Figure 2D). Later, he developed worsened vision, increased IOP to 52, and RAPD. Due to concern for orbital compartment syndrome, urgent repeat decompression and orbital osteotomy were performed. No further foreign bodies were found.
Over the next week his symptoms improved (Figure 3). Repeat CT and MRI showed no evidence of residual foreign bodies. After 3 months, his diplopia and partial ophthalmoplegia persisted but all other symptoms resolved (Figure 4).
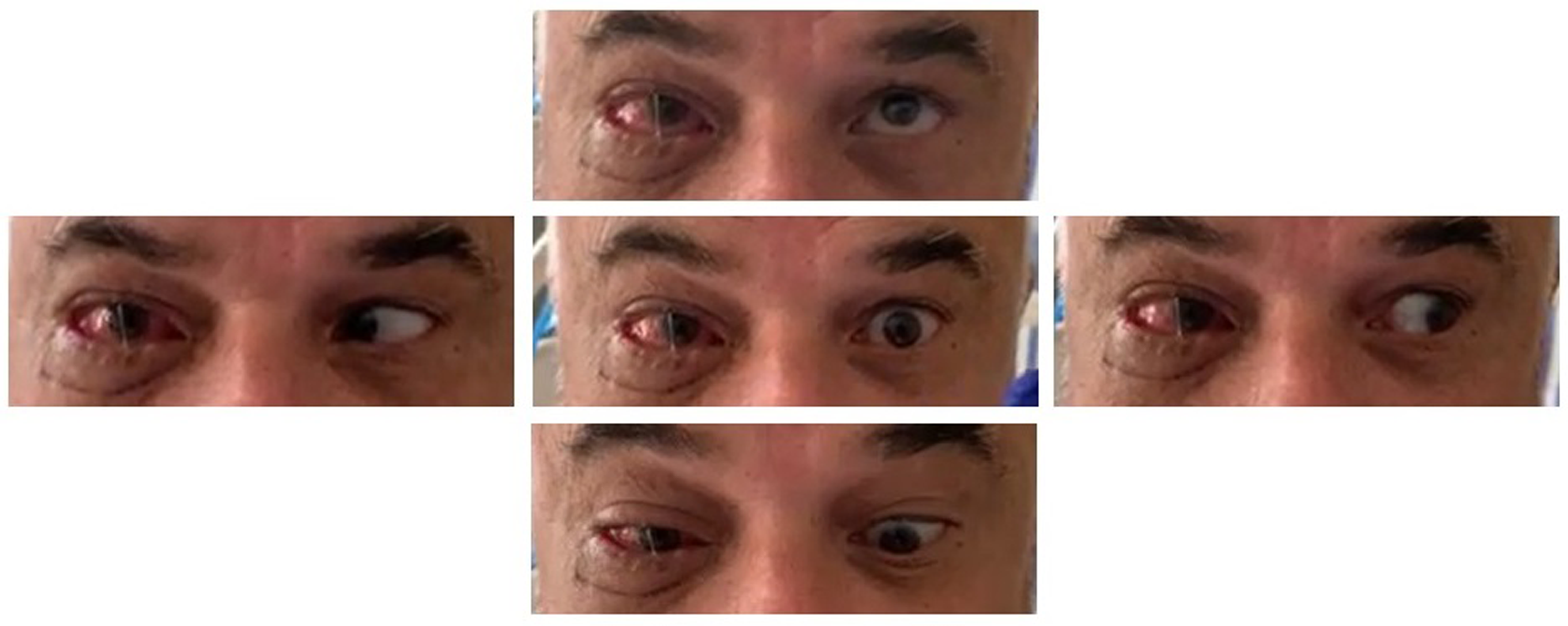
Extraocular movement of the patient after the second operation, demonstrating improved ophthalmoplegia in the right eye.
