
Abstract
Degloving injuries of the thumb pose a significant challenge as replantation is usually unsuccessful. A 60-year-old man was transferred to “Queen Victoria Hospital NHS Trust” four hours after having his left thumb completely avulsed at metacarpophalangeal level. The anastomosis repeatedly failed during urgent replantation and a distally based pedicled RFF was utilized. To achieve accurate flap design, we used the amputated part as a template for the missing tissue. After a longitudinal cut exposing the inner surface, the thumb was placed flat on top of a clean gauze package which was used as a paper template for the skin paddle; the flap was subsequently sutured without tension. Since the circumferential soft tissue envelope is three-dimensional, accurate designing of the flap on the forearm is vital. We propose a useful technique using the amputated part to enable a precise estimation of the tissue requirements to reduce potential complications related to flap inset.
Introduction
Degloving injuries of the thumb pose a significant reconstructive challenge. 1 When the avulsed part is preserved there is potential for emergency microsurgical reconstruction; however, replantation most of the times is technically unsuccessful, particularly if there is a complete avulsion of the distal part. The reverse-flow radial forearm fasciocutaneous flap is a well-described option in the plastic surgeon's toolbox, because the forearm offers adequate, thin soft tissue to cover a circumferential defect of the thumb. This technical report describes a useful yet simple way to achieve accurate skin paddle markings.
Methods
A 60-year-old man sustained a degloving injury of his left thumb while using a mechanical lathe. His past medical history included poorly controlled type II diabetes mellitus, obesity, and obstructive sleep apnea. The thumb was completely avulsed at the metacarpophalangeal level; the amputated part consisted of circumferential soft tissue with an incorporated tuft fragment and the degloved stump suffered a fracture at the proximal shaft of the distal phalanx.
The patient was urgently transferred to the “Queen Victoria Hospital NHS Trust” four hours after the injury, along with the correctly preserved amputated part. He was taken directly to theater for attempted replantation under axillary block as he was deemed high risk for general anesthesia. The exploration revealed a damaged proximal arterial stump, and the first dorsal metacarpal artery, which had adequate length and good flow, was selected as a recipient vessel. However, despite achieving some flow initially, the anastomosis repeatedly failed. The patient was taken to the theater the following day for a soft tissue reconstruction with a distally based pedicled RFF. Allen's test was performed with the patient on the operating table, hand perfusion was evaluated, and ulnar artery flow was checked with a handheld Doppler. The radial artery and cephalic vein were marked from wrist to antecubital fossa, and the intended pivot point of the pedicle was placed approximately one centimeter proximal to the distal wrist crease.