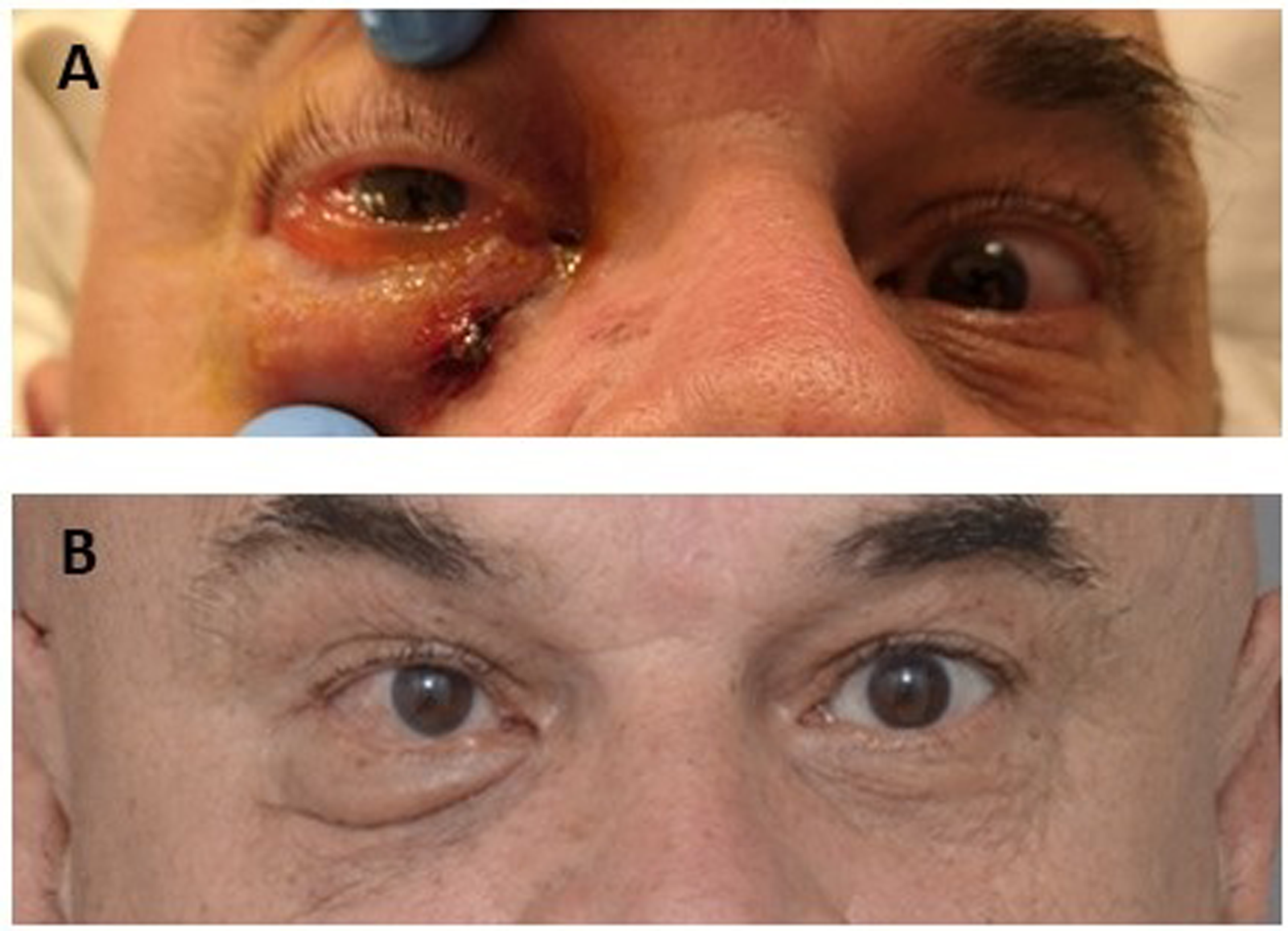
Pictures (A) at presentation and (B) at the 3-month follow-up.
Discussion
Retained intraorbital wooden foreign bodies are difficult to diagnose and patient presentations are variable. 1 Wood contains many bacteria due to its porous texture which lead to abscess and fistula formation, requiring prompt diagnosis and surgical removal. 2
Choosing the appropriate diagnostic imaging modality is challenging. X-ray is inaccurate, and ultrasound is inconsistent and operator-dependent. 3 MRI offers better detection with findings including hypointensity on T1 and ring enhancement with contrast, although these are not always present and urgent MRIs can be difficult to obtain. 4 Currently, CT scan remains the gold standard but it has inconsistent reported detection rates ranging from 42% to 72%.1,2,5–7 The type of wood, density, and freshness leads to variable signal densities on CT. 8
Wooden foreign bodies in the orbit are challenging to diagnose and easily missed on imaging. A clear history with the presumed clinical diagnosis should be provided to radiology for careful assessment of images. Surgical evacuation through the original wound should be the initial approach but other decompressive methods may be performed if exposure is inadequate.
Footnotes
Author Contributions
All authors made substantial contribution to the conception and design of this work, along with critical revision of the manuscript and approval of the final version for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent for information and images to be published was provided by the patient.