Results
To achieve an accurate flap design, we decided to use the amputated part as a template for the missing soft tissue. In this context, we proceeded to a longitudinal cut of the thumb exposing the inner surface. Using a clean gauze package, the amputated part was placed flat on top of the paper and used a template for the skin paddle; this template has been purposely created slightly wider than the physical margins of the amputated part homogenously on its periphery to allow the tension-free closure, and a spearhead-shaped extension was added distally to accommodate the vascular pedicle (Figure 1). The paper outline was used to confirm the necessary cover of the thumb, and subsequently placed on the forearm to outline the flap's skin paddle (Figure 2).
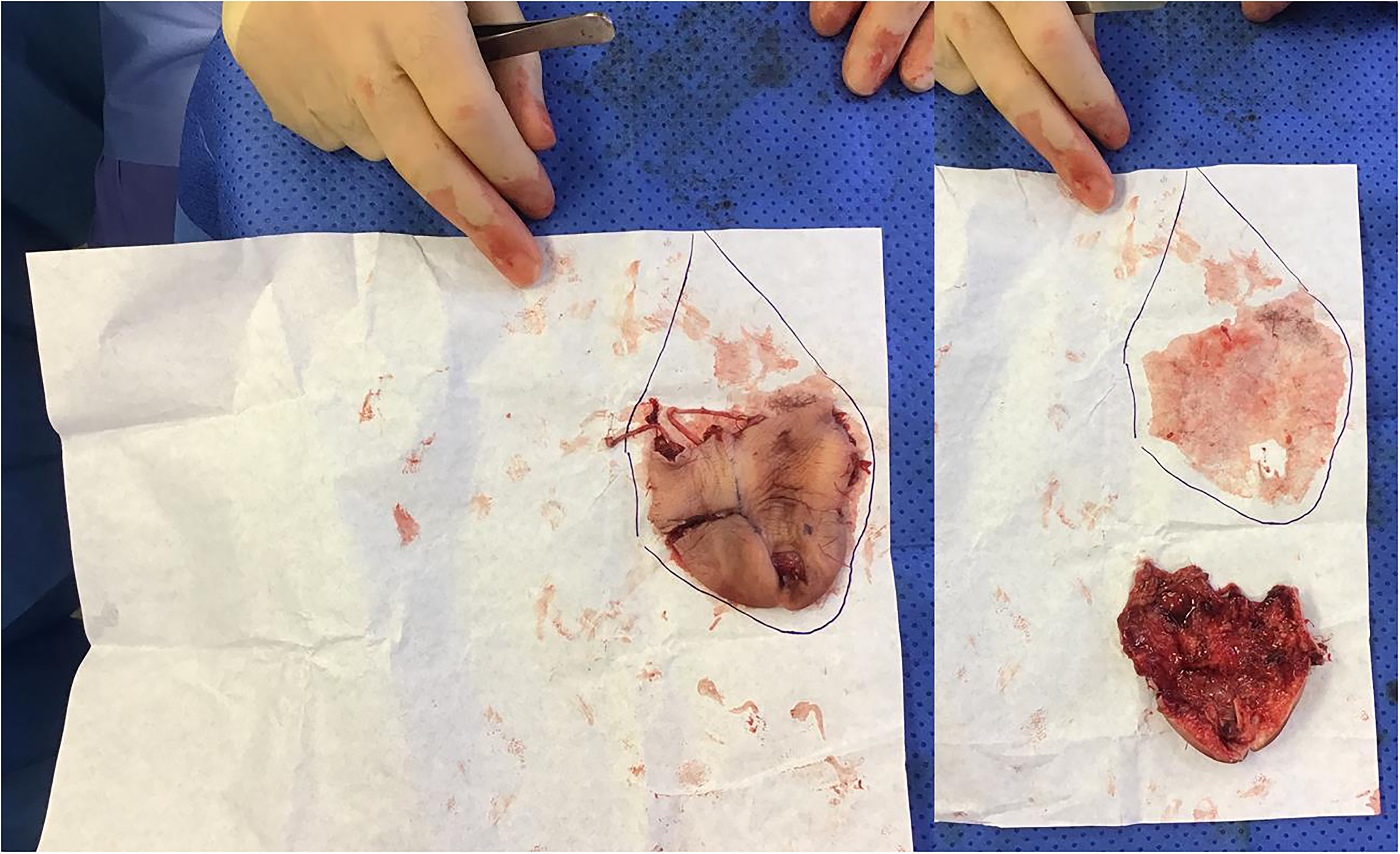
Design of a paper template for the flap's skin paddle with the use of the longitudinally cut amputated soft tissue envelope of the thumb.

The paper template was used to confirm the adequate cover of the thumb (upper photo) and the design of the flap's skin paddle (lower photo).
The flap was harvested in the usual manner. Initially, we elevated the pedicle's ulnar border over the paratenon distally and the epimysium of the flexor carpal radialis proximally. We proceeded radially with the identification of the cephalic vein, which was included in the pedicle. The cutaneous branches of the superficial radial nerve were preserved, and radial artery was visualized in the lateral intramuscular septum; it was then clamped with a 2-A vascular clamp proximally, and the perfusion of hand and flap was assessed after tourniquet release. The pedicle was ligated proximally and flap's elevation was completed from proximal to distal. The intervening skin bridge after the pivot point at the posterolateral aspect of the hand was divided and re-sutured without tension over the pedicle. The donor site defect was reconstructed with a split-thickness skin graft harvested from the right lateral thigh (Figure 3). The patient was discharged on the second postoperative day and the flap was settling well and all wounds were healing well at the two week follow-up review.
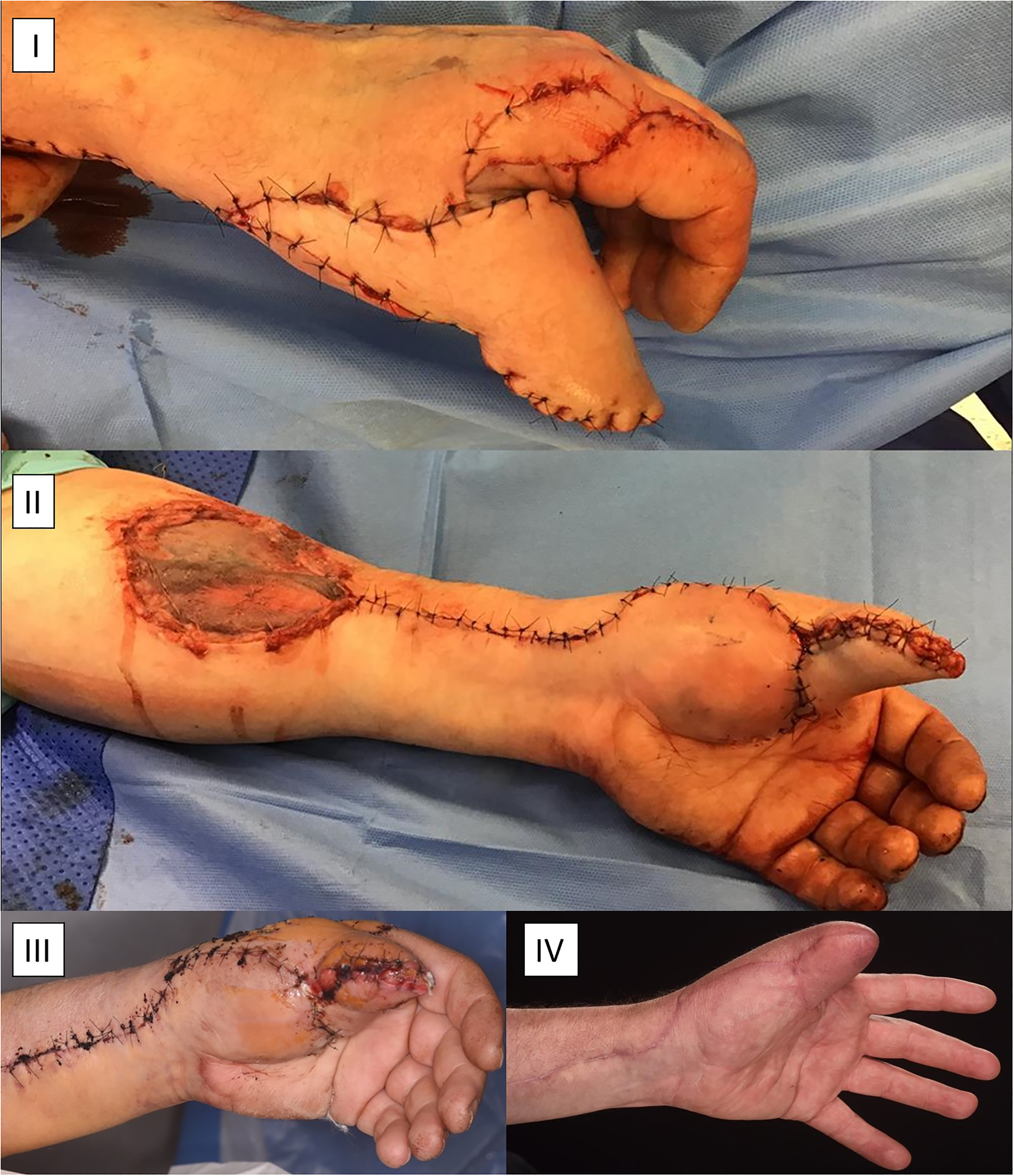
Flap inset for excellent thumb cover with reconstruction of the donor site with a split-thickness skin graft (I, II), and follow-up healing progress after one week (III) and eight months (IV).
Discussion
The radial forearm retrograde-flow pedicled flap for hand reconstruction was described by Lu et al 1 in 1982, one year after the initial introduction of the free radial forearm “Chinese” flap. 2 Generally, the use of the same surgical field, the robust blood supply and the thin and pliable nature of the forearm fasciocutaneous tissue, and the avoidance of microvascular anastomosis, have been regarded as strengths of the pedicled radial forearm flap for hand reconstruction, 3 particularly with demanding reconstructive cases including degloving and ring avulsion injuries, 4 where replantation of the soft tissue envelope enjoys a low success rate due to the significant contusion of the amputated tissue and the elongation derived intimal shearing of its vessels.5,6 The disadvantages of the reverse-flow RF flap are the sacrifice of a significant inflow hand vessel, the use of hair-bearing and insensate skin for a non-articulated thumb, and the unsightly grafted donor site.7,8 Further suggested refinements in the flap harvest to improve the aesthetic and functional outcome include using a sensate 9 or an osseocutaneous 10 RF flap for thumb reconstruction.
The accurate design of the flap for the thumb reconstruction is a vital component of operative planning. Several variations for optimization of flap design have been proposed, 11 including the use of an oblique skin paddle design to offer a longer pedicle and arc of rotation, 12 a butterfly shape to provide adequate padding to the tip, 13 and longitudinal splitting of the skin paddle for bifid insetting. 14 However, since the circumferential soft tissue envelope is three-dimensional, designing the flap on the forearm is not straightforward. There is significant risk of underestimating the circumferential thumb defect and harvesting too small a flap that could result in a tight inset; in contrast, an overly cautious approach could lead to a fasciocutaneous tissue surplus to the requirements and a larger residual donor site defect, and risk flap necrosis.
This paper proposes a useful way to overcome difficulties with flap design by using the amputated part to design an exact match for the defect. As shown in the included figures, the amputated soft tissue envelope is transformed with a longitudinal incision to a monodimensional model easily transposed onto a paper template; the flap was subsequently sutured without any tension on the reconstructed thumb. This technique does not prolong the operation but, on the contrary, enables precise estimation of the tissue requirements to reduce adverse complications related to flap inset.
Footnotes
Authors’ Note
There has been no previous study-related presentation and publication to the submitted paper. Patient signed informed consent regarding publishing their data and photographs and has consented to the submission of the case report to the journal. All authors participated in the presented case report and contributed to this study. Dr G. Christopoulos was the main author of the paper and Mr Thomson assisted in the collection of all the relevant information. Mr M. E. Jones was the lead surgeon and contributed as a senior author with the general overview and the final refinements.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.